

Abstract
Oncocytic neoplasms comprise a group of rare tumors of salivary glands. Histologically, World Health Organization (WHO) (1991) classified them into three distinct types: Oncocytosis, oncocytoma and oncocytic carcinoma. Oncocytoma is also known by the more descriptive and less confusing terms of oxyphilic adenoma and oxyphilic granular cell adenoma. Oncocytoma is a rare benign salivary gland neoplasm composed of large epithelial cells with characteristic bright eosinophilic granular cytoplasm (oncocytic cells). It accounts for approximately 0.4-1% of all salivary gland neoplasms, occurring primarily in parotid glands, with only a small percentage occurring in minor salivary glands of palate, tonsillar fossi, larynx, nasal cavity, maxillary sinus and the lacrimal gland. It occurs primarily in persons older than 50 years of age. According to some authors, the biologic behavior of oncocytomas arising from minor salivary glands is that of an aggressive nature and should be considered as low-grade malignancies. Only 17 cases of histologically verified oncocytoma of an intraoral minor salivary gland are reported in literature, the current case being the 18th. Owing to the lack of large series, assiduous study of the cases reported in the literature may lead to better understanding of this rare entity. We herein describe a rare and probably the first case of minor salivary gland oncocytoma involving retromolar area in a 32-year-old female patient with a brief review of literature.
Keywords: Minor salivary gland, oncocytoma, retromolar
INTRODUCTION
Oncocytic neoplasms comprise a group of rare benign neoplasm of salivary glands accounting for approximately 0.4-1% of all salivary gland neoplasms, occurring primarily in parotid glands in persons older than 50 years of age.[1] Oncocytomas are designated as oxyphilic granular adenoma, oxyphilic adenoma and eosinophilic adenoma.[2] Oncocytomas arise very rarely from the minor glands of tonsillar fossi, larynx, nasal cavity, maxillary sinus and the lacrimal gland.[3] Reports of well-documented intraoral lesions arising from minor salivary glands are very rare.
In this report, a case of oncocytoma arising in intraoral minor salivary glands in the right retromolar area of a 32-year-old female patient is presented.
CASE REPORT
A 32-year-old female patient reported with a chief complaint of a large swelling in her right back teeth region since several months. Clinical examination revealed a 2 × 1.5 cm2 in dimensions, well-circumscribed, lobulated and pinkish mass on the right retromolar area [Figure 1]. The swelling was soft in consistency and nontender on palpation. There was no paresthesia, facial asymmetry or regional lymphadenopathy noted. Normal complement of dentition was seen. Provisional diagnosis of irritational fibroma was made. Differential diagnosis included peripheral ossifying fibroma, peripheral giant cell granuloma, pyogenic granuloma, mucocele, lipoma, other benign mesenchymal tumors and benign salivary gland neoplasms. Following written consent from the patient, the growth including the normal surrounding tissue was excised under local anesthesia. Postoperative period was uneventful.
Figure 1.

Intraoral picture revealing a solitary swelling in the retromolar region
Excisional biopsy specimen was fixed in 10% formalin and sent to the Department of Oral Pathology and Microbiology for histopathological examination. Histopathologically, hematoxylin and eosin stained sections revealed a well-circumscribed tumor composed of granular cells that were arranged in solid sheets, alveoli, nests, columns or cords with scattered focal clear cells throughout the tumor tissue, separated by a delicate fibrovascular network [Figure 2]. On higher magnification, the tumor cells were polyhedral to round with distinct cell borders. Abundant cytoplasm, with centrally located nucleus and little mitotic activity were seen [Figure 3]. Features were in favor of oncocytoma rather than fibroma. To confirm the diagnosis, phosphotungstic acid-hematoxylin (PTAH) staining was carried out, which revealed abundant coarse cytoplasmic granules that correspond to abundance of mitochondria [Figure 4]. The final diagnosis was determined as oncocytoma of minor salivary glands of the retromolar area.
Figure 2.
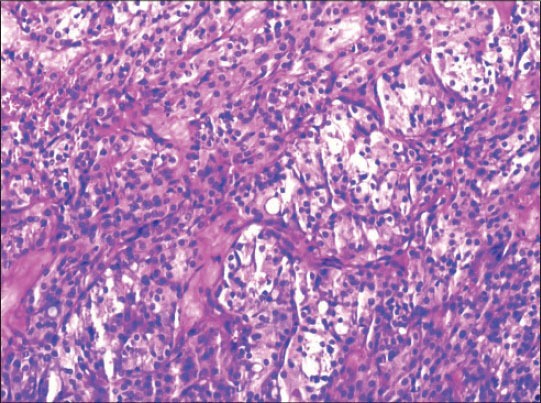
Photomicrograph showing neoplastic cells arranged in solid sheets, nests, columns/cords and separated by fibrovascular network (H&E stain, ×100)
Figure 3.
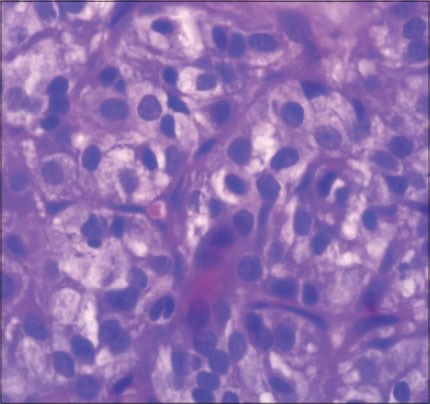
Photomicrograph showing polygonal tumor cells with centrally placed nuclei and abundant dense granular eosinophilic cytoplasm (H&E stain, ×400)
Figure 4.
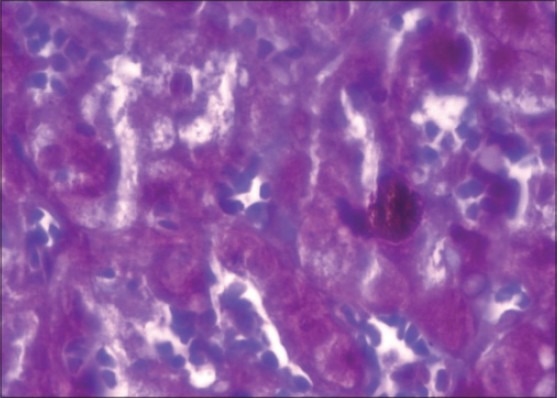
Photomicrograph showing abundant cytoplasmic granules (PTAH stain, ×400). PTAH = Phosphotungstic acid-hematoxylin
DISCUSSION
Oncocytic lesions were described nearly a century ago by Schaffer when he described “granular swollen cells” in the ductal and acinar elements of salivary glands. Although in 1927, McFarland described a tumor as an “adenoma”, without specifically calling it an oncocytoma, the description and illustrations certainly appeared to demonstrate an oncocytoma of the parotid gland.[4]
Hamperl has designated “oncocyte” (from Greek; onkousthai = swollen and cytos = cell) as a special type of epithelial cell characterized by a larger than the original cell, with a mitochondria-rich considerably dense cytoplasm containing acidophilic granules. Oncocytes can be found in normal organs, as in tumors, like major and minor salivary glands, the thyroid, parathyroid, pituitary gland, adrenal gland, gall bladder, uterus, testicle, fallopian tube, pancreas, liver, stomach, kidney, lung, pharynx, trachea and esophagus.[4] The term “oncocytoma” was first introduced by Jaffe in 1932, referring to the lesion currently called adenolymphoma or Warthin's tumor.[5]
The World Health Organization (WHO) (1991) classification of salivary gland neoplasms recognizes three oncocytic entities: Oncocytosis, oncocytoma and oncocytic carcinoma. Oncocytosis is considered to be a hyperplastic change and may present with generalized enlargement of the glands, whereas oncocytoma and oncocytic carcinoma represent neoplastic processes and in agreement with the Armed Forces Institute of Pathology (AFIP) classification, oxyphilic adenoma is considered a benign neoplasia of secretary epithelial origin.[4]
It is generally accepted that for a tumor to be called an oncocytoma, it must comprise exclusively of oncocytes. Even though oncocytes are considered to contain abundant eosinophilic cytoplasm, cases with clear cell changes have been described in the literature.[6]
There are no definitive etiologic factors for this tumor, although there has been an association with radiation in some reports.[6]
Oncocytic changes are noted with increasing age and are almost a universal finding in individuals around the seventh decade of life. Oncocytic changes of secretory epithelia are thought to be metaplastic, a protective phenomenon against adverse change. Hamperl considered oncocytes to be burnt out cells as they lost their original specialization and increased in number with age.[4]
Bonikos DS et al., suggested that oncocytic change may be the result of compensatory mitochondrial hyperplasia in normal cells caused by mitochondrial damage or the exhaustion of one or more mitochondrial enzymes. Linnane et al., advocated that aging caused the accumulation of mitochondrial deoxyribonucleic acid (DNA) errors leading to “mitochondrial respiratory failure and multisystem degeneration”.[4]
Sunmunn et al., stated that oncocytic change could be a regressive alteration of previously hypertrophied or hyperplastic ductal epithelium with the appearance of a mitochondriopathy.[4]
Till date, the PubMed and the Medline search has revealed only 17 reported cases of histologically verified oncocytoma of an intraoral minor salivary gland. The current case is the 18th and the first case to be reported in the retromolar region. Their sex, age and site distribution, together with the current case is summarized in the Table 1.[2,3,5,7]
Table 1.
Reported cases of minor salivary gland oncocytomas
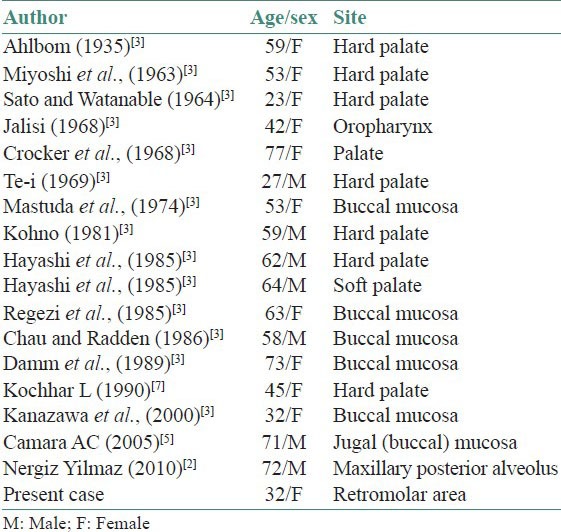
Of the 17 cases reported, 58.8% (10) were women and the age distribution of the reviewed cases at diagnosis varied from 23 to 77 years, with a mean age of 53 years. However, studies of oncocytomas arising in major salivary glands have shown that there is an equal predilection for both sexes and predilection for older individuals, with a peak incidence in the seventh to ninth decades of life. The most frequent site of origin of minor salivary gland oncocytoma is the hard and soft palate (52.9%), followed by buccal mucosa (35.3%).
Microscopically, the tumor is seen as solid cords or clusters of tightly packed oncocytes and a thin strand of fibrovascular stroma is present separating these cells. Scattered lumina of variable sizes, of which some with associated eosinophilic intraluminal secretions may be prominent. The cells are large cuboidal to columnar in shape and are arranged in an organoid pattern with prominent eosinophilic finely granular cytoplasm and round nuclei. The eosinophilia is variable and hence there may be an admixture of light- and dark-stained cells. Occasionally, cystic changes are noted in oxyphilic adenomas.[4] The histological features observed in the present case were satisfactory for the diagnosis as oncocytoma.
Oncocytoma's clinical behavior is generally benign. From their clinical appearance, the lesions were often indistinguishable from other benign tumors as seen in the present case. Most reported cases were treated by surgical excision without recurrence. However, a recurrence rate of 20% has been reported due to incomplete surgical eradication or occult multifocality. For this reason, oncocytomas of the minor salivary glands should be carefully removed, together with a small margin of uninvolved healthy soft tissue, because these lesions occasionally have a thin incomplete capsule and rare malignant cases of oncocytic carcinoma have been reported.[2]
Though the prognosis after tumor excision is excellent, Gray et al., in their review of the literature reported six oncocytomas arising from the seromucous glands in the nasal mucosa or the palate that were more aggressive than the typical oncocytomas but were not malignant. They classified the group as “locally aggressive oncocytomas”, in which local infiltration of the capsule, scattered mitotic figures and focal cellular pleomorphism were seen. According to some authors, the biologic behavior of oncocytomas arising from minor salivary glands in the nasal cavity and maxillary sinuses have an aggressive nature and should be considered as low-grade malignancies.[3]
Oncocytic cells are associated with other definable major salivary gland tumors. Oncocytic differentiation has been observed in pleomorphic adenoma, monomorphic adenoma, basal cell adenoma, canalicular adenoma, myoepithelioma, cystadenoma (lipoadenoma), adenoid cystic carcinoma, acinic cell carcinoma, cystadenocarcinoma, adenocarcinoma and much less frequently in mucoepidermoid carcinoma.[8] Synchronous oncocytoma and Warthin's tumor in the ipsilateral parotid gland has been reported in the literature.[9]
There have been rare examples of malignant oncocytic tumors and the criteria for malignancy includes capsular invasion, destructive growth, necrosis, increased pleomorphism, lymphatic or distant metastasis, vascular/neural invasion and mitotic figures and so forth.[1] Except for few mitotic figures, the above features were absent in the present case.
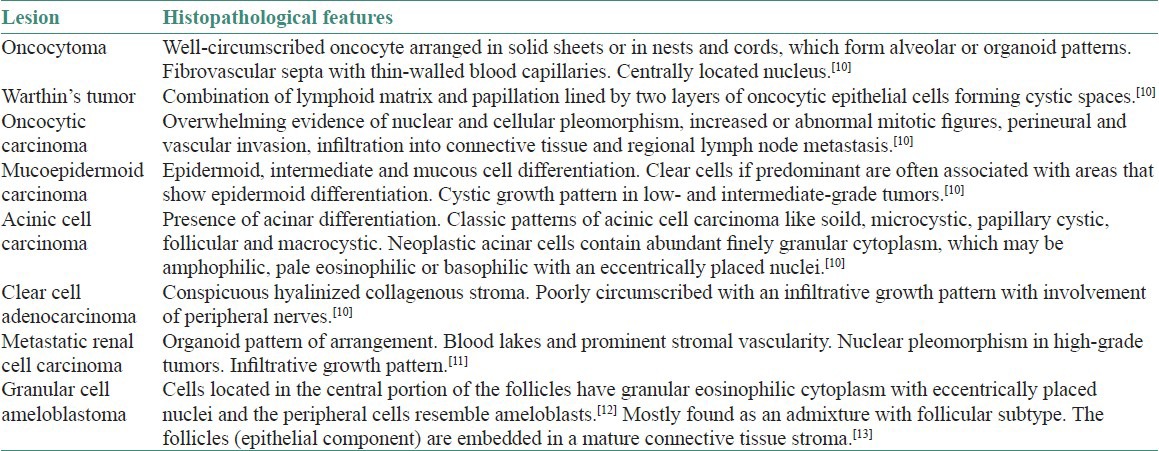
The histological differential diagnosis for oncocytic lesions in the parotid gland include papillary cystadenoma lymphomatosum (Warthin's tumor), acinic cell carcinoma, clear cell carcinoma, oncocytic carcinoma, mucoepidermoid carcinoma, metastatic renal cell carcinoma and granular cell ameloblastoma. The oncocytoma is differentiated from its mimickers by feature enlisted in the Table 2.[10,11,12,13]
Table 2.
Histopathological differential diagnosis of oncocytoma
The clinical, histological and histochemical data from the reported case conform to that in the literature.
CONCLUSION
This oncocytoma of minor salivary gland origin was, to our knowledge, the 18th and the first case to be reported, arising in the right retromolar area. Owing to the lack of large series, industrious study of the cases reported in the literature may lead to better understanding of this rare entity.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Nikumbh DB, Nikumbh RD, Sushama R, Desai SR, Kshirsagar AY, Badwe AS. Oncocytoma of the parotid gland: Cytohistopathological diagnosis with brief review of the literature. Int J Health Sci Res. 2012;114:114–8. [Google Scholar]
- 2.Yilmaz N, Gönülol E, Bereket CM, Karakaş C, Temiz P. An uncommon benign tumor of oral minor salivary glands: A case of oncocytoma. J Dent Fac Atatürk Uni Suppl. 2011;4:77–9. [Google Scholar]
- 3.Kanazawa H, Furuya T, Murano A, Yamaki M. Oncocytoma of an intraoral minor salivary gland: Report of a case and review of literature. J Oral Maxillofac Surg. 2000;58:894–7. doi: 10.1053/joms.2000.8217. [DOI] [PubMed] [Google Scholar]
- 4.Manjunath SM. Oxyphilic adenoma involving floor of the mouth: A case report. Ann Essen Dent. 2011;3:68–70. [Google Scholar]
- 5.Camara AC, Kelner N, Kauffman CM, Lima KP, Henriques AC, de Castro JF. Oncocytoma of an intraoral minor salivary gland: Case report and review of literature. Appl Cancer Res. 2005;25:90–2. [Google Scholar]
- 6.Thompson LD, Wenig BM, Ellis GL. Oncocytomas of the submandibular gland. A series of 22 cases and a review of the literature. Cancer. 1996;78:2281–7. doi: 10.1002/(sici)1097-0142(19961201)78:11<2281::aid-cncr3>3.0.co;2-q. [DOI] [PubMed] [Google Scholar]
- 7.Kochhar L, Kumar S, Deka RC, Bose S. Oncocytoma of the minor salivary glands of hard palate. Indian J Otolaryngol. 1990;42:132–3. [Google Scholar]
- 8.Brannon RB, Willard CC. Oncocytic mucoepidermoid carcinoma of parotid gland origin. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;96:727–33. doi: 10.1016/s1079-2104(03)00377-9. [DOI] [PubMed] [Google Scholar]
- 9.Araki Y, Sakaguchi R. Synchronous oncocytoma and Warthin's tumor in the ipsilateral parotid gland. Auris Nasus Larynx. 2004;31:73–8. doi: 10.1016/j.anl.2003.07.008. [DOI] [PubMed] [Google Scholar]
- 10.Ellis GL, Auclair PL, Gnepp DR. 1st ed. Philadelphia: WB Saunders; 1991. Surgical pathology of the salivary glands. [Google Scholar]
- 11.Prabakaran SS, Chen F, Aguirre A. Oncocytoma of the parotid gland and its mimickers; A comprehensive review. N A J Med Sci. 2010;3:171–80. [Google Scholar]
- 12.Oza N, Agrawal K. Granular cell ameloblastoma mimicking oncocytoma. J Oral Maxillofac Pathol. 2012;16:446–9. doi: 10.4103/0973-029X.102516. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Reichart PA, Philipsen HP. 3rd ed. New Maden, UK: Quintessence Publishing; 2004. Odontogenic tumors and allied lesions; p. 50. [Google Scholar]