

Abstract
Perioperative visual loss (POVL), a rare but devastating complication, has been reported after spine, cardiac, and head-neck surgeries. The various causes include ischemic optic neuropathy, central or branch retinal artery occlusion, and cortical blindness. The contributory factors described are microvascular diseases and intraoperative hemodynamic compromise. However, the exact association of these factors with post-operative blindness has not yet been confirmed. A case of POVL with caesarian section surgery is being presented. The visual loss occurred due to a combined occlusion of central retinal artery and vein. The causes, presentation, and risk factors of POVL after non-ocular surgery are being discussed.
Keywords: Caesarian section, combined occlusion, non-ocular surgery, perioperative visual loss
Perioperative visual loss (POVL) accompanying non-ocular surgery is a rare but potentially devastating complication. It is usually due to ischemic optic neuropathy, retinal artery occlusion, or cortical blindness. Most cases are reported with spinal and cardiac surgeries.[1] A case of vision loss associated with caesarian section surgery is being presented here. The fundus picture as well as fundus fluorescein angiography suggested a combined occlusion of central retinal artery and vein. A brief review of literature on POVL associated with non-ocular surgery is also being presented.
Case Report
A 20-year-old lady presented with complaints of sudden loss of vision in the left eye (LE), immediately following caesarian section surgery. The patient had no ocular complaints prior to surgery. The surgery was done under spinal anesthesia and was uneventful. On presentation, 5 days after surgery, patient had visual acuity of 20/20 in the right eye and no perception of light in the LE. External ocular examination showed a relative afferent pupillary defect in the LE with no other abnormality noticed in both eyes.
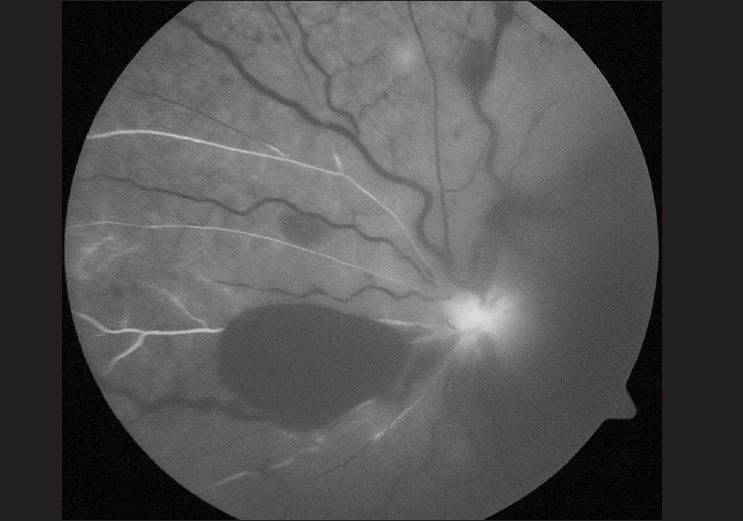
Fundus examination of the right eye was normal, whereasthe LE showed a clear media, with hyperemic disc having blurred margins. Arteries showed severe narrowing, whereas veins were grossly engorged. There were several pre-retinal and blot retinal hemorrhages. Two days later, the pre-retinal hemorrhage on the temporal side had leaked into the vitreous. [Fig. 1].
Figure 1.

Fundus photograph of the left eye, showing grossly dilated veins, pre-retinal hemorrhages, and vitreous hemorrhage
Fundus fluorescein angiography showed grossly delayed filling of vessels on nasal side with absence of perfusion in rest of the vessels. Temporal view was obscured due to vitreous hemorrhage[Fig. 2]. Carotid Doppler study was normal while Doppler study of central retinal artery and vein showed absence of perfusionbeyond the optic disc [Fig. 3]. Systemic examination was normal, except signs of anemia.
Figure 2.
Fundus fluorescein angiography at 14 s showing blocked fluorescein due to pre-retinal hemorrhage, filling of nasal vessels, and non-perfusion of rest of the vessels
Figure 3.
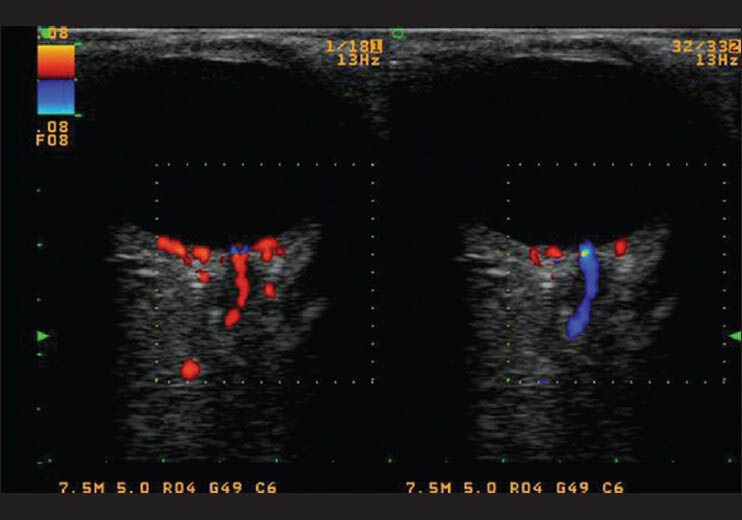
Doppler study showing normal filling of vessels in the right eye, whereasthe left eyeshows no filling of central retinal artery with filling of the central retinal vein
Her pre-operative records were reviewed, which revealed hemoglobin of 7.5 gm% prior to surgery She also had borderline hypertension. The surgery was done under high risk due to thick meconium and fetal distress (the baby died due to meconium aspiration, following surgery). During surgery, she received 3,000 ml of fluids. On the day after surgery, her hemoglobin reduced to 5.6 gm% and was administered two units of blood in the post-operative period. Other counts were normal (except total proteins, 4.1 g/dl). Sickling test was negative.
On the basis of fundus picture and fluorescein angiographic findings, the patient was diagnosed to have combined occlusion of central retinal artery and vein. Due to risk of neovascularization, she was advised to undergo a panretinal photocoagulation. She was subsequently lost to follow-up.
Discussion
Visual loss after non-ocular surgery, though rare, can be a devastating complication. The incidence of POVL is estimated to be around 0.013% for all surgeriesand up to 0.2% followingspine surgery.[2] Cardiac, spinal as well as head and neck surgeries have been associated with POVL. The main reported causes are ischemic optic neuropathy, central retinal artery occlusion, and cortical blindness. Optic nerve ischemia is the most common mechanism of injury. Posterior ischemic optic neuropathy is more commonly reported after spinal surgeries, whereas anterior ischemic optic neuropathy is more prevalent after cardiac surgery.[3]
Although the etiology of POVL is not properly understood, multiple factors have been proposed as risk factors. These include decreased ocular perfusion pressure, excessive blood loss and anemia, hypotension, hypoxia, excessive fluid replacement, elevated venous pressure, head positioning, and patient-specificvascularsusceptibility.[3] POVL due to ischemic optic neuropathy is typically noticed within the first 24-48 h, frequently when the patient awakes after surgery. Hypotension, blood loss, lengthy surgery, and large quantities of fluid administration may occur in many patients undergoing complex spinal surgery. These together with abnormal autoregulation in the posterior optic nerve and other patient-specific factors may predispose to decreased oxygen delivery to the optic nerve leading to ischemic injury.[4]
Branch and central retinal vein occlusion may sometimes occur in the post-operative period either from external pressure from improper head positioning or due to increased internal pressure from retrobulbar hemorrhage. Retinal emboli may also be a potential cause. Rarely, hypotension may be the culprit.[4]
Our case presented with a combined occlusion of central retinal artery and vein which has not been previously reported as a cause of POVL to the best of our knowledge.
The overall visual outcome of POVL, in general, is very poor owing to limited treatment options and unclear pathogenesis. There are no definite clinical trials to show a direct causal relationship between some patient-related factors and intraoperative situations with the occurrence of POVL. Several studies have linked the association of POVL with some pre-operative and intraoperative risk factors. The pre-operative factors often associatedare anemia, hypertension, glaucoma, carotid artery disease, smoking, obesity, and diabetes.[2] Intraoperatively, many factors have been proposed which include long duration in the prone position, decreased oxygen perfusion pressure, excessive blood loss and anemia, hypotension, hypoxia, excessive fluid replacement, elevated venous pressure, head positioning, and patient-specific vascular susceptibility which may be anatomic or physiologic. However, the risk factors for any given patient or procedure may vary.[5] Our patient had a pre-operative anemia, and intraoperatively, suffered significant blood loss as is evident by furtherdecrease inhemoglobin level post-operatively. She also received significant quantities of fluids intraoperatively. A resultant compartment syndrome at the optic nerve head may be a likely explanation for the combined occlusion. Pregnancy-induced hypercoagulability might be a contributing factor. Investigations pointing to coagulation disorders such as estimation of Proteins C and S, and anti-thrombin levels could have helped in proving this etiology. Systemic lupus erythematosuses specially in the presence of anti-phospholipid antibody, is another possibility, particularly in young individuals.
Rarity of the condition as well as lack of definite causal risk factors may be responsible for inability to prevent the occurrence of this complication. Measures such as thorough pre-operative evaluation and preparation, intraoperative patient positioning, proper management of intravenous fluids, correction of anemia, use of vasopressors, maintaining blood pressure during surgery, and optimization of duration of surgery have beenproposed by American Society of Anesthesiologists Task Force, to avoid perioperative blindness in patients undergoing spine surgery under general anesthesia.[6] Similar precautions taken in other surgeries as well, might decrease the incidence of this devastating complication.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Grover V, Jangra K. Perioperative vision loss: A complication to watch out. J Anaesthesiol Clin Pharmacol. 2012;28:11–6. doi: 10.4103/0970-9185.92427. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Berg KT, Harrison AR, Lee MS. Perioperative visual loss in ocular and nonocular surgery. Clin Ophthalmol. 2010;4:531–46. doi: 10.2147/opth.s9262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kawaguchi M, Hayashi H, Kurita N, Furuya H. Postoperative visual disturbances after non-ophthalmic surgery. Masui. 2009;58:952–61. [PubMed] [Google Scholar]
- 4.Roth S. Perioperative visual loss: What do we know, what can we do? Br J Anaesth. 2009;103:i31–40. doi: 10.1093/bja/aep295. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Shmygalev S, Heller AR. Perioperative visual loss after nonocular surgery. Anaesthesist. 2011;60:683–94. doi: 10.1007/s00101-011-1908-x. [DOI] [PubMed] [Google Scholar]
- 6.American Society of Anesthesiologists Task Force on Perioperative Visual Loss. Practice advisory for perioperative visual loss associated with spine surgery: An updated report by the American Society of Anesthesiologists Task Force on Perioperative Visual Loss. Anesthesiology. 2012;116:274–85. doi: 10.1097/ALN.0b013e31823c104d. [DOI] [PubMed] [Google Scholar]