

Abstract
Angiolipoma is a common benign tumor with a characteristic vascular component that usually occurs in subcutaneous tissue. Although lipomas are frequently encountered at colonoscopy as submucosal tumors, angiolipomas are rarely found in the gastrointestinal tract including the large intestine. Here we report a 77-year old Japanese man who underwent transanal resection of a tumor that was diagnosed tentatively as a leiomyoma. Histologically, the tumor consisted of mature fat cells and blood vessels. Immunohistochemically, the tumor cells were negative for c-kit and HMB-45, which are consistently expressed in tumors such as gastrointestinal stromal tumor and angiomyolipoma. The tumor was therefore diagnosed as an angiolipoma. This is thought to be the first case report of a surgically resected angiolipoma of the rectum.
Keywords: Angiolipoma, Angiomyolipoma, Gastrointestinal stromal tumor
INTRODUCTION
Angiolipomas are subcutaneous tumors made up of mature fat and prominent blood vessels, and usually occur in young adults and older teenagers. They are rarely larger than 2 cm in diameter, frequently multiple, and characteristically tender or painful[1]. The most common locations are the forearm, trunk, and upper arm, and they rarely occur in the gastrointestinal tract. Grossly, angiolipomas are well circumscribed and yellow with varying amounts of red surface. A characteristic feature is fibrin thrombi within the vessels. The proportion of adipose and vascular tissue varies from predominantly lipomatous to predominantly angiomatous. Here we describe the first case of rectal angiolipoma diagnosed postoperatively.
CASE REPORT
A 77-year old Japanese man was admitted to our hospital with a 1-year history of anal bleeding. The patient lacked any findings suggestive of tuberous sclerosis. He had no cutaneous or retinal lesions, neurologic symptoms, or evidence of mental retardation. The family history and past medical history were unremarkable. All routine laboratory parameters, including carcinoembryonic antigen, were within normal limits. A double-contrast barium enema revealed a sessile lesion in the periproctic area measuring 20 mm × 15 mm (Figure 1). A subsequent colonofiberscopy disclosed a sessile-type submucosal tumor with internal hemorrhoids, and the tumor had no reddish depression or ulceration at its top (Figure 2). The other parts of the colon and rectum appeared normal. A biopsy specimen revealed proliferation of the muscle component with no atypical cells. A tentative diagnosis of leiomyoma was therefore made. Enhanced CT of the abdomen demonstrated a partially enhanced mass lesion with fat component which was not suspected of having infiltrated the proper muscle layer, on the right wall of the lower rectum (Figure 3). Trans-anal endoscopic ultrasonography revealed that the tumor was located in the submucosal layer. Because the tumor was considered to be benign, and difficult to resect by endoscopic surgery, we elected to perform trans-anal tumor resection with an ultrasonically activated device (Harmonic Scalpel®) to prevent bleeding from the internal hemorrhoids. Under general anesthesia, with the patient in the lithotomy position, we were able to approach the anal side of the tumor easily and resect it without massive oozing. Complete resection was performed with a sufficient surgical margin from the submucosal tumor. The total operation time was 42 min and bleeding was only slight. The postoperative course was uncomplicated, and the patient was discharged five days later. He was followed up for 12 mo at the outpatient clinic and no tumor recurrence was observed during that time. Macroscopic observation revealed that the sessile tumor, measuring 2 cm × 1.5 cm × 1 cm, was yellowish in color, located in the submucosal layer and covered with normal mucosa. A cross-section of the formalin-fixed tumor revealed massive growth without a capsule. The proper muscle layer was not infiltrated by the tumor. The tumor consisted of mature fat cells and blood vessels of various sizes. No mitoses or cytological atypia were found in the cells. Immunohistochemical staining for alpha-smooth muscle actin, S-100 protein, HMB-45 and c-kit was performed. Only the blood vessels were positive for alpha-smooth muscle actin, and the tumor cells were negative for HMB-45, c-kit and S-100 (Figure 4).
Figure 1.
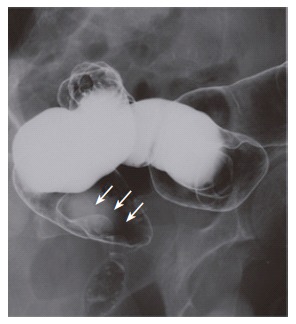
Double-contrast barium enema revealing a 20 mm × 15 mm sessile lesion in the periproctic area (arrows).
Figure 2.
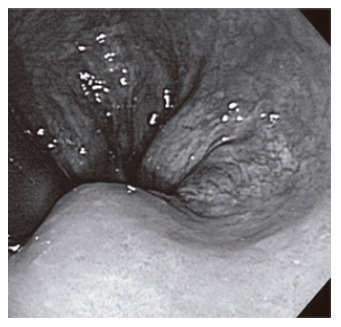
Colonoscopy disclosing a sessile lesion with a smooth surface.
Figure 3.

Enhanced CT of the lower abdomen demonstrating a fat-containing and slightly enhanced mass at a slice level corresponding to the right side of the lower rectum (arrow).
Figure 4.
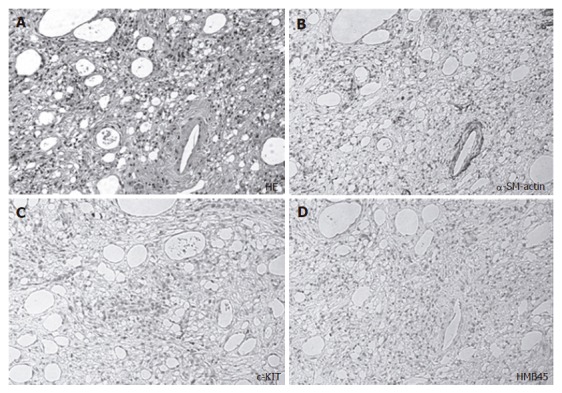
The tumor composed of a mixture of fat cells, proliferated blood vessels, spindle cells and immature mesenchymal cells (A), smooth muscle of a blood vessel demonstrating staining for alpha-smooth muscle actin but not for spindle cells (B), no tumor cells but only a few histiocytes displaying staining for c-kit (C), and no cells showing positive staining for HBM-45 (D).
DISCUSSION
Angiolipoma was first described in 1912 by Bowen[2]. In 1960, Howard and Helwig[3] demonstrated that the clinicopathologic features of angiolipomas differ from those of lipomas, thereby delineating angiolipoma as a new entity. Angiolipomas usually develop as encapsulated subcutaneous tumors, most commonly on the arms and trunk in young adults. Only 15 cases of angiolipoma occurring in the gastrointestinal tract were found in a MEDLINE search. These angiolipomas were located in the esophagus in one case[4], the stomach in 4 cases[5-8], the small intestine in 5 cases[9-13] and the colon in 5 cases[14-18]. The search revealed no reported cases of rectal angiolipoma. There are clinical differences between angiolipomas located in the gastrointestinal tract and those commonly occurring in subcutaneous tissue. The 15 reported gastrointestinal lesions were all solitary, and 4 showed bleeding from the tumor[5,8,9,13], all except one[7] occurring in elderly patients. In the bleeding cases, the tumor was over 2 cm in diameter and the bleeding point was located on the top of the tumor[14,16], which had a pumpkin-like shape[16]. In the present case, the tumor was less than 2 cm in diameter and its surface was covered with smooth and normal mucosa. It was thought that the tumor was too small to show a bleeding tendency. The differential diagnosis of angiolipoma includes angiomyolipoma[19], which is composed of smooth muscle, fatty tissue and blood vessels. Because a minor smooth muscle component was recognized in this case, the initial pathological diagnosis was angiomyolipoma. However, examination in detail showed that proliferation of the lamina muscularis mucosae might have caused physical irritation, especially during defecation, and that the smooth muscle component was not a dominant component of the tumor. Additionally, immunohistochemical staining for HMB-45 was effective for differential diagnosis between angiolipoma and angiomyolipoma. In this case, HMB45 staining was negative. However, there is a case report of angiomyolipoma that was immunohistochemically negative for HMB45[15]. In addition, pathologically, angiomyolipoma is common in the kidney and is often associated with dermatomyositis.
Angiomyolipoma is difficult to diagnose preoperatively and is usually diagnosed as lipoma.
Surgical excision is the treatment of choice. The recurrence rate is high in cases that are inadequately resected, but when the tumor can be removed completely, the prognosis is excellent. In this case, we selected transanal tumor resection because of the difficulty to obtain a good field for performing endoscopic resection[20] or transanal endoscopic microsurgery for this periproctic tumor with internal hemorrhoids that would bleed easily. Transanal tumor resection allowed us to obtain a good field and we were able to minimize bleeding from the internal hemorrhoids by removing the tumor with a Harmonic Scalpel® with a sufficient surgical margin.
Footnotes
S- Editor Liu Y L- Editor Wang XL E- Editor Bi L
References
- 1.Rogy MA, Mirza D, Berlakovich G, Winkelbauer F, Rauhs R. Submucous large-bowel lipomas--presentation and management. An 18-year study. Eur J Surg. 1991;157:51–55. [PubMed] [Google Scholar]
- 2.Bowen JT. Multiple subcutaneous hemangiomas, together with multiple lipomas, occurring in enormous numbers in anotherwise healthy, muscular subject. Am J Med Sci. 1912;144:189–192. [Google Scholar]
- 3.Howard WR, Helwig EB. Angiolipoma. Arch Dermatol. 1960;82:924–931. doi: 10.1001/archderm.1960.01580060078011. [DOI] [PubMed] [Google Scholar]
- 4.Kline ME, Patel BU, Agosti SJ. Noninfiltrating angiolipoma of the mediastinum. Radiology. 1990;175:737–738. doi: 10.1148/radiology.175.3.2343124. [DOI] [PubMed] [Google Scholar]
- 5.DeRidder PH, Levine AJ, Katta JJ, Catto JA. Angiolipoma of the stomach as a cause of chronic upper gastrointestinal bleeding. Surg Endosc. 1989;3:106–108. doi: 10.1007/BF00590911. [DOI] [PubMed] [Google Scholar]
- 6.Ferrozzi F, Tognini G, Marchesi G, Spaggiari E, Pavone P. Gastric tumors with fatty components. CT findings and differential diagnosis. Radiol Med. 2000;100:343–347. [PubMed] [Google Scholar]
- 7.Hunt J, Tindal D. Solitary gastric Peutz-Jeghers polyp and angiolipoma presenting as acute haemorrhage. Aust N Z J Surg. 1996;66:713–715. doi: 10.1111/j.1445-2197.1996.tb00724.x. [DOI] [PubMed] [Google Scholar]
- 8.McGregor DH, Kerley SW, McGregor MS. Case report: gastric angiolipoma with chronic hemorrhage and severe anemia. Am J Med Sci. 1993;305:229–235. doi: 10.1097/00000441-199304000-00006. [DOI] [PubMed] [Google Scholar]
- 9.Aouad K, Texier P, Bloch F, De Labriolle-Vaylet C, Bouillot JL. Benign angiolipoma of the Bauhin valve causing severe digestive tract bleeding. Gastroenterol Clin Biol. 2000;24:686–688. [PubMed] [Google Scholar]
- 10.Jung IS, Jang JY, Ryu CB, Hong SJ, Kim JO, Cho JY, Lee JS, Lee MS, Jin SY, Shim CS, et al. Angiolipoma of the duodenum diagnosed after endoscopic resection. Endoscopy. 2004;36:375. doi: 10.1055/s-2004-814213. [DOI] [PubMed] [Google Scholar]
- 11.Kaneko T, Karasawa Y, Inada H, Tamura Y, Yamamura N, Iijima Y, Nagata A, Oohata T, Shirota H, Nakamura T, et al. An adult case of intussusception due to inverted Meckel's diverticulum accompanied by angiolipoma. Nihon Shokakibyo Gakkai Zasshi. 1996;93:260–265. [PubMed] [Google Scholar]
- 12.Kwak HS, Kim CS, Lee JM. Small intestinal angiolipoma: MR imaging appearance. Abdom Imaging. 2003;28:515–517. doi: 10.1007/s00261-002-0058-7. [DOI] [PubMed] [Google Scholar]
- 13.Manner M, Scholz E, Wehrmann M, Stickel W. Invagination caused by angiolipoma of the small intestine--a rare cause of occult gastrointestinal hemorrhage. Chirurg. 2001;72:305–307. doi: 10.1007/s001040051310. [DOI] [PubMed] [Google Scholar]
- 14.Kato K, Matsuda M, Onodera K, Sakata H, Kobayashi T, Kasai S. Angiolipoma of the colon with right lower quadrant abdominal pain. Dig Surg. 1999;16:441–444. doi: 10.1159/000018765. [DOI] [PubMed] [Google Scholar]
- 15.Maesawa C, Tamura G, Sawada H, Kamioki S, Nakajima Y, Satodate R. Angiomyolipoma arising in the colon. Am J Gastroenterol. 1996;91:1852–1854. [PubMed] [Google Scholar]
- 16.Okuyama T, Yoshida M, Watanabe M, Kinoshita Y, Harada Y. Angiolipoma of the colon diagnosed after endoscopic resection. Gastrointest Endosc. 2002;55:748–750. doi: 10.1067/mge.2002.122958. [DOI] [PubMed] [Google Scholar]
- 17.Saroglia G, Coverlizza S, Roatta L, Leli R, Fontana D. Angiolipoma of the cecum. Minerva Chir. 1996;51:59–62. [PubMed] [Google Scholar]
- 18.Vandamme J. Angiolipoma of the colon. Acta Gastroenterol Belg. 1964;27:750–757. [PubMed] [Google Scholar]
- 19.Chen JS, Kuo LJ, Lin PY, Changchien CR. Angiomyolipoma of the colon: report of a case and review of the literature. Dis Colon Rectum. 2003;46:547–549. doi: 10.1007/s10350-004-6598-x. [DOI] [PubMed] [Google Scholar]
- 20.Pfeil SA, Weaver MG, Abdul-Karim FW, Yang P. Colonic lipomas: outcome of endoscopic removal. Gastrointest Endosc. 1990;36:435–438. doi: 10.1016/s0016-5107(90)71110-8. [DOI] [PubMed] [Google Scholar]