

Abstract
INTRODUCTION
Follicular carcinoma of thyroid usually behaves in an indolent manner with low metastatic potential. Distant metastases as initial presentation is rare in follicular carcinoma; especially in young patients.
PRESENTATION OF CASE
We report the clinical, pathological features and the management of three different cases of follicular carcinoma of the thyroid with unusual presentations at the time of diagnosis. First case presented as thyroid abscess, second case with a large skull swelling in a pre-exiting goiter and the third case with a swelling in the sternum.
DISCUSSION
Follicular carcinoma of thyroid is the second category of well-differentiated thyroid cancer that constitutes about 10% of all thyroid malignancies. Blood borne metastasis is common with spread to lung, bone and other solid organs. In less than 10% cases of follicular carcinoma, there is evidence of lymphatic involvement. The patients’ presentations above are highly unusual.
CONCLUSION
Recognizing these cases has a significant impact on clinical decision-making and prognosis of the patients. Treatment in these patients should be individualized and an alternative therapeutic approach should be considered.
1. Introduction
Papillary (PTC) and follicular (FTC) thyroid carcinomas are follicular cell-derived carcinomas. They are differentiated forms of thyroid carcinoma and are characterized by slow growth and an indolent biological behavior. These cancers usually remain localized in the thyroid gland. Follicular thyroid carcinoma is the second most common thyroid cancer after papillary carcinoma. It accounts for 10–20% of all thyroid malignancies and is most often seen in patients over 40 years of age.1 The tumor usually presents as an asymptomatic solitary thyroid nodule. These neoplasms tend to metastasize hematogenously, with lung and bone most commonly affected,2 while distant metastases at the time of diagnosis are reported in 11–20% of patients.3 Less than 1% of these cases are seen in patients younger than 45 years of age.4 There have been a few case reports of follicular carcinoma causing unusual bony metastases, such as skull,5 mandible,6 maxilla,7 spine,8 and orbit.9 Sometimes, the metastatic focus may be the presenting feature. When combined with distant especially widespread metastases, the quality of life is compromised and the overall survival rate significantly decreases. Hence management of follicular carcinoma requires special attentions and knowledge about its metastatic potential and its effect. Eighty percent of differentiated thyroid carcinoma (DTC) patients respond to total thyroidectomy, radioiodine-131 (131I) ablation and levothyroxine suppression treatment.10 We discuss here the unusual presentations of these cases of follicular thyroid carcinoma and their difficult management.
2. Case series
We have described three cases of follicular Carcinoma of thyroid with unusual presentations. First case presented as thyroid abscess, second case presented with a large skull swelling in a pre-exiting goiter, and the third case presented with a swelling in the sternum. The first case was a 25 year old lady having a pre-existing goiter for 5 years (Fig. 1). She was diagnosed as follicular adenoma by fine needle aspiration cytology (FNAC) 2 years back but refused for surgery. She came with sudden onset of pain, swelling, fever with chill & rigor, redness, erythema and tenderness over the swelling and dysphagia. She was treated with a complete course of antibiotic based on culture sensitivity. On ultrasonography only cystic component was found and subsequently underwent hemithyroidectomy which came out to be follicular carcinoma of thyroid. Second Case was a 40 yr old lady, had a pre-existing Goiter for last 10 years. She was on regular follow up by an endocrinologist. She developed a swelling on the left parietal region of the skull for last one year, gradually increasing in size for which she reported to us. On examination, a globular hard swelling of size about 2 cm × 4 cm × 4 cm situated on left parietal bone of her skull (Fig. 2a). An incisional biopsy was performed. The histopathological examination revealed thyroid follicles filled with colloid material which is positive for PAS stain. The cells surrounding the follicles were intensely positive for thyroglobulin. The interpretation was metastatic follicular carcinoma of the thyroid. X-ray and Magnetic resonance imaging (MRI) of skull showed bone destruction with intracerebral extension (Fig. 2b,d,e). She underwent total thyroidectomy and the histopathology of the specimen showed follicular carcinoma with lymphovascular invasion (Fig. 2c). Then the patient was referred to radiotherapy department for radioiodine therapy. Third case was a 45 year old lady presented with a Solitary thyroid nodule (STN) on left lobe of thyroid, left hemithyroidectomy was done based upon FNAC report as follicular adenoma. Two years later patient presented with a swelling on right lobe of thyroid with a swelling on the sternum (Fig. 3). Core needle biopsy from the sternal growth comes out as metastatic follicular carcinoma. She underwent completion thyroidectomy with radioiodine therapy.
Fig. 1.
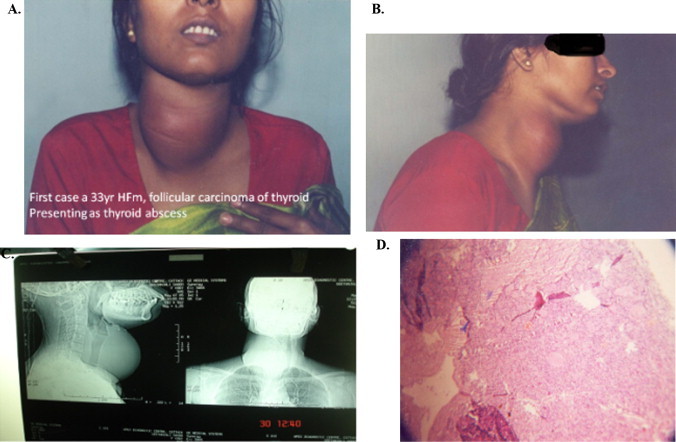
First case, a 25 yr female of follicular carcinoma of thyroid presenting as thyroid abscess.
Fig. 2.
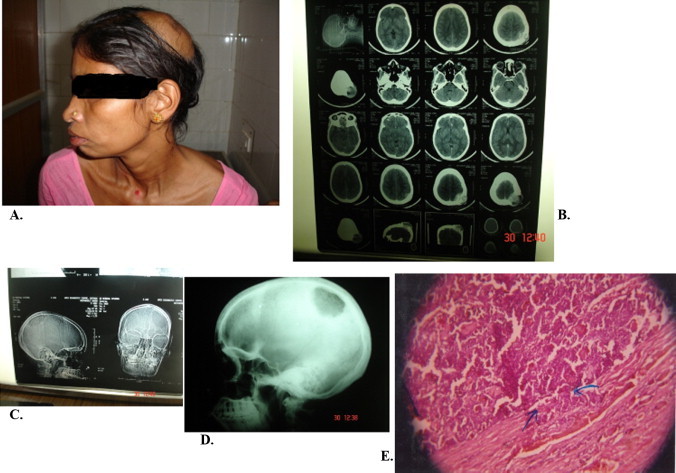
(A) Second case, a 40 yr old lady with metastasis over skull bone (B)–(D) CT head showing large fronto-parietal mass eroding through the skull, and extending into the scalp and intracranially. (E) Histopathology showing follicular carcinoma with lymphovascular invasion.
Fig. 3.
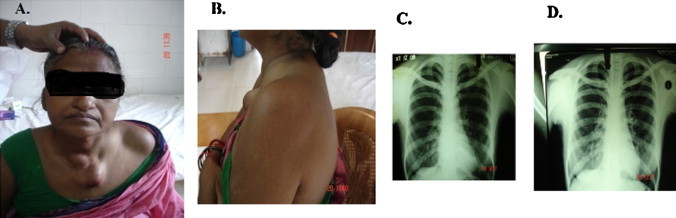
Third case, a 45 year old lady with follicular carcinoma thyroid with sternal metastasis.
3. Result
First case was a minimally invasive follicular carcinoma and hemithyroidectomy was appropriate extent of surgical excision. She was on suppressive dose of Thyroxine and doing well in 3 years follow up. In the 2nd case after total thyroidectomy and radioiodine treatment the skull swelling disappeared, on follow up of 1 year she had hemoptysis. Computed tomography (CT) scan of chest showed bilateral chest metastatic nodules. The patient is now on chest external beam radiation therapy (EBRT). In the third case after total thyroidectomy and radioiodine therapy there was no recurrence of the tumor on follow up of 2 years.
4. Discussion
Follicular carcinoma is the second most prevalent of the thyroid carcinomas with an incidence of approximately 10–15%. Blood borne metastasis is common with spread to lung, bone and other solid organs. In less than 10% cases of follicular carcinoma, there is evidence of lymphatic involvement.11 Patients with differentiated thyroid carcinoma (DTC) have a 10-year survival rate of 80–95%. However, when distant metastases are present, the overall 10-year survival rate is 40%.12 The patients’ presentations above are highly unusual.
Thyroid abscess and acute supporative thyroiditis are not common, presenting only 0.1–0.7% of surgically treated thyroid pathologies.13 Infection of the thyroid gland are rare due to its isolated anatomic location, fibrous capsule, rich blood supply, generous lymphatic drainage, and high content of iodine. However, various factors like congenital pyriform sinus, thyroid/neck injury, blood-borne infections, surrounding infections and intrinsic gland pathology like nodular goiter, thyroid cyst, and papillary thyroid cancer may predispose to suppurative thyroiditis.14 Infection in pre-existing thyroid pathology may present with localized thyroid abscess. In the first case, the underlying pathology was solitary thyroid nodule and FNAC revealed follicular adenoma. After 2 years, the patient presented with thyroid abscess. Hemithyroidectomy was done and biopsy showed follicular carcinoma.
Bone metastases from DTC occur in 2–13% of patients. When bone metastases are present, the overall survival at 10 years was reported to range from 13 to 21%.15 The study of Durante et al. (2006) found 44% of bone metastases in 444 metastatic DTC patients. They are more frequent in Follicular thyroid carcinoma (7–28%) compared with Papillary thyroid carcinoma (1.4–7%). The bones most often involved in metastasis of follicular carcinoma are the long bones, such as the femur and flat bones, particularly the pelvis and sternum.16 It is not unusual for a pathological break of a long bone to be the first clinically significant manifestation of follicular thyroid carcinoma. The second case was being followed up by an endocrinologist who aggressively worked up the patient for the benign lesions of the thyroid over a period of two-years, but had significant metastasis in the left parietal region of the skull that measured about 2 cm × 4 cm × 4 cm in size. Research indicates that treatment with radioactive iodine improves survival for patients with thyroid cancer that has spread to nearby lymph nodes or to distant locations in the body.17 The patient underwent total thyroidectomy followed by radioiodine therapy.
The staging of follicular thyroid carcinoma is differentiated from the standpoint of the age of the patient. There are two categories: older than 45 years of age and younger than 45 years of age. Staging of patients who are younger than 45 years of age is quite simple; if the carcinoma is confined to only the thyroid with no lymph node involvement or metastasis, it is stage I. In our patient, who had distant metastasis, the carcinoma would be considered stage II. This method of staging is the tumor, node, metastasis method (TNM method) and is the official method of staging adopted by the American Joint Commission on Cancer. In cases of metastatic disease to lung and/or bone, adverse prognostic factors are said to include multiplicity of sites, older patient age at the time of discovery of the metastases, and absence of radioactive iodine uptake by the metastases.18
The extent of metastatic disease to bone and its response to radioactive iodine are associated with survival.19 A retrospective study evaluated therapeutic outcome, total administered radioiodine activities, and side effects (blood count alterations grades I–IV, WHO classification, and acute leukemia) in 107 patients with initial bone metastases. This study concluded that initial bone metastases in selected DTC patients up to 45 years and especially in those with less than three bone metastases can be treated with curative intent.20
5. Conclusion
Although the incidence of papillary thyroid carcinoma is much higher than of follicular carcinoma, the later accounts for more deaths. Follicular carcinoma differs from papillary in that it occurs at an older age, exhibits hematogenous spread rather than lymphatic dissemination, and has a more aggressive behavior. So total thyroidectomy with adjuvent radioiodine therapy remains the standard of treatment for follicular carcinoma thyroid. Disseminated metastases from follicular carcinoma at the time of diagnosis in a young patient remain exceedingly rare. Even if it is advanced and metastatic, can be managed adequately with proper modalities of treatment.
Conflict of interest
None.
Funding
None.
Ethical approval
Obtained.
Author contributions
Sangram Keshari Panda – study design and data analysis; K.C. Mohapatra and Jagadananda Mishra – data collection and writing; R.K. Meher – study design; Byomokesh Patro – writing; Manas Ranjan Samantaroy – data analysis and writing.
Contributor Information
Sangram Keshari Panda, Email: drsangram83@gmail.com.
Jagadananda Mishra, Email: drjnms@gmail.com.
References
- 1.Mazzaferri E.L. Papillary and follicular thyroid cancer: a selective approach to diagnosis and treatment. Annu Rev Med. 1981;32:73–91. doi: 10.1146/annurev.me.32.020181.000445. [DOI] [PubMed] [Google Scholar]
- 2.Courtney M., Townsend R., Daniel Beauchamp, Mark Evers B., Mattox K.L. 19th ed. An imprint of Elsevier; Philadelphia: 2012. Thyroid; Sabiston textbook of surgery; p. 911. [Google Scholar]
- 3.Schlumberger M., Tubiana M., De Vathaire F. Long-term results of treatment of 283 patients with lung and bone metastases from differentiated thyroid carcinoma. J Clin Endocrinol Metab. 1986;63:960–967. doi: 10.1210/jcem-63-4-960. [DOI] [PubMed] [Google Scholar]
- 4.Shaha A.R., Shah J.P., Loree T.R. Differentiated thyroid cancer presenting initially with distant metastasis. Am J Surg. 1997;174:474–476. doi: 10.1016/s0002-9610(97)00158-x. [DOI] [PubMed] [Google Scholar]
- 5.Ozdemir N., Senoglu M., Acar U.D., Canda M.S. Skull metastasis of follicular thyroid carcinoma. Acta Neurochir (Wien) 2004;146:1155–1158. doi: 10.1007/s00701-004-0290-8. [DOI] [PubMed] [Google Scholar]
- 6.Anil S., Lal P.M., Gill D.S., Beena V.T. Metastasis of thyroid carcinoma to the mandible, Case report. Aust Dent J. 1999;44:56–57. doi: 10.1111/j.1834-7819.1999.tb00537.x. [DOI] [PubMed] [Google Scholar]
- 7.Hefer T., Manor R., Zvi Joachims H. Metastatic follicular thyroid carcinoma to the maxilla. J Laryngol Otol. 1998;112:69–72. doi: 10.1017/s0022215100139921. [DOI] [PubMed] [Google Scholar]
- 8.Scarrow A.M., Colina J.L., Levy E.I., Welch W.C. Thyroid carcinoma with isolated spinal metastasis: case history and review of the literature. Clin Neurol Neurosurg. 1999;101:245–248. doi: 10.1016/s0303-8467(99)00040-2. [DOI] [PubMed] [Google Scholar]
- 9.Daumerie C., De Potter P., Godfraind C. Orbital metastasis as primary manifestation of thyroid carcinoma. Thyroid. 2000;10:189–192. doi: 10.1089/thy.2000.10.189. [DOI] [PubMed] [Google Scholar]
- 10.Sakamoto A. Definition of poorly differentiated carcinoma of the thyroid: the Japanese experience. Endocr Pathol. 2004;15:307–311. doi: 10.1385/ep:15:4:307. [DOI] [PubMed] [Google Scholar]
- 11.Santacroce L, Gagliardi S: Thyroid, follicular carcinoma. Emedicine.25Sep, 2009. Available at http://emedicine.medscape.com/article/278488-overview (accessed March 30,2010).
- 12.Schlumberger M.J. Papillary and follicular thyroid carcinoma. New England J. Med. 1998;338:297–306. doi: 10.1056/NEJM199801293380506. [DOI] [PubMed] [Google Scholar]
- 13.Menegaux F., Biro G., Schatz C. Thyroid abscess; A propos of 5 cases. Ann. Med. Interne (Paris) 1991;142(2):99–102. [PubMed] [Google Scholar]
- 14.De Sousa R.F., Dilip A., Mervyn C. Thyroid abscess with cutaneous fistula: case report and review of the literature. Thyroid Sci. 2008;3(11):CR1–CR4. [Google Scholar]
- 15.Mc Cormack K.R. Bone metastases from thyroid carcinoma. Cancer. 1966;19:181–184. doi: 10.1002/1097-0142(196602)19:2<181::aid-cncr2820190207>3.0.co;2-2. [DOI] [PubMed] [Google Scholar]
- 16.Nagamine Y., Suzuki J., Katakura R., Yoshimoto T., Matoba N., Takaya K. Skull metastasis of thyroid carcinoma, study of 12 cases. J Neurosurg. 1985;63:526–531. doi: 10.3171/jns.1985.63.4.0526. [PubMed] [DOI] [PubMed] [Google Scholar]
- 17.Podnos Y.D., Smith D., Wagman L.D., Ellenhorn J.D. Radioactive iodine offers survival improvement in patients with follicular carcinoma of the thyroid. Surgery. 2005;128(6):1072–1076. doi: 10.1016/j.surg.2005.09.021. [DOI] [PubMed] [Google Scholar]
- 18.Rosai J, Carcangui ML, Delellis RA: Armed Forces Institute of Pathology; Atlas of Tumor Pathology. Third Series, Fascicle 5. Available at http://www.pathologyresources.com/AFIP/thyroid/tumor04.htm (accessed March 29,2010).
- 19.Lin J.D., Huang M.J., Juang J.H., Chao T.C., Huang B.Y., Chen K.W., Chen J.Y., Li K.L., Chen J.F., Ho Y.S. Factors related to the survival of papillary and follicular thyroid carcinoma patients with distant metastases. Thyroid. 1999;9:1227–1235. doi: 10.1089/thy.1999.9.1227. [DOI] [PubMed] [Google Scholar]
- 20.Petrich T., Widjaja A., Musholt T.J., Hofmann M., Brunkhorst T., Ehrenheim C., Oetting G., Knapp W.H. Outcome after radioiodine therapy in 107 patients with differentiated thyroid carcinoma and initial bone metastases: side-effects and influence of age. Eur J Nucl Med. 2001;28:203–208. doi: 10.1007/s002590000420. [DOI] [PubMed] [Google Scholar]