

Abstract
Exercise-induced rhabdomyolysis related to military training, marathon running, and other forms of strenuous exercise has been reported. The incidence of acute kidney injury appears to be lower in exercise-induced cases. We present 2 cases of exercise-induced rhabdomyolysis following spinning classes, one of which was further complicated by acute compartment syndrome requiring bilateral fasciotomies of the anterior thigh and acute kidney injury. With vigorous hydration and urine pH monitoring, both patients exhibited good mobility, sensation, and renal function on discharge.
Keywords: rhabdomyolysis, spinning, compartment syndrome, acute kidney injury
Case 1
A 24-year-old woman with no significant medical history presented to the emergency department (ED) complaining of increasing bilateral thigh pain and dark urine. Four days prior, she attended a spinning class for the first time. The patient noted thigh soreness and cramps after the class that progressed relentlessly over 4 days until she could no longer tolerate the pain and presented to the ED. Most of her pain localized to her anterior thighs bilaterally, which she described as “tight as drums.” She also noticed that her urine had become darker.
In the ED, the patient was afebrile, tachycardic to 122 beats per minute, and hypertensive at 133/99 mmHg. On physical examination, the patient was in mild distress and was exquisitely tender to palpation of her anterior thighs and intolerant of any range of motion of her knees because of pain. The anterior compartments of her thighs were palpably tense. She was neurovascularly intact. Admission laboratory results revealed a creatine phosphokinase (CPK) of 161,550 U/L (normal range, 38-234 U/L), an aspartate aminotransferase (AST) of 1983 U/L (normal range, 15-41 U/L), and a creatinine of 0.87 mg/dL (normal range, 0.44-1.03 mg/dL). A diagnosis of rhabdomyolysis was made, and orthopaedic surgery was consulted for possible compartment syndrome.
In the ED, anterior intracompartmental pressures measured 36 mmHg on the left and 24 mmHg on the right. The patient was taken emergently to the operating room for further measurements and likely compartment release. Intraoperative thigh compartment pressure measurements revealed a pressure of 42 mmHg in her left anterior compartment and 28 mmHg in the right. Based on her worsening symptoms, her dramatic clinical examination, significant rhabdomyolysis, and intraoperative pressure measurements, the clinical decision was made to perform emergent bilateral anterior compartment fasciotomies. Once the fascia lata was incised, the quadriceps musculature immediately bulged through the defects (Figure 1). Skin and fascia were left open, and vacuum-assisted closure dressings were placed over both sites. Two days later, primary closure of the skin overlying the fascial releases was performed.
Figure 1.
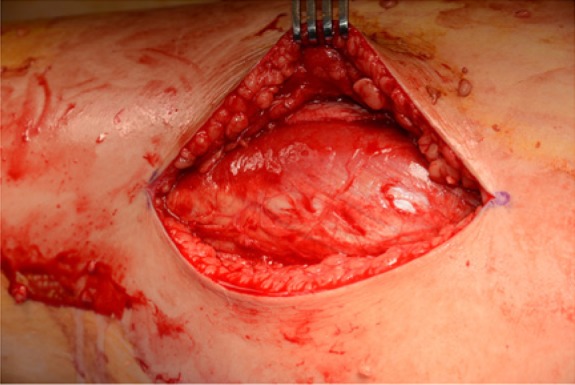
Intraoperative photograph of the left anterior compartment of the thigh. The quadriceps musculature can be seen bulging through the fascial defects.
Immediately after surgery, the patient’s CPK level dropped to 156,199 U/L. Over the following days, intravenous fluids (IVF) were aggressively administered, and her CPK trended down precipitously (Figure 2). Her creatinine, however, increased from 0.87 mg/dL to a maximum of 3.53 mg/dL (Figure 3). With continued hydration and urine pH monitoring, the patient’s creatinine eventually began to decline, and her renal function fully recovered to her baseline without requiring hemodialysis.
Figure 2.
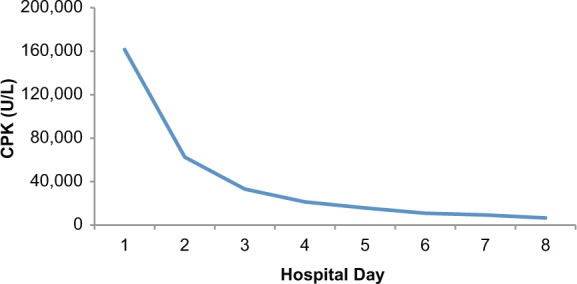
Creatine phosphokinase (CPK) levels for patient 1 by hospital day.
Figure 3.
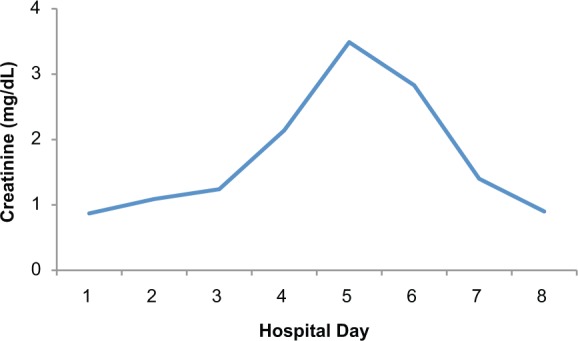
Serum creatinine levels for patient 1 by hospital day.
Case 2
A 24-year-old man with a history of right lower extremity congenital anomalies (absence of the right fifth toe and congenital hypoplasia of the right tibia and fibula, which required multiple reconstructive surgeries as a child) presented after 2 days of worsening thigh pain after his first spinning class. He also noticed that his urine was dark.
He was afebrile with normal vital signs. On physical examination, his thighs were soft to palpation bilaterally. The right foot was cool to touch while the left foot was warm. His posterior tibial pulses were palpable bilaterally; dorsalis pedis pulses were detectable by Doppler signal only. The vascular surgery team was consulted and concluded that there was low suspicion for compartment syndrome given the clinical examination. Laboratory results were notable for a CPK of 14,960 U/L (normal range, 38-234 U/L), AST of 252 U/L (normal range, 15-41 U/L), and creatinine of 0.93 mg/dL (normal range, 0.44-1.03 mg/dL). The patient was started on aggressive IVF hydration with frequent laboratory monitoring. The remaining hospital course was uncomplicated. The patient’s CPK levels progressively declined (Figure 4) and renal function remained stable (Figure 5). Five days later, he was discharged home.
Figure 4.
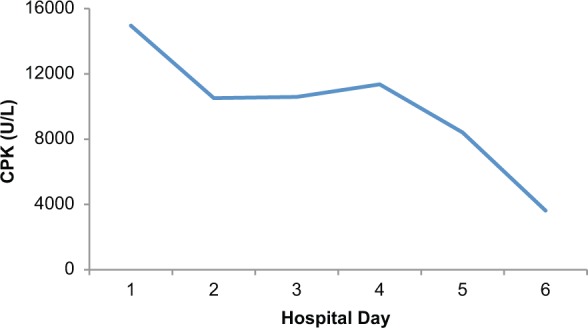
Creatine phosphokinase (CPK) levels for patient 2 by hospital day.
Figure 5.
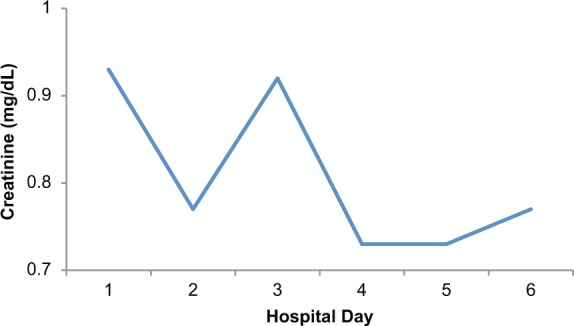
Serum creatinine levels for patient 2 by hospital day.
Discussion
Exertional rhabdomyolysis is the exercise-induced dissolution of skeletal muscle characterized by the leakage of electrolytes, myoglobin, and other sarcoplasmic proteins into the circulation from injured or ischemic muscle cells.4 Exertional rhabdomyolysis has been defined by a constellation of findings, including exercise-associated muscle pain, swelling, dark urine, increased CPK level to at least 5 times the upper limit of normal, and myoglobinuria.9 It should be noted that patient 1 had CPK levels of nearly 700 times the upper limit of normal, and patient 2 had CPK levels of nearly 70 times the upper limit of normal. Also, a urine dipstick that is positive for blood but shows no red blood cells is suggestive of myoglobinuria.2 Following muscle damage, serum myoglobin levels rise.2 Myoglobin is filtered in the glomerulus and will appear in urine when levels exceed 1.5 mg/dL.2 Notable complications include renal failure and compartment syndrome.2,9,11
Acute kidney injury in rhabdomyolysis results from accumulation of myoglobin and other proteins in the renal tubules.10 Myoglobin may form casts within the tubules, leading to obstruction, intrarenal vasoconstriction, and a decrease in the glomerular filtration rate.2 Thirteen cases of exertional rhabdomyolysis in division I football players have been reported requiring hospitalization with admission creatinines as high as 2.6 and 3.4 mg/dL.9
Treatment of exertional rhabdomyolysis begins with aggressive IVF hydration with correction or prevention of electrolyte abnormalities.2 Diuretics such as mannitol are also used to dilute nephrotoxic substances and increase urine flow through the renal tubules.2 Sodium bicarbonate may also be used to alkalinize the urine, and it prevents myoglobin from breaking down into ferrihemate, a nephrotoxic metabolite.2 Treatment should continue until CPK levels decline and the appearance of urine returns to normal.5 When treated early and aggressively, rhabdomyolysis has an excellent prognosis.2 The vast majority of cases will have full recovery of renal function.2 Only 4% of patients with acute kidney injury due to rhabdomyolysis require hemodialysis.2
Compartment syndrome may occur in patients with exercise-induced rhabdomyolysis due to the edema subsequent to muscle injury and tissue damage.6 The fascia that delineates the compartments prevents expansion and causes the intracompartmental pressures to rise.5 Patients often present with severe pain to palpation and passive stretch that is out of proportion.7 Most commonly, compartment syndromes develop in the leg or the forearm.6 The compartments of the thigh are significantly larger than those of the leg or the forearm, allowing for larger volume expansion and greater swelling before reaching critical pressure.6 For this reason, thigh compartment syndrome is quite rare.6 Of the thigh compartments, the anterior is surrounded by the stiffest intermuscular septa and thus is most vulnerable to compartment syndrome.6 Even if the initial clinical examination is negative, serial clinical and laboratory examinations in patients with rhabdomyolysis are recommended to ensure that a developing compartment syndrome is not missed.5 Fasciotomy is the definitive treatment for compartment syndrome of any etiology; however, the decision to perform fasciotomy is not always simple. Compartment pressures greater than 30 to 45 mmHg typically necessitate surgical intervention.2,5 Nevertheless, the decision is a clinical one and cannot be dogmatically based on any one particular measurement.1 In the first case, although the compartment measurement on the right leg was under the general threshold, her clinical picture was severe enough to warrant release. In general, it is prudent to err on the side of release when the clinical picture is unclear since the morbidity of a missed compartment syndrome is far worse than the morbidity of a fascial release. A delay could have led to muscle necrosis, permanent debility, and/or transient or persistent nerve damage.3
Exertional rhabdomyolysis is likely underreported, with an estimated incidence of 26,000 cases per year.2 The first case of spinning-induced rhabdomyolysis was reported in 2004 in the United Kingdom.11 A healthy 34-year-old woman attended a spinning class for the first time and subsequently presented with leg pains and hematuria 2 days later. Her CPK was 409,000 U/L on presentation.11 Two cases of exertional rhabdomyolysis requiring hospitalization after spinning classes have occurred.8 However, none of these patients developed compartment syndrome requiring fasciotomy or acute kidney injury.
Footnotes
The authors report no potential conflicts of interest in the development and publication of this article.
References
- 1. Anderson KD. Missed diagnosis of acute exertional compartment syndrome, occurring after a short run. Am J Emerg Med. 2005;23:215-216 [DOI] [PubMed] [Google Scholar]
- 2. Bagley WH, Yang H, Shah KH. Rhabdomyolysis. Intern Emerg Med. 2007;2:210-218 [DOI] [PubMed] [Google Scholar]
- 3. Balogh B, Piza-Katzer H. Compartment syndrome. Frequently missed, with severe sequelae. Langenbecks Arch Für Chir. 1995;380:308-314 [DOI] [PubMed] [Google Scholar]
- 4. Bosch X, Poch E, Grau JM. Rhabdomyolysis and acute kidney injury. N Engl J Med. 2009;361:62-72 [DOI] [PubMed] [Google Scholar]
- 5. King TW, Lerman OZ, Carter JJ, Warren SM. Exertional compartment syndrome of the thigh: a rare diagnosis and literature review. J Emerg Med. 2010;39:e93-e99 [DOI] [PubMed] [Google Scholar]
- 6. Nau T, Menth-Chiari WA, Seitz H, Vécsei V. Acute compartment syndrome of the thigh associated with exercise. Am J Sports Med. 2000;28:120-122 [DOI] [PubMed] [Google Scholar]
- 7. Oh JY, Laidler M, Fiala SC, Hedberg K. Acute exertional rhabdomyolysis and triceps compartment syndrome during a high school football camp. Sports Health. 2012;4:57-62 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Parmar S, Chauhan B, DuBose J, Blake L. Rhabdomyolysis after spin class? J Fam Pract. 2012;61:584-586 [PubMed] [Google Scholar]
- 9. Smoot MK, Amendola A, Cramer E, et al. A cluster of exertional rhabdomyolysis affecting a Division I football team. Clin J Sport Med. 2013;23:365-372 [DOI] [PubMed] [Google Scholar]
- 10. Weibrecht K, Dayno M, Darling C, Bird SB. Liver aminotransferases are elevated with rhabdomyolysis in the absence of significant liver injury. J Med Toxicol. 2010;6:294-300 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Young IM, Thomson K. Spinning-induced rhabdomyolysis: a case report. Eur J Emerg Med. 2004;11:358-359 [DOI] [PubMed] [Google Scholar]