

Abstract
Purpose:
We assessed the prevalence of the clinically important posterior fossa emissary veins detected on computed tomography (CT) angiography.
Materials and Methods:
A total of 182 consecutive patients who underwent 64-slice CT angiography were retrospectively reviewed to determine the clinically important posterior fossa emissary veins.
Results:
Of 166 patients, the mastoid emissary vein (MEV) was not identified in 37 (22.3%) patients. It was found bilaterally in 82 (49.4%) and unilaterally in 47 (28.3%) patients. Only six patients had more than one MEV that were very small (<2 mm), and only five patients had very large (>5 mm) veins. The posterior condylar vein (PCV) was not identified in 39 (23.5%) patients. It was found bilaterally in 97 (58.4%) and unilaterally in 30 (18.1%) patients. Only 15 patients had a very large (>5 mm) PCV. The petrosquamosal sinus (PSS) was identified only in one patient (0.6%) on the left side. The occipital sinus was found in two patients (1.2%).
Conclusions:
The presence of the clinically important posterior fossa emissary veins is not rare. Posterior fossa emissary veins should be identified and systematically reported, especially prior to surgeries involving the posterior fossa and mastoid region.
Keywords: Anatomy, angiography, blood vessels, computed tomography, emissary vein, posterior fossa
Introduction
Emissary veins are valveless veins that pass through cranial apertures. Along with the internal jugular vein, they participate in the extracranial venous drainage of the dural sinuses of the posterior fossa or play roles in jugular vein aplasia and thrombosis.[1]
The mastoid emissary vein (MEV), posterior condylar vein (PCV), petrosquamosal sinus (PSS), and occipital emissary vein (OEV) are the major posterior fossa emissary veins. It is important to recognize and describe these veins to prevent complications during surgeries.[2,3]
Few case series have investigated emissary veins in patients with inner ear malformations and craniofacial syndromes.[4,5] The prevalence of the posterior fossa emissary veins on computed tomography (CT) angiography in the general population has not been reported. We investigated the prevalence of the major posterior fossa emissary veins on CT angiography.
Materials and Methods
This retrospective study had institutional review board approval, with a waiver of the informed consent requirement. The CT data of 182 patients who underwent 64-slice CT angiography from September 2011 to August 2012 were retrospectively reviewed to identify the major posterior fossa emissary veins. Patients were referred for CT angiography because of various vascular pathologies.
All CT angiography examinations were performed using a 64-slice CT scanner (Aquilion 64; Toshiba Medical Systems, Tochigi, Japan) from the aortic arc through the cerebral vertex. All images were obtained with previously reported dose-reduction techniques.[6] In preparation for the study readings, all multidetector CT angiography data were transferred from the archive to a workstation (Aquarius Workstation; TeraRecon, San Mateo, CA) via internal network connections, providing 3D postprocessing options, multiplanar image reformatting (MPR), and maximum intensity projections. Images were separately reviewed by two radiologists. The images were reassessed to reach a consensus on all findings.
All the veins and canal were also evaluated by obtaining thin MPR images (1 mm collimation, bone window, sharpest filter). These setting allowed good delineation of the emissary veins and venous canals.
The bilateral posterior fossa emissary vein canals and veins (MEV, PCV, PSS, and OEV) and venous canal anomalies were evaluated as follows.
The MEV originates from the sigmoid sinus, crosses the mastoid foramen, and drains into the posterior auricular or occipital vein [Figure 1]. The MEV was classified according to its size and was considered to be small when it was <2 mm, medium when it was between 2 and 5 mm, and large when it was >5 mm.
Figure 1.
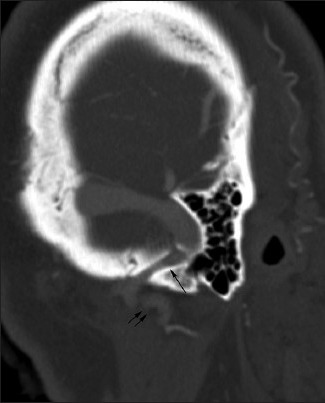
The mastoid emissary vein crosses the mastoid canal (arrow) and runs between the sigmoid sinus and the posterior auricular vein (double arrows)
The PCV usually originates from the superior bulb of the internal jugular vein, courses along the PCV canal, and drains into the deep cervical vein. It also connects with the horizontal portion of the vertebral artery venous plexus [Figure 2]. The PCV was classified according to its size and was considered to be small when it was <2 mm, medium when it was between 2 and 5 mm, and large when it was >5 mm.
Figure 2.
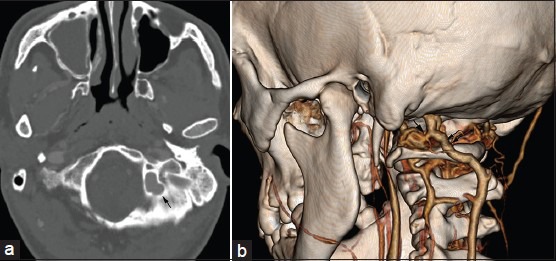
Multiplanar image reformatting (a) and 3D volume rendered (b) Images of the same patient show that the left large posterior condylar vein courses along the posterior condylar vein canal (arrow in a), originates from the superior bulb of the internal jugular vein, and drains into the deep cervical vein (double arrows in b). It connects with the horizontal portion of the vertebral artery venous plexus (arrow in b)
The OEV is located at the midline and connects the transverse sinuses near the confluens sinuum region to the suboccipital plexus [Figure 3].
Figure 3.
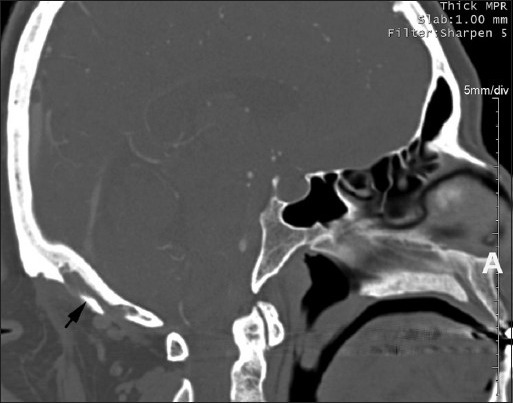
The occipital emissary vein canal (arrow) connects the transverse sinuses near the confluens sinuum region to the suboccipital plexus
The PSS arises from the transverse sinus or upper part of the sigmoid sinus, courses along the petrosquamosal fissure, and drains either into the retromandibular vein through the postglenoid foramen or into the pterygoid venous plexus through the foramen ovale [Figure 4].
Figure 4.
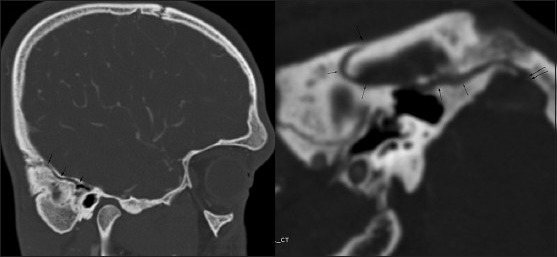
Curved planar reformation shows the petrosquamosal sinus that course along the petrosquamosal fissure (arrows) at the lateral part of the superior surface of the petrous bone
Results
Of the 182 patients evaluated, 16 were subsequently excluded (13 had inadequate image quality mainly due to patient movement and technical problems, and 3 underwent mastoid region and/or posterior fossa surgery prior to the CT angiography). The mean age of the remaining 166 patients (76 females, 90 males) was 52.7 years.
Table 1 outlines the prevalence of the MEV and the PCV on CT angiography. Table 2 shows the distribution of the detected MEV/canal and PCV/canal according to their diameters.
Table 1.
Prevalance of the MEV and PCV on CT angiography
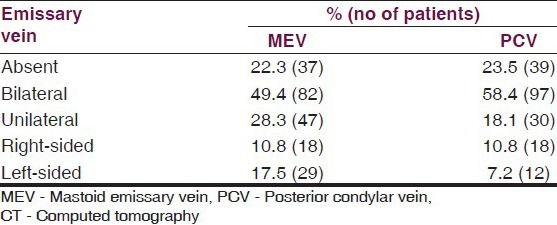
Table 2.
The distribution of the detected mastoid emissary vein/canal and posterior condylar vein/canal according to their diameters
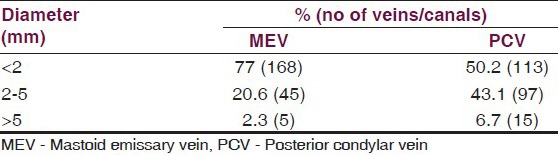
The MEVs were not identified in 37 (22.3%) patients. It was found bilaterally in 82 (49.4%) and unilaterally in 47 (28.3%) patients. Unilateral left-sided MEVs were more common (n = 29) than unilateral right-sided MEVs (n = 18). Only six patients had more than one MEV that were very small (<2 mm). Of all MEVs, only five were very large (>5 mm) (two on the right side and three on the left side).
The PCV were not identified in 39 (23.5%) patients. It was found bilaterally in 97 (58.4%) and unilaterally in 30 (18.1%) patients. The number of unilateral right-sided PCVs was slightly higher (n = 18) than unilateral left-sided ones (n = 12). Of all PCVs, only 15 were very large (>5 mm) (5 on the right side and 10 on the left side).
The PSS was identified in only one patient (0.6%) on the left side. The occipital sinus was found in only two patients (1.2%).
Discussion
Unrecognized major posterior fossa emissary veins can cause surgical complications such as bleeding, air embolism, retrograde spread of infection or tumors, and fatal increases in intracranial pressure.[2,3,4] Systematic evaluation of these veins prior to mastoid region and/or posterior fossa surgeries is clinically important. These veins are reportedly frequent in patients with inner ear malformations and craniofacial syndromes, but their prevalence in the general population has not been reported. We identified the prevalence of the major posterior fossa emissary veins on CT angiography.
CT angiography is a valuable tool for assessing the emissary veins and venous vascular canals. It is superior to MR venography in depicting venous structures with slower flow and smaller diameters.[7] It also has the advantage of imaging the bony canal.
The MEV was found bilaterally in 82 (49.4%) and unilaterally in 47 (28.3%) patients in our study. A previous study identified the MEV in 82% of patients on temporal CT.[8] However, their results concerned the incidence of the bony canal, not the emissary veins, and they did not classify these veins according to their diameter.
Persistent PSS was found in 1% of patients on routine temporal CT examinations, as noted by Koesling et al.,[8] and in up to 23% of corrosion casts, as noted by San Millán Ruiz et al.[9] In contrast to anatomical studies, radiological identification of posterior fossa emissary veins is quite uncommon.[10,11] They are usually observed in patients with inner ear malformations or craniofacial syndromes.[12,13] In the present study, which included only patients without these anomalies, only one patient (0.6%) had a unilateral left-sided PSS.
The frequency of PCV and OEV has not yet been published. The PCV and MEV were the most common emissary veins observed in our study. We classified the MEV and PCV according to their diameter. The diameter of the emissary vein should be determined because it may help plan the surgical approach.[14] The diameter of the MEV may be important because this vein is a potential target for cannulation during endovascular procedures involving the transverse or sigmoid sinus.[15] In addition, a large MEV and PCV may be associated with pulsatile tinnitus.[16,17]
Describing the posterior fossa emissary veins before surgery is very important because they are potential sources of intense bleeding and air embolism formation during surgical procedures. They can be the source of thrombosis in the sigmoid sinus after middle ear surgery or may cause retrograde, thrombophlebitic extension from an infected mastoid cavity.[10,18] Furthermore, emissary veins may represent the main outflow pathway in some cases, and particular care should be taken during surgical procedures in these patients. Sacrificing this outflow pathway could lead to catastrophic venous ischemic and hemorrhagic consequences.
The present study has some limitations. First, it was performed retrospectively. Second, it was conducted on the basis of image interpretations performed by means of consensus opinion. Third, because our study was based on the analysis of radiologic images, depiction of very small emissary veins could have been missed and was beyond the capability of the CT examinations. Finally, we only evaluated the major posterior fossa emissary veins that can be evaluated on CT angiography and have clinical importance. However, these veins are not limited to the MEV, PCV, PSS, and OEV.
In conclusion, the prevalence of the major posterior fossa emissary veins is not low in the general population, and CT angiography is the best method with which to display both an emissary vein and its canal. These veins should be identified and systematically reported, especially prior to surgeries that are related to the posterior fossa and mastoid region.
Footnotes
Source of Support: Nil.
Conflict of Interest: None.
References
- 1.San Millán Ruíz D, Gailloud P, Rüfenacht DA, Delavelle J, Henry F, Fasel JH. The craniocervical venous system in relation to cerebral venous drainage. AJNR Am J Neuroradiol. 2002;23:1500–8. [PMC free article] [PubMed] [Google Scholar]
- 2.Jeevan DS, Anlsow P, Jayamohan J. Abnormal venous drainage in syndromic craniosynostosis and the role of CT venography. Childs Nerv Syst. 2008;24:1413–20. doi: 10.1007/s00381-008-0667-8. [DOI] [PubMed] [Google Scholar]
- 3.Hadeishi H, Yasui N, Suzuki A. Mastoid canal and migrated bone wax in the sigmoid sinus: Technical report. Neurosurgery. 1995;36:1220–24. doi: 10.1227/00006123-199506000-00028. [DOI] [PubMed] [Google Scholar]
- 4.Anderson PJ, Harkness WJ, Taylor W, Jones BM, Hayward RD. Anomalous venous drainage in a case of non-syndromic craniosynostosis. Childs Nerv Syst. 1997;13:97–100. doi: 10.1007/s003810050052. [DOI] [PubMed] [Google Scholar]
- 5.Sandberg DI, Navarro R, Blanch J, Ragheb J. Anomalous venous drainage preventing safe posterior fossa decompression in patients with chiari malformation type I and multisutural craniosynostosis. Report of two cases and review of the literature. J Neurosurg. 2007;106(Suppl 6):490–4. doi: 10.3171/ped.2007.106.6.490. [DOI] [PubMed] [Google Scholar]
- 6.Thomas M, Barker N. Dose-optimised 3D CT evaluation. Toshiba Vis J. 2008;12:54–61. [Google Scholar]
- 7.Hoffmann O, Klingebiel R, Braun JS, Katchanov J, Valdueza JM. Diagnostic pitfall: Atypical cerebral venous drainage via the vertebral venous system. AJNR Am J Neuroradiol. 2002;23:408–11. [PMC free article] [PubMed] [Google Scholar]
- 8.Koesling S, Kunkel P, Schul T. Vascular anomalies, sutures and small canals of the temporal bone on axial CT. Eur J Radiol. 2005;54:335–43. doi: 10.1016/j.ejrad.2004.09.003. [DOI] [PubMed] [Google Scholar]
- 9.San Millán Ruíz D, Gailloud P, Yilmaz H, Perren F, Rathgeb JP, Rüfenacht DA, et al. The petrosquamosal sinus in humans. J Anat. 2006;209:711–20. doi: 10.1111/j.1469-7580.2006.00652.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Marsot-Dupuch K, Gayet-Delacroix M, Elmaleh-Bergès M, Bonneville F, Lasjaunias P. The petrosquamosal sinus: CT and MR findings of a rare emissary vein. AJNR Am J Neuroradiol. 2001;22:1186–93. [PMC free article] [PubMed] [Google Scholar]
- 11.Chauhan NS, Sharma YP, Bhagra T, Sud B. Persistence of multiple emissary veins of posterior fossa with unusual origin of left petrosquamosal sinus from mastoid emissary. Surg Radiol Anat. 2011;33:827–31. doi: 10.1007/s00276-011-0822-x. [DOI] [PubMed] [Google Scholar]
- 12.Giesemann AM, Goetz GF, Neuburger J, Lenarz T, Lanfermann H. Persistent petrosquamosal sinus: High incidence in cases of complete aplasia of the semicircular canals. Radiology. 2011;259:825–33. doi: 10.1148/radiol.11101466. [DOI] [PubMed] [Google Scholar]
- 13.Morimoto AK, Wiggins RH, 3rd, Hudgins PA, Hedlund GL, Hamilton B, Mukherji SK, et al. Absent semicircular canals in CHARGE syndrome: Radiologic spectrum of findings. AJNR Am J Neuroradiol. 2006;27:1663–71. [PMC free article] [PubMed] [Google Scholar]
- 14.Reis CV, Deshmukh V, Zabramski JM, Crusius M, Desmukh P, Spetzler RF, et al. Anatomy of the mastoid emissary vein and venous system of the posterior neck region: Neurosurgical implications. Neurosurgery. 2007;61(5 Suppl 2):193–201. doi: 10.1227/01.neu.0000303217.53607.d9. [DOI] [PubMed] [Google Scholar]
- 15.Rivet DJ, Goddard JK, 3rd, Rich KM, Derdeyn CP. Percutaneous transvenous embolization of a dural arteriovenous fistula through a mastoid emissary vein. Technical note. J Neurosurg. 2006;105:636–9. doi: 10.3171/jns.2006.105.4.636. [DOI] [PubMed] [Google Scholar]
- 16.Forte V, Turner A, Liu P. Objective tinnitus associated with abnormal mastoid emissary vein. J Otolaryngol. 1989;18:232–5. [PubMed] [Google Scholar]
- 17.Lambert PR, Cantrell RW. Objective tinnitus in association with an abnormal posterior condylar emissary vein. Am J Otol. 1986;7:204–7. [PubMed] [Google Scholar]
- 18.An YH, Wee JH, Han KH, Kim YH. Two cases of petrosquamosal sinus in the temporal bone presented as perioperative finding. Laryngoscope. 2011;121:381–4. doi: 10.1002/lary.21369. [DOI] [PubMed] [Google Scholar]