

Abstract
Substantial evidence points to the presence of subtle weaknesses in the nonlinguistic cognitive processing skills of children with primary (or specific) language impairment (PLI). It is possible that these weaknesses contribute to the language learning difficulties that characterize PLI, and that treating them can improve language skills. To test this premise, we treated two nonlinguistic cognitive processing skills, processing speed and sustained selective attention, in two Spanish–English bilingual children with PLI. The study followed a single-subject multiple baseline design, with both repeated measures and standardized pre- and post-testing as outcome measures. Results from the repeated measures tasks showed that both participants made gains in nonlinguistic cognitive processing skills as well as in Spanish and English. These results both replicate and extend prior work showing that non-linguistic cognitive processing treatment can positively affect language skills in children with PLI.
Keywords: specific language impairment, bilingualism, children, nonlinguistic cognitive treatment
The relationship between cognition and language in children with primary language impairment (PLI) is a source of spirited debate (e.g. Kohnert & Ebert, 2010). PLI is a developmental disorder characterized by language delays without associated intellectual, hearing, neurological or psychological disorders. Given the apparent isolation of the language deficits, the disorder is often labeled as specific language impairment. However, an in-depth examination of the cognitive processing skills of children with PLI reveals the presence of subtle, subclinical deficits. In other words, evidence has amassed that, despite performing within the average range on a test of nonverbal intelligence, children with PLI perform below their peers on tasks that tap a variety of nonlinguistic cognitive processing skills.
In a previous work (Ebert & Kohnert, 2009), we have examined the effects of treating these nonlinguistic cognitive processing skills in order to gain insight into the relationship between nonlinguistic cognitive processing and language skills in children with PLI. If cognitive processing deficits contribute to language learning delays in PLI, improvements in these processing skills should positively affect language. Here, we extend this line of reasoning by applying nonlinguistic cognitive processing treatment to bilingual children with PLI; if language gains result from treating nonlinguistic cognitive processing skills, then these gains should appear in both languages spoken by bilingual children. This investigative line also presents an exciting opportunity to improve treatment outcomes for bilingual children with PLI.
We begin by reviewing the evidence for nonlinguistic cognitive processing weaknesses in children with PLI. This leads to a description of the previous work investigating treatment of nonlinguistic cognitive processing skills and its results. Finally, we motivate the current study by examining the challenges and opportunities presented by the population of bilingual children with PLI.
Information Processing Skills in Children with PLI
Evidence of nonlinguistic cognitive processing deficits in children with PLI has increased in the recent years. Three lines of research can be distinguished within this evidence base; each line establishes the presence of a subtle cognitive processing deficit in the population of children with PLI. In addition, all three areas of weakness encompass processing nonlinguistic as well as linguistic information.
The first line of research concerns speed of processing. Evidence indicates that children with PLI process information more slowly than their typically developing (TD) peers (for reviews, see Kohnert, Windsor, & Ebert, 2009; Ullman & Pierpont, 2005). Slowed processing is apparent on a variety of linguistic and nonlinguistic tasks, including naming pictures, making lexical judgments, mentally rotating geometric shapes (Windsor, Kohnert, Loxtercamp, & Kan, 2008), completing addition problems (Fazio, 1999), and detecting colored shapes or auditory tones (Fazio, 1999; Kohnert & Windsor, 2004; Miller, Kail, Leonard, & Tomblin, 2001; Windsor & Kohnert, 2004; Windsor, Kohnert, Loxtercamp, & Kan, 2008). Furthermore, the speed of processing nonlinguistic, as well as linguistic stimuli, contributes uniquely to a higher level of language performance in children with and without PLI (Leonard et al., 2007).
The second line of research concerns working memory. Children with PLI generally demonstrate deficits in comparison to TD peers on tasks thought to tap working memory. Verbal working memory is hypothesized to be a key deficit in the PLI profile (e.g. Gathercole, 2006; Montgomery, Magimairaj, & Finney, 2010). For example, children with PLI have marked deficits on nonword repetition (Graf Estes, Evans, & Else-Quest, 2006) and sentence span tasks (Ellis Weismer, Evans, & Hesketh, 1999). Importantly, working memory deficits in PLI also extend beyond language. Children with PLI have difficulty in both spatial (Hoffman & Gillam, 2004) and auditory working memory tasks (Yim, Kohnert, & Windsor, 2005) that employ nonlinguistic stimuli. As with processing speed, factor analysis supports the separate contributions of verbal and nonverbal working memory abilities in children with PLI (Leonard et al., 2007).
Finally, recent evidence suggests that reduced attention is another nonlinguistic cognitive processing weakness in the PLI profile. Attention is a basic cognitive construct that has been conceptualized in many different ways. Subclinical deficits in the attention skills of children with PLI have been uncovered according to several of these conceptualizations. PLI has been associated with weak controlled attention skills (Marton, 2008), decreased attentional capacity (Montgomery, Evans, & Gillam, 2009), and deficits in sustained and selective attention (Finneran, Francis, & Leonard, 2009; Spaulding, Plante, & Vance, 2008). Meta-analytic evidence points to a significant gap between the performance of children with PLI and that of their TD peers on Continuous Performance Tasks, a prototypical assessment of sustained and selective attention (Ebert & Kohnert, 2011). This meta-analysis also established that sustained and selective attention deficits in children with PLI are present in both the auditory and visual domains, as measured with tasks that use linguistic as well as nonlinguistic stimuli.
Treating Cognitive Processing Weaknesses
The extant evidence clearly supports the presence of subclinical weaknesses in processing speed, working memory and attention in the PLI profile. It is possible that these weaknesses, individually or in combination, impede language learning and thus contribute causally to the salient language deficits in PLI (e.g. Kohnert & Ebert, 2010; Leonard et al., 2007). If there is a causal (versus simply correlated) association between the subtle nonlinguistic processing weaknesses and language abilities in children with PLI, then modifying these basic cognitive processing skills could enhance language treatment outcomes. The concept of improving language skills via treatment of underlying nonlinguistic cognitive processing skills is not entirely new. Diverse groups of children (including children with PLI, TD children, at-risk populations and children with cognitive delays) were treated with training programs based on the Illinois test of psycholinguistic abilities (Kirk, McCarthy, & Kirk, 1968). These programs targeted a wide range of psycholinguistic skills using both linguistic and nonlinguistic stimuli. Results of these trials were mixed (Hammill & Larsen, 1978). More recently, Tallal et al. (1996) have developed software based on the hypothesis that the ability to process rapidly changing auditory information, such as the formant transitions apparent in natural speech, is impaired in PLI. Once again, the effects of this treatment have been disputed (Gillam et al., 2008).
At the same time, treatments for children with PLI based specifically on evidence of impaired processing speed, working memory and attention have not been thoroughly investigated. Authors of some recent studies speculated that gains following intensive language treatments for PLI were driven in part by gains in attention (Gillam, Crawford, Gale, & Hoffman, 2001; Gillam et al., 2008). However, these studies did not include a measure of attention to directly investigate this possibility. One treatment study (Stevens, Fanning, Coch, Sanders, & Neville, 2008) documented improvements in selective attention both before and after intensive language treatment using event-related potentials (ERPs). ERPs offer a physiological measure of attention that may in fact be more sensitive than behavioral outcomes; however, behavioral measures of attention were not included in the study, leaving open the question of how intensive treatment may affect observable indices of attention in children with PLI.
In Ebert and Kohnert (2009), we provided preliminary evidence that treating nonlinguistic processing speed and memory skills could improve some aspects of language in school-age children with PLI. Ebert and Kohnert (2009) used single-subject experimental design (SSED) to demonstrate treatment effects for two monolingual, English-speaking children with severe PLI. As with the current project, Ebert and Kohnert (2009) used both repeated-dependent measures and standardized pre- and post-testing to determine treatment effectiveness. Following an intensive treatment protocol spanning a 4-week period, both participants demonstrated large improvements in standardized scores for global language and expressive vocabulary; global language gains were driven primarily by improvements in sentence formulation and production of grammatical morphemes. Naming speed also improved substantially for both participants throughout the treatment period. The results did not, however, support notable changes in memory or receptive language, at least during the short period of the study. Furthermore, it is possible that social interactions with the therapist contributed to language improvements; although all treatment activities used nonlinguistic stimuli, children still received some linguistic stimulation through normal interaction with the therapist.
Bilingualism and PLI
A significant portion of children in many Western countries learn a minority home language from birth (L1) (e.g. Turkish in Germany, Punjabi in England, Spanish in the USA) and the majority community language (L2) (e.g. German or English) in childhood with attendance in educational programs. Although the vast majority of these sequential bilinguals are typical learners, as with monolingual learners, a subset will struggle with both languages for no readily apparent reason. Sequential bilingual children with PLI are recognized as a uniquely challenging population for speech-language therapists (e.g. Caesar & Kohler, 2007; Kohnert, 2007, 2010; Royal College of Speech and Language Therapists Special Interest Group in Bilingualism, 2007).
Unfortunately, evidence of effective treatment for bilingual children with communication disorders, including PLI, is extremely scarce (Kohnert & Medina, 2009). The general consensus of expert opinion in the literature is that sole reliance on direct treatment in L2 frequently does not meet the communicative needs of bilingual children (e.g. Kohnert, 2010; Royal College of Speech and Language Therapists Special Interest Group in Bilingualism, 2007). Instead, practitioners should take active steps to support L1 as well as L2. There may be many ways to promote L1 growth, including direct treatment of L1, in the relatively rare cases when there is a match between client and clinician languages; selecting treatment targets to facilitate cross-linguistic transfer using technology, and incorporating L1 speakers (such as family members, peers, trained support personnel or interpreters) into therapy (e.g. Kelley & Kohnert, 2012; Kohnert, Yim, Nett, Kan, & Duran, 2005; Pham, Kohnert, & Mann, 2011).
The current study investigates the feasibility of alternative means to support growth in both L1 and L2 for bilingual children with PLI. If processing speed, working memory and attention skills contribute to the language learning difficulties that characterize PLI, improving these cognitive skills could lead to gains in both L1 and L2, given continued meaningful experiences in each language. The inclusion of bilingual children also provides a unique vantage point for testing the theoretical claim that nonlinguistic cognitive processing weaknesses contribute to PLI, because the effects of social interaction can be separated from the effects of treatment activities. That is, gains that stem from improvements in processing speed, working memory or attention should appear in both L1 and L2, whereas gains that stem from peripheral aspects of treatment should be more apparent in the language of treatment interactions.
Study Purpose and Design
The purpose of this study was to use SSED to test the hypothesis that treating nonlinguistic cognitive processing weaknesses could improve the L1 and L2 skills of bilingual children with PLI. Participants are two school-age children who speak Spanish (L1) and English (L2). This study represents both a replication and an extension of previous work investigating the effectiveness of nonlinguistic cognitive processing treatment for two monolingual English-speaking children with PLI (Ebert & Kohnert, 2009). Based on the results of Ebert and Kohnert (2009), the focus of the nonlinguistic cognitive processing treatment program was shifted slightly, away from working memory and toward sustained and selective attention. The resulting treatment program uses nonlinguistic stimuli to treat processing speed and sustained selective attention. Outcome measures span three areas: nonlinguistic cognitive processing, L1 and L2. Gains across all three areas would support the hypothesis that nonlinguistic cognitive processing weaknesses contribute to PLI and can provide a foothold for effective clinical treatment with bilingual school-age children.
We used a multiple baseline SSED across participants. In this design, each participant completes a baseline phase (without intervention) followed by treatment. Tasks hypothesized to measure the skills targeted by treatment are administered repeatedly throughout both baseline and treatment phases. Treatment effects are established when these repeated measures remain relatively stable during the baseline phase and improve during the treatment phase for each participant (e.g. McReynolds & Thompson, 1986). A variety of features – including using objective measures, assessing skills repeatedly, treating stable problems and including multiple cases – strengthen the inferences that can be drawn from such data beyond what can be inferred from a case study (Kazdin, 1981). Ideally, multiple-baseline designs will contain at least three separate baselines (or three participants, in the case of multiple-baseline across participants); however, the presence of two baselines meets the minimum criteria for the design (Kazdin, 1981). SSEDs are considered Level 2 evidence in many hierarchies that rank the quality of treatment evidence from highest to lowest (e.g. Gillam & Gillam, 2006); they also make up a substantial portion of the evidence for treatment efficacy in children with developmental communication disorders (e.g. Baker & McLeod, 2011; Cirrin & Gillam, 2008).
In addition to the baseline and treatment phases that are characteristic of SSED, pre- and post-treatment test phases were included in this study. The purpose of pre- and post-treatment testing here was to provide additional information about L1 (Spanish) and L2 (English) skills using standardized, norm-referenced language assessments in Spanish and English. Such standardized measures also provide indices of change that are more accessible to many clinical professionals.
Methods
Participants
Two Spanish–English bilingual boys with PLI participated in the study. The first participant (P1) was aged 8;4 when the study began and the second participant (P2) was aged 7;5. Both children spoke Spanish in the home per parent and child report. The children attended public schools in a large metropolitan upper Midwest school district in the USA that provided instruction in English. Both participants had qualified for ongoing school-based services for PLI. During the school year, P1 and P2 received speech-language therapy from a monolingual English-speaking clinician. Because the study was conducted during the summer, the participants were not receiving any other speech-language therapy at the time this study was conducted.
Both participants had a clinical referral from their school speech-language therapist. The minimum criterion for a clinical diagnosis of PLI in bilingual learners is significantly low performance in both languages on a minimum of two standardized and/or criterion-referenced receptive and/or expressive language measures, as compared to age peers with similar language, cultural and educational experiences (Minnesota Office of the Revisor of Statutes, 2008). The language impairment is accompanied by significant academic delays and is not accompanied by frank motor, sensory, intellectual or social-emotional deficits. Both P1 and P2 met these clinical criteria as judged by experienced bilingual clinical speech-language pathologists. In addition, both participants had histories of delayed language onset and family concern, considered an additional significant marker of PLI (cf. Restrepo, 1998).
The clinical referrals for P1 and P2 were confirmed by our bilingual research staff using the following methods: (a) family interview to determine the child’s developmental history and parental concern, (b) review of educational history and current academic status, (c) performance on Spanish and English standardized tests (see also section on Measures), (d) a hearing screening conducted at 20 dBHL at 500, 1000, 2000 and 4000 Hz, and (e) the Test of Nonverbal Intelligence – 3rd Edition (TONI-3; Brown, Sherbenou, & Johnsen, 1997).
Although both participants shared a home language and a diagnosis of PLI, they presented with notably different profiles. (See Table III for standardized pre-treatment language testing scores for P1 and P2.) For example, on the TONI-3, both participants scored well above the cut-off used to determine intellectual impairment, yet the two scores were quite different. P1 scored in the high average range (standard score = 115, one full standard deviation above the published mean) and P2 scored within one standard deviation of the mean on the low average side (standard score = 94). P2 demonstrated relatively similar scores on the Spanish and English measures, but overall presented with a more severe language impairment than P1. Both participants demonstrated a relative strength in vocabulary (as compared to more global levels of language, including listening comprehension or formulating grammatical sentences). It is important to note that heterogeneity in terms of relative levels of L1 and L2 ability is endemic to TD bilingual children (e.g. Kohnert, 2010). Similarly, monolingual children with PLI present a wide range of variation in language profiles and symptom severity (e.g. van Weerdenburg, Verhoeven, & van Balkom, 2006). As such it is quite expected the profiles of two bilingual children with PLI would differ substantially, despite both children meeting the same study criteria.
Table III.
Pre- and post-test scores for standardized language tests.
| P1
|
P2
|
|||
|---|---|---|---|---|
| Test | Pre-test | Post-test | Pre-test | Post-test |
| ROWPVT-E | 83 | 84 | 77 | 80 |
| EOWPVT-E | 74 | 74 | 64 | 67 |
| CELF-CD-E | 4 | 6* | 1 | 1 |
| CELF-WS-E | 2 | 6* | 1 | 1 |
| CELF-FS-E | 4 | 4 | 1 | 1 |
| ROWPVT-S | 121 | 115* | 79 | 98* |
| EOWPVT-S | 101 | 100 | 77 | 87* |
| CELF-CD-S | 8 | 9 | 1 | 1 |
| CELF-WS-S | 4 | 5 | 3 | 2 |
| CELF-FS-S | 5 | 5 | 1 | 1 |
| CELF-RS-S | 5 | 5 | 1 | 1 |
Post-test score exceeds the 90% confidence interval surrounding the pre-test score.
Notes: The Recalling Sentences subtest of the English CELF-4 was not administered because the sentences were used for the Sentence Repetition repeated measure in this study. Abbreviations: ROWPVT-E, Receptive One-Word Picture Vocabulary Test, English; EOWPVT-E, Expressive One-Word Picture Vocabulary Test, English; CELF-CD-E, Concepts and Following Directions subtest of CELF-4E; CELF-WS-E, Word Structure subtest of CELF-4E; CELF-FS-E, Formulated Sentences subtest of CELF-4E; ROWPVT-S, Receptive One-Word Picture Vocabulary Test, Spanish-Bilingual Edition; EOWPVT-S, Expressive One-Word Picture Vocabulary Test, Spanish-Bilingual Edition; CELF-CD-S, Concepts and Following Directions subtest of CELF-4S; CELF-WS-S, Word Structure subtest of CELF-4S; CELF-FS-S, Formulated Sentences subtest of CELF-4S; CELF-RS-S, Recalling Sentences subtest of CELF-4S.
Treatment program
The treatment program administered in this study was a brief, intensive intervention designed to improve speed of processing and sustained selective attention without directly treating language. Treatment sessions were scheduled during the participants’ summer school programs. All sessions were conducted at the school site. Sessions were scheduled to occur every day of the summer school program. Summer school in this district is conducted 4 days per week over 5 weeks, excluding holidays, resulting in a total of 19 days of instruction. The time needed for pre- and post-treatment testing reduced the number of possible days of treatment to 14. One participant (P1) attended 13 of 14 treatment sessions. The other, P2 attended only 7 of 14 treatment sessions.
All sessions lasted 90 min, with one 15-min break. The remaining 75 min were divided into five 15-min periods. Typically, these were four treatment activity periods and one period for administering the repeated-dependent measures. On the day each week that repeated measures were not administered (for the purpose of maximizing treatment time), all five periods were devoted to treatment activities.
Six treatment activities were included in the protocol. All six activities used stimuli with minimal linguistic content. That is, children responded to tones, shapes, colors and musical noises rather than words and sentences. All activities were designed to promote faster processing speed and improved sustained attention skills. Participants were instructed to respond as quickly as possible and most games had a time limit for responding correctly. Finally, all activities were also used in prior work on this treatment program (Ebert & Kohnert, 2009).
Three of the six activities were computer games: Change, Scanning and Dominoes. All three are available in the Locutour Multimedia Attention and Memory: Volume II software package (Scarry-Larkin & Price, 2007). The remaining three activities are commercially available games that the participants played together with the clinician. Blink (Staupe, 2001) requires children to sort cards quickly and flexibly depending on the shape, color and number of symbols on the cards; Bop-It requires children to carry out actions associated with musical noises and Simon Trickster requires children to replicate sequences of tones and lights.
A speech-language therapist certified by the American Speech-Language Hearing Association carried out all treatment sessions and administered the repeated-dependent measures at the end of the sessions. The clinician was instructed to interact normally with the participants. A complete lack of verbal interaction with participants would likely result in a very artificial atmosphere, potentially reducing participants’ faith in the legitimacy of the treatment. However, the clinician was also trained to avoid using traditional linguistic therapy techniques, such as recasts, corrections and expansions of child utterances. In addition, the clinician was a monolingual speaker of English. Therefore, no Spanish was spoken in any treatment session. Pre- and post-treatment testing in Spanish was conducted by two graduate students in speech-language pathology and one certified speech-language pathologist, all of whom were fluent in Spanish.
Measures
Two types of dependent variables were employed in this study: repeated measures and standardized pre/post-treatment assessments. The purpose of the repeated measures was to track change in targeted skills across the baseline and treatment phases. Five tasks were employed for this purpose: three in English, one in Spanish and one nonlinguistic cognitive processing task. The greater number of English versus Spanish tasks was due to the logistical impossibility of bringing in a Spanish-speaking task administrator on a daily basis. All repeated measures were administered to the participants three times per week throughout the study. A summary of the repeated measures appears in Table I.
Table I.
Repeated dependent measures tasks.
| Task name | Construct of interest | Domain | Dependent variable |
|---|---|---|---|
| Choice Visual Detection | Processing speed | Nonlinguistic cognitive | Mean RT in milliseconds |
| Rapid Automatic naming | Lexical processing efficiency | English | Total time in seconds |
| Sentence repetition | Access to lexical and morphosyntactic knowledge | English | Percentage of words repeated correctly |
| Nonword repetition | Phonological working memory | English | PPC |
| Nonword repetition | Phonological working memory | Spanish | PPC |
The first repeated measure was a choice visual detection task. The choice visual detection task is a measure of visual nonlinguistic cognitive processing speed, and is sensitive to PLI (Kohnert & Windsor, 2004). The task was implemented in E-Prime (Psychology Software Tools, Inc., 2000). To complete the task, each participant was seated in front of the computer with the index finger of his or her dominant hand resting equidistant between two buttons on a response box. The participant was instructed to respond as quickly as possible to the appearance of a colored circle on the computer screen. The participant was then trained to use one of the response buttons for a red circle and the other for a blue circle, with ensuing practice to ensure comprehension. The choice visual detection task contains 25 trials. The dependent variable of interest is mean reaction time (RT), calculated from correct responses only. In addition, any response time greater than 2000 ms, less than 50 ms or greater than 2 standard deviations from an individual child’s daily mean was trimmed from the mean RT calculation.
The second repeated measure was a sentence repetition task in English. To construct this task, sentence stimuli were extracted from the Recalling Sentences subtest of the Clinical Evaluation of Language Fundamentals – 4th Edition, English (CELF-4E). Sentence recall tasks appear closely linked to language learning abilities, an association that may be driven in part by the ability to access information in long-term memory stores (Alloway & Gathercole, 2005). Four sets of equivalent difficulty were created: each set included one sentence with 6 or 7 words, one sentence with 10 or 11 words and one sentence with 13 or 14 words. Sentences were always presented in increasing order of difficulty. The presentation rotated through the four sets to minimize practice effects. The dependent variable for the sentence repetition task was the percentage of words repeated correctly.
The third repeated measure was a rapid automatic naming task, conducted in English. This task was employed as a measure of lexical processing speed. The same task provided strong evidence of nonlinguistic cognitive processing treatment effects in monolingual children with PLI (Ebert & Kohnert, 2009). To complete the rapid automatic naming task, children were asked to name 32 color–shape combinations. The color–shape combinations were displayed in a four by eight array of images; each image was one of four shapes (star, circle, square or triangle) filled with one of four colors (red, yellow, green or blue). Four different versions of the array were created to prevent practice effects. Because task accuracy was consistently high (with the mean number of errors per administration below 0.5 for all participants), the total time to name all shapes was the dependent variable of interest.
The final two repeated measures were nonword repetition tasks in English and in Spanish. Nonword repetition is often considered a measure of phonological working memory and is well established as an area of deficit in PLI. English nonword stimuli were drawn from Dollaghan and Campbell (1998) and Spanish nonword stimuli were drawn from Ebert, Kalanek, Cordero, and Kohnert (2008). Four sets of equivalent difficulty were recorded in each language. In English, a set consisted of one word at each of three different syllable lengths (two, three and four syllables); in Spanish, a set consisted of one word at each of four syllable lengths (two, three, four and five syllables). The words were administered over headphones to the participant. The participant was asked to repeat each word and responses were recorded for later transcription and scoring. Scoring was conducted according to Dollaghan and Campbell (1998), resulting in a percent phonemes correct (PPC) score for each language. A second coder rescored 20% of nonword repetition samples. Phoneme-by-phoneme interrater reliability was 80% for English nonwords and 87% for Spanish nonwords.
In addition to the repeated measures, standardized language assessments were administered immediately prior to and following treatment to gauge progress in English and Spanish using conventional language tests. Measures included an assessment of global language in English (Clinical Evaluation of Language Fundamentals – 4, CELF-4E; Semel, Wiig, & Secord, 2003) and in Spanish (Clinical Evaluation of Language Fundamentals – 4, CELF-4S; Wiig, Secord, & Semel, 2006); an assessment of expressive vocabulary in English (Expressive One-Word Vocabulary Test, EOWPVT-E; Brownell, 2000a) and in Spanish (Expressive One-Word Picture Vocabulary Test – Spanish-Bilingual Edition, EOWPVT-S; Brownell, 2001a); and an assessment of receptive vocabulary in English (Receptive One-Word Vocabulary Test, ROWPVT-E; Brownell, 2000b) and in Spanish (Expressive One-Word Picture Vocabulary Test – Spanish-Bilingual Edition, EOWPVT-S; Brownell, 2001b). Because the stimuli from the Recalling Sentences subtest on the CELF-4E were used for the repeated measures task, this subtest was not administered in English. The omission resulted in the inability to calculate the Core Language score on the CELF-4E; instead each subtest was scored according to published procedures.
Analyses
Separate data analysis procedures were conducted for each of the two types of outcome measures. For the repeated measures data, visual analysis and effect sizes were combined to make judgments about treatment effectiveness. Appropriate effect sizes in SSED are the source of substantial discussion (e.g. Busk & Serlin, 1992; Olive & Smith, 2005). In order to present a complete picture of the repeated measures data in this study, we calculated three types of effect sizes. The first one, d, has been used in past SSEDs on treatment of PLI (Ebert & Kohnert, 2009; Gillam et al., 2001). It is calculated by subtracting the mean of the first three data points, representing baseline performance, from the mean of the last three data points, representing performance at the end of intervention. The result is then divided by the pooled standard deviation for all data points. This procedure acknowledges the potential for gradual change throughout an intervention, but may over-represent change if performance improves substantially at the end of intervention.
The second effect size, SMDbaseline, is calculated by subtracting the mean of the baseline data points from the mean of all data points following the introduction of treatment, and dividing by the standard deviation of the baseline data points (Busk & Serlin, 1992). Thus, SMDbaseline differs from d in two ways: treatment is represented using all data points instead of the final three and variance is represented using only the baseline data points rather than all data points. According to Busk and Serlin (1992), this measure has the advantage of imposing no statistical assumptions on the data.
The third effect size, SMDpooled, is the same as SMDbaseline except that (like d) it uses the pooled standard deviation across all data points instead of from the baseline only. It assumes equal variances across both baseline and treatment phases (Busk & Serlin, 1992); given the relatively small number of baseline data points in this study, it may provide a more accurate measure of variance.
For all three effect sizes, a criterion for “clinically significant change” was adopted in order to provide a context for interpreting SSED effect sizes. Following Gillam et al. (2001), we considered effect sizes of 0.8 or larger to indicate clinically significant change.
Standardized test scores were analyzed by constructing a 90% confidence interval around the pre-treatment test score. Post-treatment test scores that exceeded the 90% confidence interval were considered significantly different from the pre-test score.
Results
Using the three types of effect sizes described above resulted in the calculation of 30 effect sizes. These effect sizes are displayed in Table II. All effect sizes represented positive change over time. However, two effect sizes for P1’s Choice Visual Detection were nearly zero. Excluding these two effect sizes, all remaining calculations resulted in effect sizes of 0.88 or larger. Thus, evidence of clinically significant change can be seen on all five repeated measures tasks for P2 and on four of five repeated measures tasks for P1.
Table II.
Repeated measures effect sizes.
| P1
|
P2
|
|||
|---|---|---|---|---|
| Task | Type | Effect size | Type | Effect size |
| Choice Visual Detection | d | 1.67 | d | 1.81 |
| SMDbaseline | 0.01 | SMDbaseline | 3.46 | |
| SMDpooled | 0.01 | SMDpooled | 1.08 | |
| Sentence repetition | d | 2.03 | d | 1.8 |
| SMDbaseline | 1.8 | SMDbaseline | 1.2 | |
| SMDpooled | 1.6 | SMDpooled | 1.39 | |
| Rapid Automatic Naming | d | 2.3 | d | 0.88 |
| SMDbaseline | 3.4 | SMDbaseline | 0.9 | |
| SMDpooled | 3.8 | SMDpooled | 0.99 | |
| Nonword repetition, English | d | 2.06 | d | 1.27 |
| SMDbaseline | 1.69 | SMDbaseline | 5.5 | |
| SMDpooled | 1.76 | SMDpooled | 0.98 | |
| Nonword repetition, Spanish | d | 2.01 | d | 1.12 |
| SMDbaseline | 2.3 | SMDbaseline | 3.18 | |
| SMDpooled | 1.79 | SMDpooled | 0.98 | |
Notes: Three effect sizes for each measure and each participant are presented. All effect sizes provide an estimate of change from baseline to treatment, in standard deviation units. The signs on the Choice Visual Detection and Rapid Automatic Naming effect sizes were inverted so that a positive sign uniformly indicates positive change across time. The first effect size, d, was calculated by subtracting the mean of the three baseline data points from the mean of the last three data points and dividing by the pooled standard deviation across all data points for an individual (Gillam et al., 2001). The second effect size, SMDbaseline, was calculated by subtracting the mean of the three baseline data points from the mean of all treatment data points and dividing by the standard deviation of the baseline data points (Busk & Serlin, 1992). The third effect size, SMDpooled, was calculated by subtracting the mean of the three baseline data points from the mean of all treatment data points and dividing by the pooled standard deviation across all data points for an individual (Busk & Serlin, 1992).
The effect sizes should be interpreted in conjunction with visual analysis of the patterns in the repeated measures data. Figure 1 displays the data for the two timed repeated measures, Choice Visual Detection and Rapid Automatic Naming. For both participants, the Rapid Automatic Naming graph shows improvement during the baseline period. This pattern is suggestive of practice effects rather than intervention effects. In contrast, the baselines displayed on the Choice Visual Detection graphs show no overall trend toward improvement (or deterioration) during the baseline period.
Figure 1.
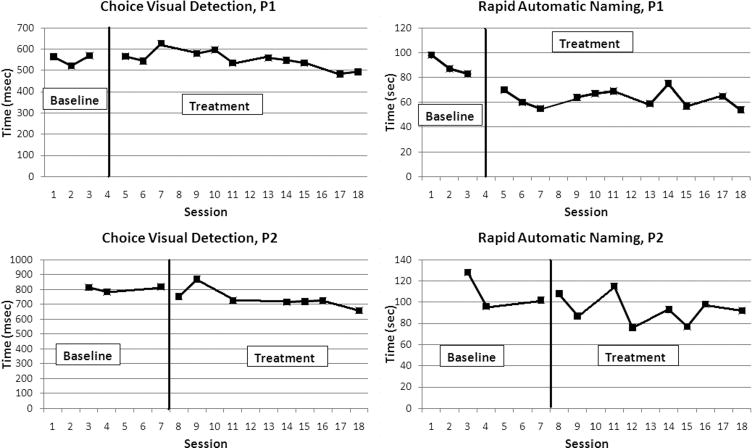
Results of timed repeated measures tasks. Upper graphs show performance across time for the first participant (P1) and lower graphs show performance for second participant (P2). The vertical black line on each graph indicates the start of the intervention phase. Improvement on the timed tasks is indicated by lower scores or lines with negative slope.
The repeated measures data for the three accuracy tasks (Sentence Repetition, English and Spanish Nonword Repetition) are displayed in Figure 2. All six graphs show stable or declining baselines, with improvement during the treatment period. The figure also reveals potential ceiling effects for P1 on Spanish Nonword Repetition.
Figure 2.
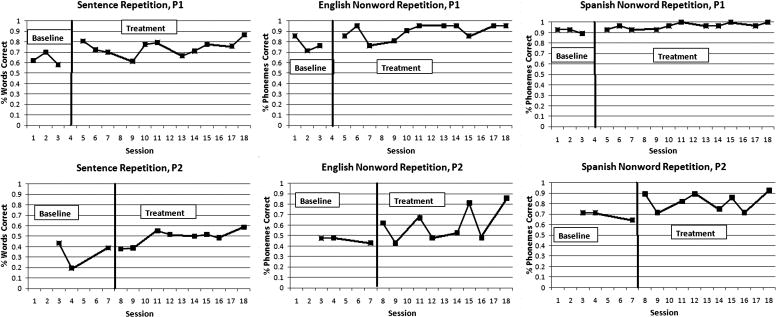
Results of accuracy repeated measures tasks. Upper graphs show performance across time for the first participant (P1) and lower graphs show performance for second participant (P2). The vertical black line on each graph indicates the start of the intervention phase. Improvement on the accuracy tasks is indicated by higher scores or lines with positive slope.
All standardized language test scores from pre- and post-treatment testing are displayed in Table III. P1 made significant gains on two subtests from the CELF-4E: Concepts and Following Directions and Word Structure. This participant also demonstrated a post-treatment test score below the 90% confidence interval for the pre-treatment test score on one test, the ROWPVT-S. P2 made significant gains on both Spanish vocabulary tests (the ROWPVT-S and EOWPVT-S). All other post-treatment test scores fell within the 90% confidence interval for the pre-treatment test score, indicating that the post-treatment test score did not differ significantly from the pre-treatment test score.
Discussion
The results of the repeated measures tasks suggest that the treatment program led to changes in the nonlinguistic processing speed of participants, as measured by the Choice Visual Detection task, as well as in their sentence and nonword repetition skills. The apparent practice effects reflected by the improvement during the baseline period for Rapid Automatic Naming preclude an interpretation of treatment effects on that measure. However, the repeated measures graphs and effect sizes overall present some evidence of nonlinguistic and linguistic change during the treatment period.
An examination of the effect sizes and the repeated measures graphs illustrates some of the considerations in calculating SSED effect sizes for language treatment studies. For example, the three effect sizes for Choice Visual Detection for P1 are quite different from each other. This results from including all treatment data points in the calculation of SMDbaseline and SMDpooled, and only the final three data points in the calculation of d. Figure 1 shows that P1’s performance on Choice Visual Detection improved dramatically at the final two treatment sessions. Including all treatment data points in the effect size prevents overemphasis on these final sessions (Olive & Smith, 2005). In language treatment, however, gradual growth throughout treatment may be more likely than instantaneous change at the introduction of treatment; in this scenario, including all treatment data points may mask growth.
Other differences between effect size measures are illustrated by P2’s results for Choice Visual Detection, English Nonword Repetition and Spanish Nonword Repetition. For each of these tasks, the SMDbaseline calculation results in substantially larger values than the other two effect size variants. Inspection of the visual data indicates that P2 had little variance during the baseline period for these tasks. Although SMDbaseline is typically considered advantageous (Busk & Serlin, 1992; Olive & Smith, 2005), it can result in extraordinarily large effect sizes when baseline variance is minimal, which is indeed the ideal in SSED.
Outside of these differences, the three effect sizes for each measure are generally complementary, and clearly show that treatment produced some change in the indexed skills (with the possible exception of Choice Visual Detection for P1). The differences between effect sizes highlighted here illustrate the need for interpreting SSED effect sizes with caution, and in conjunction with complete visual data (Olive & Smith, 2005).
As expected, there were fewer significant changes evident in standardized test scores as compared to the more sensitive repeated measures. The treatment period in this study was likely too brief to produce unequivocal changes on standardized test scores; even so both participants demonstrated significant gains on two of the standardized measures. There was one instance of significant loss in the standardized language test scores (for P1 on the ROWPVT-S). This result may be partially attributed to P1’s age gain between pre-treatment and post-treatment testing, which resulted in a new set of comparison norms, and partially attributed to the exceptionally high pre-treatment test score for this child. However, it is clear that, unlike P2, P1 did not derive significant benefit from the treatment in the area of Spanish vocabulary.
Overall, the standardized test scores and the repeated measures complement each other. The repeated measures provide a fine-grained view of subtle changes in cognitive-linguistic skills over the treatment period, whereas the standardized tests provide an indication that some of these changes were large enough to result in immediate changes in standardized scores.
The evidence of Spanish language gains is particularly important to the hypothesis of interest here. Both participants achieved effect sizes on the Spanish nonword repetition task that were well above the threshold of clinical significance, 0.8 standard deviations (Gillam et al., 2001). P2 also made gains in both receptive and expressive Spanish vocabulary. These L2 gains are consistent with the possibility that changes in underlying information processing skills, combined with opportunities to use Spanish in the home, improved Spanish language skills.
Replicating Treatment Effects for Nonlinguistic Cognitive Processing Treatment
In past work with nonlinguistic cognitive processing treatment (Ebert & Kohnert, 2009), we hypothesized that the treatment facilitated language performance via improved access to stored information, at least in the short time period of the study. The largest changes in the previous study were seen on expressive vocabulary testing, Rapid Automatic Naming and formulated sentences. The same explanation could account for some of the results seen here, although the pattern is not identical. Only one participant improved expressive vocabulary scores, in only one language, and the practice effects seen in the Rapid Automatic Naming data limit any interpretation of treatment effects on this task. However, the large improvement for P1 in performance on the Word Structure subtest of the CELF-4E is in fact consistent with facilitated access to stored information. In addition, the sentence repetition measure included in this study has been hypothesized to index access to stored linguistic knowledge (Alloway & Gathercole, 2005). Both participants made substantial gains on the sentence repetition measure, again supporting a link between the treatment and information access.
Key differences between the two studies may play a role in the outcomes. First, the treatment period was slightly shorter in the present study than in the previous study; for P2, who had poor attendance, the amount of treatment delivered was substantially less. This is likely to result in smaller gains on standardized tests than were seen in Ebert and Kohnert (2009). However, the repeated measures tasks were also adjusted from past work; we decreased the difficulty of nonword repetition task, eliminated a short-term auditory memory task, and added the sentence repetition task. These adjustments resulted in more robust evidence of change on repeated measures than were seen in the previous study.
Secondly, there was an intentional difference in the type of participants in the present study: all four participants across the two studies shared a diagnosis of PLI, but the two participants included in this study were bilingual. The cognitive-linguistic system of bilingual children is by definition distinct from that of monolingual children, and it is not surprising that cognitive processing treatment effects would manifest themselves slightly differently between the two populations. There is also some expected variation in individual children’s responses to the same treatment. Given the notable heterogeneity of the population of bilingual children with PLI (Kohnert, 2010), additional individual variation in treatment response seems likely. This prediction is consistent with actual results; the two participants in Ebert and Kohnert (2009) had quite similar outcomes to each other, whereas substantial between-participant differences were seen here.
Limitations and Future Directions
The primary limitation of this study, like most SSEDs, is its generalizability across the larger population of children with PLI. The data presented here provide evidence of change due to treatment in two individuals, but the design is not intended to provide inferences about the treatment’s effects across a population. Replication is essential for establishing the external validity of SSEDs (McReynolds & Thompson, 1986). Here we have provided a replication and extension of past work on this type of treatment (Ebert & Kohnert, 2009). Further investigation is needed to determine if a broader range of children with PLI could benefit from treatment focused on basic cognitive processing mechanisms. In addition, the breadth of evidence for change in L1 (Spanish) is limited here. A full battery of Spanish testing was conducted at pre- and post-treatment testing, but the Spanish repeated measures were limited to nonword repetition. Performance on this measure does provide clear evidence of some changes in L1, which is essential to the primary purpose of the study. However, a broader array of repeated measures tasks in Spanish would enhance our ability to compare and contrast treatment effects in L1 and L2.
Finally, the relatively poor attendance of P2 presents a challenge for interpreting the results of this study. That is, despite receiving approximately 50% of the treatment dosage that P1 received, P2 was able to make comparable or sometimes larger gains. One possible explanation for this result is that P2, with a more severe impairment, had more room for growth in all areas and was thus more responsive to treatment. Another possibility is that, while some treatment of nonlinguistic cognitive processing skills is helpful, more is not necessarily better. In other words, P1 might have also demonstrated gains in just seven treatment sessions. In order to refine the nonlinguistic cognitive processing treatment program presented here, future studies should investigate the effects of treatment dosage more systematically.
The long-term goal of this line of work is to determine whether nonlinguistic cognitive processing activities would be useful as part of a language-based treatment program for children with PLI (e.g. Leonard et al., 2007). This study contributes to the first step of that process: establishing the treatment’s effects in isolation. To complete this first step, studies that examine the effects of nonlinguistic cognitive processing treatment in larger groups of children with PLI will be essential. The effects of integrating this type of nonlinguistic cognitive processing work into more traditional language interventions can then be investigated.
It will also be important to compare the effects of nonlinguistic cognitive processing treatment to outcomes following more conventional language treatments, documenting performance on both language and cognitive processing measures. In addition to advancing pedagogy, this type of study would allow us to investigate the directionality of cross-domain transfer to provide additional theoretical insight. That is, the current study investigates the possibility of transfer from cognition to language. It will also be important to determine if language treatment results in improved cognitive processing. We are currently investigating the absolute and relative efficacy of non-linguistic cognitive processing treatment as compared to English-only and bilingual treatments using a larger randomized group design with Spanish–English school–age children with PLI.
Acknowledgments
Funding for this project was provided by NIH NIDCD 1R21DC010868, awarded to Kathryn Kohnert, and by a Doctoral Dissertation Fellowship from the University of Minnesota Graduate School, awarded to Kerry Danahy Ebert. We thank Maura Arnoldy, Mary DesChamps and Amelia Medina for their assistance with Spanish language testing. We are also grateful to Dr Frank Cirrin and the faculty and staff of participating Minneapolis Public Schools.
Footnotes
Declaration of Interest: The authors report no conflicts of interest.
References
- Alloway TP, Gathercole SE. The role of sentence recall in reading and language skills of children with learning difficulties. Learning and Individual Differences. 2005;15:271–282. [Google Scholar]
- Baker E, McLeod S. Evidence-based practice for children with speech sound disorders: Part 1 narrative review. Language, Speech, and Hearing Services in Schools. 2011;42:102–139. doi: 10.1044/0161-1461(2010/09-0075). [DOI] [PubMed] [Google Scholar]
- Brown L, Sherbenou R, Johnsen S. Test of nonverbal intelligence. 3. Austin, TX: Pro-Ed; 1997. [Google Scholar]
- Brownell R. Expressive one-word picture vocabulary test. Novato, CA: Academic Therapy Publications; 2000a. [Google Scholar]
- Brownell R. Receptive one-word picture vocabulary test. Novato, CA: Academic Therapy Publications; 2000b. [Google Scholar]
- Brownell R. Expressive one-word picture vocabulary test – Spanish-bilingual edition. Novato, CA: Academic Therapy Publications; 2001a. [Google Scholar]
- Brownell R. Receptive one-word picture vocabulary test – Spanish-bilingual edition. Novato, CA: Academic Therapy Publications; 2001b. [Google Scholar]
- Busk PL, Serlin RC. Meta-analysis for single case research. In: Kratochwill TR, Levin JR, editors. Single-case research designs and analysis: New directions for psychology and education. Hillsdale, NJ: Lawrence Erlbaum; 1992. pp. 187–212. [Google Scholar]
- Caesar LG, Kohler PD. The state of school-based bilingual assessment: Actual practice versus recommended guidelines. Language, Speech, and Hearing Services in Schools. 2007;38:190–200. doi: 10.1044/0161-1461(2007/020). [DOI] [PubMed] [Google Scholar]
- Cirrin FM, Gillam RB. Language intervention practices for school-aged children with spoken language disorders: A systematic review. Language, Speech, and Hearing Services in Schools. 2008;39:S110–S137. doi: 10.1044/0161-1461(2008/012). [DOI] [PubMed] [Google Scholar]
- Dollaghan C, Campbell T. Nonword repetition and child language impairment. Journal of Speech, Language, and Hearing Research. 1998;41:1136–1146. doi: 10.1044/jslhr.4105.1136. [DOI] [PubMed] [Google Scholar]
- Ebert KD, Kalanek J, Cordero KN, Kohnert K. Spanish nonword repetition: Stimuli development and preliminary results. Communication Disorders Quarterly. 2008;29:67–74. doi: 10.1177/1525740108314861. [DOI] [Google Scholar]
- Ebert KD, Kohnert K. Efficacy of nonlinguistic cognitive intervention for school-aged children with language impairment. Clinical Linguistics and Phonetics. 2009;23:647–664. doi: 10.1080/02699200902998770. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ebert KD, Kohnert K. Sustained attention in children with primary language impairment: A meta-analysis. Journal of Speech, Language, and Hearing Research. 2011;54:1372–1384. doi: 10.1044/1092-4388(2011/10-0231). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ellis Weismer S, Evans J, Hesketh L. An examination of verbal working memory capacity in children with specific language impairment. Journal of Speech, Language, and Hearing Research. 1999;42:1249–1260. doi: 10.1044/jslhr.4205.1249. [DOI] [PubMed] [Google Scholar]
- Fazio B. Arithmetic calculation, short-term memory, and language performance in children with specific language impairment: A 5-year follow-up. Journal of Speech, Language, and Hearing Research. 1999;42:420–431. doi: 10.1044/jslhr.4202.420. [DOI] [PubMed] [Google Scholar]
- Finneran DA, Francis AL, Leonard LB. Sustained attention in children with specific language impairment (SLI) Journal of Speech, Language, and Hearing Research. 2009;52:915–929. doi: 10.1044/1092-4388(2009/07-0053). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gathercole SE. Nonword repetition and word learning: The nature of the relationship. Applied Psycholinguistics. 2006;27:513–543. doi: 10.1017.S0142716406060383. [Google Scholar]
- Gillam RB, Crofford JA, Gale MA, Hoffman LM. Language change following computer-assisted language instruction with Fast ForWord or Laureate Learning Systems software. American Journal of Speech-Language Pathology. 2001;10:231–247. doi: 10.1044/1058-0360(2001/021). [DOI] [Google Scholar]
- Gillam RB, Loeb DF, Hoffman LM, Bohman T, Champlin CA, Thibodeau L, Widen J, Brandel J, Friel-Patti S. The efficacy of Fast ForWord Language intervention in school-age children with language impairment: A randomized controlled trial. Journal of Speech, Language, and Hearing Research. 2008;51:97–119. doi: 10.1044/1092-4388(2008/007). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gillam SL, Gillam RB. Making evidence-based decisions about child language intervention in schools. Language, Speech, and Hearing Services in Schools. 2006;37:304–315. doi: 10.1044/0161-1461(2006/035). doi: 0161-1461/06/3704-0304. [DOI] [PubMed] [Google Scholar]
- Graf Estes K, Evans JL, Else-Quest NM. Differences in the nonword repetition performance of children with and without specific language impairment: A meta-analysis. Journal of Speech, Language, and Hearing Research. 2007;50:177–195. doi: 10.1044/1092-4388(2007/015). [DOI] [PubMed] [Google Scholar]
- Hammill DD, Larsen SC. The effectiveness of psycholinguistic training: A reaffirmation of position. Exceptional Children. 1978;44:402–414. doi: 10.1177/001440297804400602. [DOI] [PubMed] [Google Scholar]
- Hoffman LM, Gillam RB. Verbal and spatial information processing constraints in children with specific language impairment. Journal of Speech, Language, and Hearing Research. 2004;47:114–125. doi: 10.1044/1092-4388(2004/011). [DOI] [PubMed] [Google Scholar]
- Kazdin AE. Drawing valid inferences from case studies. Journal of Consulting and Clinical Psychology. 1981;49:183–192. doi: 10.1037/0022-006X.49.2.183. [DOI] [PubMed] [Google Scholar]
- Kelley A, Kohnert K. Is there a cognate advantage for Spanish-speaking ELLs? Language, Speech and Hearing Services in Schools. 2012 doi: 10.1044/0161-1461(2011/10-0022). [DOI] [PubMed] [Google Scholar]
- Kirk SA, McCarthy JJ, Kirk WD. Illinois test of psycholinguistic abilities. Urbana, IL: University of Illinois Press; 1968. (rev. ed.) [Google Scholar]
- Kohnert K. Language disorders in bilingual children and adults. San Diego, CA: Plural; 2007. [Google Scholar]
- Kohnert K. Bilingual children with primary language impairment: Issues, evidence and implications for clinical actions. Journal of Communication Disorders. 2010;43:456–473. doi: 10.1016/j.jcomdis.2010.02.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kohnert K, Ebert KD. Beyond morphosyntax in developing bilinguals and “specific” language impairment. Applied Psycholinguistics. 2010;31:303–310. [Google Scholar]
- Kohnert K, Medina A. Bilingual children and communication disorders: A 30-year research retrospective. Seminars in Speech and Language. 2009;30:219–233. doi: 10.1055/s-0029-1241721. [DOI] [PubMed] [Google Scholar]
- Kohnert K, Windsor J. The search for common ground part II: Nonlinguistic performance by linguistically diverse learners. Journal of Speech, Language, and Hearing Research. 2004;47:891–903. doi: 10.1044/1092-4388(2004/066). [DOI] [PubMed] [Google Scholar]
- Kohnert K, Windsor J, Ebert KD. Primary or “specific” language impairment and children learning a second language. Brain and Language. 2009;109:101–111. doi: 10.1016/j.bandl.2008.01.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kohnert K, Yim D, Nett K, Kan PF, Duran L. Intervention with linguistically diverse preschool children: A focus on developing home language(s) Language, Speech, and Hearing Services in Schools. 2005;36:251–263. doi: 10.1044/0161-1461(2005/025). [DOI] [PubMed] [Google Scholar]
- Leonard L, Ellis Weismer S, Miller CA, Francis DJ, Tomblin JB, Kail RV. Speed of processing, working memory, and language impairment in children. Journal of Speech, Language, and Hearing Research. 2007;50:408–428. doi: 10.1044/1092-4388(2007/029). [DOI] [PubMed] [Google Scholar]
- Marton K. Visuo-spatial processing and executive functions in children with specific language impairment. International Journal of Language and Communication Disorders. 2008;43:181–200. doi: 10.1080/16066350701340719. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McReynolds LV, Thompson CK. Flexibility of single-subject experimental designs. Part I: Review of the basics of single-subject designs. Journal of Speech and Hearing Disorders. 1986;51:194–203. doi: 10.1044/jshd.5103.194. [DOI] [PubMed] [Google Scholar]
- Miller C, Kail R, Leonard L, Tomblin B. Speed of processing in children with specific language impairment. Journal of Speech, Language, and Hearing Research. 2001;44:416–433. doi: 10.1044/1092-4388(2001/034). [DOI] [PubMed] [Google Scholar]
- Minnesota Office of the Revisor of Statutes. Speech or language impairments. 2008 (Rule 3525.1343). Retrieved May 15, 2011, from https://www.revisor.mn.gov/rules/?id=3525.1343.
- Montgomery JW, Evans JL, Gillam RB. Relation of auditory attention and complex sentence comprehension in children with specific language impairment: A preliminary study. Applied Psycholinguistics. 2009;30:123–151. doi: 10.1017/S0142716408090061. [DOI] [Google Scholar]
- Montgomery JW, Magimairaj BM, Finney MC. Working memory and specific language impairment: An update on the relation and perspectives on assessment and treatment. American Journal of Speech-Language Pathology. 2010;19:78–94. doi: 10.1044/1058-0360(2009/09-0028). [DOI] [PubMed] [Google Scholar]
- Olive ML, Smith BW. Effect size calculations and single subject designs. Educational Psychology. 2005;25:313–324. doi: 10.1080/0144341042000301238. [DOI] [Google Scholar]
- Pham G, Kohnert K, Mann D. Addressing clinician-client mismatch: A preliminary intervention study with a bilingual Vietnamese-English preschooler. Language, Speech, and Hearing Services in Schools. 2011;42:408–422. doi: 10.1044/0161-1461(2011/10-0073). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Psychology Software Tools, Inc. E-Prime, Computer software. Pittsburgh, PA: Author; 2000. [Google Scholar]
- Restrepo MA. Identifiers of predominantly Spanish-speaking children with language impairment. Journal of Speech, Language, and Hearing Research. 1998;41:1398–1411. doi: 10.1044/jslhr.4106.1398. [DOI] [PubMed] [Google Scholar]
- Royal College of Speech and Language Therapists Special Interest Group in Bilingualism. Good practice for speech and language therapists working with clients from linguistic minority communities. 2007 Retrieved August 3, 2011, from http://www.rcslt.org/members/publications/linguistic_minorities.
- Scarry-Larkin M, Price E. LocuTour Multimedia Attention and Memory: Volume II, Computer software. San Luis Obispo, CA: Learning Fundamentals; 2007. [Google Scholar]
- Semel E, Wiig EH, Secord WA. Clinical evaluation of language fundamentals. 4. San Antonio, TX: The Psychological Corporation; 2003. [Google Scholar]
- Spaulding TJ, Plante E, Vance R. Sustained selective attention skills of preschool children with specific language impairment: Evidence for separate attentional capacities. Journal of Speech, Language, and Hearing Research. 2008;51:16–34. doi: 10.1044/1092-4388(2008/002). [DOI] [PubMed] [Google Scholar]
- Staupe R. Blink. Madison, WI: Out of the Box Publishing; 2001. [Google Scholar]
- Stevens C, Fanning J, Coch D, Sanders L, Neville H. Neural mechanisms of selective auditory attention are enhanced by computerized training: Electrophysiological evidence from language-impaired and typically developing children. Brain Research. 2008;1205:55–69. doi: 10.1016/j.brainres.2007.10.108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tallal P, Miller SL, Bedi G, Byma G, Wang XQ, Nagarajan SS, Schreiner C, Jenkins WM, Merzenich MM. Language comprehension in language-learning impaired children improved with acoustically modified speech. Science. 1996;271:81–84. doi: 10.1126/science.271.5245.81. [DOI] [PubMed] [Google Scholar]
- Ullman MT, Pierpont EI. Specific language impairment is not specific to language: The procedural deficit hypothesis. Cortex. 2005;41:399–433. doi: 10.1016/S0010-9452(08)70276-4. [DOI] [PubMed] [Google Scholar]
- van Weerdenburg M, Verhoeven L, van Balkom H. Towards a typology of specific language impairment. Journal of Child Psychology and Psychiatry. 2006;47:176–189. doi: 10.1111/j.1469-7610.2005.01454.x. [DOI] [PubMed] [Google Scholar]
- Wiig EH, Secord WA, Semel E. Clinical evaluation of language fundamentals. 4. San Antonio, TX: The Psychological Corporation; 2006. Spanish. [Google Scholar]
- Windsor J, Kohnert K. The search for common ground: Part I. Lexical performance by linguistically diverse learners. Journal of Speech, Language, and Hearing Research. 2004;47:877–890. doi: 10.1044/1092-4388(2004/065). [DOI] [PubMed] [Google Scholar]
- Windsor J, Kohnert K, Loxtercamp AL, Kan PF. Performance on nonlinguistic visual tasks by children with language impairment. Applied Psycholinguistics. 2008;29:237–268. doi: 10.1017/S0142716407080113. [DOI] [Google Scholar]
- Yim D, Kohnert K, Windsor J. Sensitivity and specificity to LI for a non-linguistic processing task. Paper presented at the American Speech-Language-Hearing Association Annual Convention; San Diego, CA. 2005. [Google Scholar]