

Abstract
Aims:
To compare the quality of vision in pseudophakic patients implanted with aspherical and spherical intraocular lenses (IOLs).
Materials and Methods:
Randomized prospective longitudinal intrapatient comparison between aspherical and spherical IOLs performed on 22 patients who underwent bilateral cataract surgery. Best corrected visual acuity, subjective contrast sensitivity, Strehl ratio and spherical aberrations (SA), and higher order wavefront aberrations for a 3.5 mm and a 6.0 mm pupil were measured after 3 months of cataract surgery.
Results:
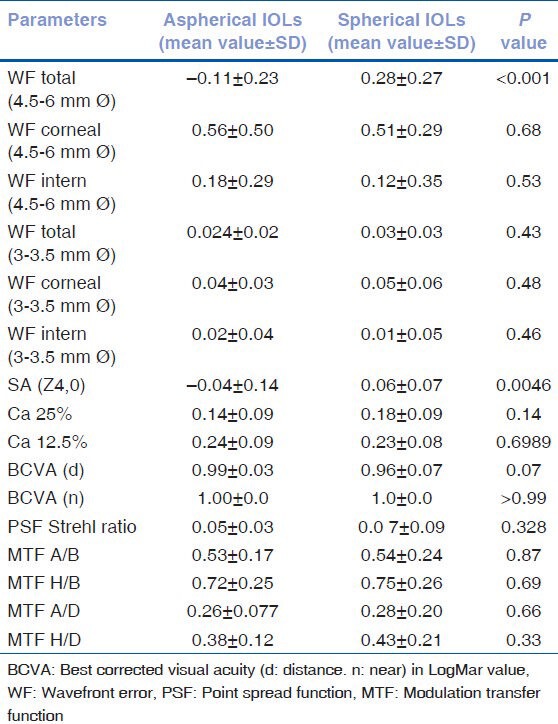
SA (Z4,0) decreased significantly in eyes with aspherical IOL implant (P =0.004). Modulation transfer function (MTF) and point spread function (PSF) resulted no significant difference between the two groups (P =0.87; P = 0.32).
Conclusion:
Although the SA is significantly lower in eyes implanted with aspherical IOL, the quality of vision determined with MTF and PSF does not significantly differ for subjective and objective parameters that were analyzed.
Keywords: Aspherical intraocular lens, quality of vision, spherical aberrations
The crystalline lens and the cornea of the human eye play an important role in determining the total ocular spherical aberrations (SA). In healthy young individuals, the negative SA of the lens is partially compensated by the positive corneal SA, resulting in a low level of SA for the entire eye. With aging, the SA of the lens becomes positive and, added to the corneal SA, it increases the total aberration of the eye.[1,2,3,4]
The spherical intraocular lens (IOL) implant after cataract surgery has a tendency to increase the overall positive SA. Standard IOLs have a positive SA, which, increasing the total SA, produces a pseudophakic eye with a total aberration not better than that recorded in an aged eye with transparent lens.[4]
In this prospective study, we analyzed the visual performance of both eyes of 22 patients who underwent bilateral cataract surgery, implanted in one eye with an aspherical IOL, whereas the contralateral received the same standard type of spherical IOL. The aim of this work was to verify the quality of vision and the contrast sensitivity, throughout subjective and objective tests, after implantation of spherical and aspherical IOLs.
Materials and Methods
Subjects
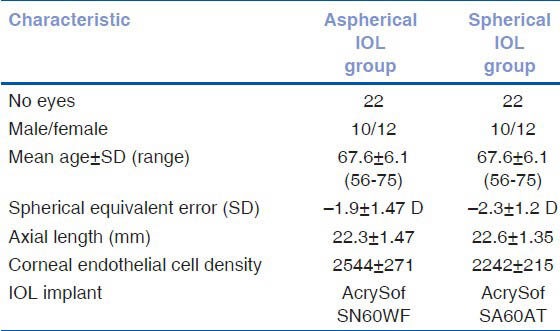
Forty-four eyes of 22 patients who underwent bilateral cataract surgery were recruited prospectively from August 2007 to October 2008. The exclusion criteria were: age less than 50 years, severe systemic disease, pregnancy, any uncontrolled ocular disease, presence of ocular pathology other than cataract, and previous history of ocular surgery. Patients with incomplete follow-up were also excluded. The patients received an aspherical IOL (AcrySof IQSN60WF, Alcon Laboratories Inc. Fort Worth, TX) in one eye and the same standard spherical IOL (AcrySof SA60AT; Alcon Laboratories Inc) in the other eye. Demographic characteristics of patients are summarized in Table 1.
Table 1.
Demographic characteristics of study
Contrast sensitivity has been tested by CSV-1000E, Vector Vision, Arcanum, OH, USA (25% and 12.5% contrast level) at 6 and 12 cycles per degree. Every patient was examined with the best spectacle correction under mesopic conditions. Measurements of ocular wavefront error were performed 3 months after cataract surgery using the OPD Scan-II aberrometer/topographer NIDEK Co Ltd, Gamagori, Japan. We analyzed total, corneal, and internal wavefront errors for pupil diameters of 3.5 and 6 mm focusing mainly on SA (Z4,0).
Vision quality has been expressed by the point spread function (PSF) and the modulation transfer function (MTF). The PSF describes the light distribution on the retina of a point source and it can be expressed with the Strehl ratio. The Strehl ratio expresses the ability of the eye to produce a point imagev on the retina when a point object is observed.[5]
The MTF is reported as a percentage of the contrast of the image that is transmitted to the retina at various spatial frequencies.[5] We also calculated MTF A/B ratio (the area ratio of the MTF curve of the examined eye over the MTF curve of the ideal eye) and MTF H/B ratio (the area ratio of the MTF curve of the examined eye without low-order aberrations over the MTF curve of the ideal eye). We analyzed the Strehl ratio and the MTF graph with a 4.5 mm pupil and 6th Zernike order of aberrations. A P ≤ 0.05 was considered to be significant.
Results
The mean age of the 22 patients was 67.6 years, 6.1 SD (range: 56-75). Demographic characteristics of patients are summarized in Table 1.
The results of contrast sensitivity testing, under mesopic conditions at 25% and 12.5% contrast, showed that there was no statistically significant difference between the groups (P =0.14; P = 0.69).
Aberration (Z4 [4,0]) (Zernike term no. 12), for a 4.5 mm optical zone diameter, decreased significantly in eyes with aspheric IOL implant (P =0.004).
The two groups were significantly different in terms of Zernike values for total (P < 0.001), whereas no difference was recorded for internal (P =0.53) wavefront error for 3.5 and 6 mm diameter pupil analysis. The results of MTF and PSF Strehl ratio were not significantly different for two groups (P =0.87; P = 0.32). The results are summarized in Table 2.
Table 2.
Difference between aspheric and standard spherical intra ocular lenses regard to subjective and objective parameters analyzed. For some patients a pupil diameter of 6 mm was obtained after instillation of mydriatic eye drops (phenylephrine). Value of the ratio close to 1 describes few aberrations and more image contrast
Discussion
The SA is a symmetrical axial aberration in which the light rays that pass through the paraxial zone of the pupil focus at a different distance where the rays that pass through the marginal pupil.
The SA of the anterior corneal surface is added to that of the posterior surface and that of the IOL. These will tend to compensate if they are of opposite signs.[4] In theory, the use of IOLs with modified aspheric surface profile should be able to compensate the positive SA in order to increase the quality of vision.
In a recent prospective randomized study on 31 patients, Ohtani et al.[6] compared aspheric and spherical silicone IOLs. The author reported significantly reduced ocular SA, but no significant differences between IOLs with regard all-distance visual acuity and ocular wavefront aberrations except for fourth-order Root Mean Square (RMS) (SA [Z4,0]).
Kim et al.[7] reported a better contrast sensitivity at 3-6 cycles per degree (cpd) in photopic and 1.5-6 cpd in mesopic conditions for 23 eyes implanted with aspheric (Tecnis ZA9003, Advanced Medical Optics, Santa Ana, CA) IOL. The author has found similar results in terms of other Zernike values and RMS of higher order wavefront aberrations, whereas MTF curve was better for the aspherical IOL group at 5-10 cpd.
Nabh et al.[8] reported a significantly decreased positive spherical ocular aberration after three different aspheric IOL implants, with no differences regarding contrast sensitivity and visual performance between the lenses. If the overall SA is not excessive, there will be a slight loss in contrast, with an improvement in the depth of the field due to the multifocal effect of the SA.[9]
In our prospective series, a significant lower SA in the eyes implanted with aspherical IOL as compared to the spherical ones, without any real gain in terms of vision, was detected. We have also found a significant difference between the groups for total aberrations, whereas no differences were found regarding internal aberrations. We believe that the decentration of aspherical IOL may induce an increase in total aberrations no more compensated by corneal aberrations. In respect to the parameters analyzed for the quality of vision (best corrected visual acuity, PSF, MTF), there were no differences between aspherical IOL and standard type of spherical IOL.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Smith G, Cox MJ, Calver R, Garner LF. The spherical aberration of the crystalline lens of the human eye. Vision Res. 2001;41:235–43. doi: 10.1016/s0042-6989(00)00206-6. [DOI] [PubMed] [Google Scholar]
- 2.Glasser A, Campbell MC. Presbyopia and the optical changes in the human crystalline lens with age. Vision Res. 1998;38:209–29. doi: 10.1016/s0042-6989(97)00102-8. [DOI] [PubMed] [Google Scholar]
- 3.Artal P, Berrio E, Guirao A, Piers P. Contribution of the cornea and internal surfaces to the change of ocular aberrations with age. J Opt Soc Am A Opt Image Sci Vis. 2002;19:137–43. doi: 10.1364/josaa.19.000137. [DOI] [PubMed] [Google Scholar]
- 4.Calossi A. Corneal asphericity and spherical aberration. J Refract Surg. 2007;23:505–14. doi: 10.3928/1081-597X-20070501-15. [DOI] [PubMed] [Google Scholar]
- 5.Bellucci R, Morselli S, Piers P. Comparison of wavefront aberrations and optical quality of eyes implanted with five different intraocular lenses. J Refract Surg. 2004;20:297–306. doi: 10.3928/1081-597X-20040701-01. [DOI] [PubMed] [Google Scholar]
- 6.Ohtani S, Gekka S, Honbou M, Kataoka Y, Minami K, Miyata K, et al. One-year prospective intrapatient comparison of aspherical and spherical intraocular lenses in patients with bilateral cataract. Am J Ophthalmol. 2009;147:984–9. doi: 10.1016/j.ajo.2008.12.037. [DOI] [PubMed] [Google Scholar]
- 7.Kim SW, Ahn H, Kim EK, Kim TI. Comparison of higher order aberrations in eyes with aspherical or spherical intraocular lenses. Eye (Lond) 2008;22:1493–8. doi: 10.1038/eye.2008.302. [DOI] [PubMed] [Google Scholar]
- 8.Nabh R, Ram J, Pandav SS, Gupta A. Visual performance and contrast sensitivity after phacoemulsification with implantation of aspheric foldable intraocular lenses. J Cataract Refract Surg. 2009;35:347–53. doi: 10.1016/j.jcrs.2008.10.043. [DOI] [PubMed] [Google Scholar]
- 9.Nio YK, Jansonius NM, Fidler V, Geraghty E, Norrby S, Kooijman AC. Spherical and irregular aberrations are important for the optimal performance of the human eye. Ophthalmic Physiol Opt. 2002;22:103–12. doi: 10.1046/j.1475-1313.2002.00019.x. [DOI] [PubMed] [Google Scholar]