

Abstract
AIM: To investigate the gastrointestinal bleeding (GIB) in people from lowland to high altitude and in workers on Mountain Tanggula and its causes as well as treatment and prophylaxis.
METHODS: From 2001 to October 2003, we studied GIB in 13 502 workers constructing the railroad on Mountain Tanggula which is 4905 m above the sea level. The incidence of GIB in workers at different altitudes was recorded. Endoscopy was performed when the workers evacuated to Golmud (2808 m) and Xining (2261 m). The available data on altitude GIB were analyzed.
RESULTS: The overall incidence of GIB was 0.49% in 13 502 workers. The incidence increased with increasing altitude. The onset of symptoms in most patients was within three weeks after arrival at high altitude. Bleeding manifested as hematemesis, melaena or hematochezia, and might be occult. Endoscopic examination showed that the causes of altitude GIB included hemorrhage gastritis, gastric ulcer, duodenal ulcer, and gastric erosion. Experimental studies suggested that acute gastric mucosal lesion (AGML) could be induced by hypoxic and cold stress, which might be the pathogenesis of altitude GIB. Those who consumed large amount of alcohol, aspirin or dexamethasone were at a higher risk of developing GIB. Persons who previously suffered from peptic ulcer or high-altitude polycythemia were also at risk of developing GIB. Early diagnosis, evacuation, and treatment led to early recovery.
CONCLUSION: GIB is a potentially life threatening disease, if it is not treated promptly and effectively. Early diagnosis, treatment and evacuation lead to an early recovery. Death due to altitude GIB can be avoided if early symptoms and signs are recognized.
Keywords: High altitude, Gastrointestinal bleeding, Hypoxic stress, Acute gastric mucosal lesion, Risk factors
INTRODUCTION
Although cardiac, respiratory and neurological symptoms are more common among mountaineers and persons from lowland going to the high altitude, little work has been done on the effect of hypoxia on digestive system in either patients with altitude illness or in healthy individuals at high altitude. In fact, symptoms of the digestive system such as anorexia, epigastric discomfort, epigastralgia, heart burn, dyspepsia, nausea, vomiting, diarrhea, haematemesis, piles and peptic ulcers are frequently found in mountaineers and altitude sojourners[1,2]. Moreover, epidemiological and clinical studies suggest that gastrointestinal bleeding (GIB) is not uncommon at high altitude, and is often life-threatening[3,4]. There are two diagnostic criteria for acute mountain sickness (AMS), one is the ESQIII[5] and the other is the Lake Louise consensus scoring system[6]. Gastrointestinal symptoms include nausea/vomiting, loss of appetite, stomach/abdominal pain, constipation, however, the GIB is not included in the diagnostic criteria. Furthermore, data on GIB are available from Japanese, Chinese, and Peruvians, but rarely reported in western people[7].
Altitude problems are of great importance for the railroad construction workers at high altitude. The construction of railroad on Mountain Tanggula offered a unique opportunity for investigation and study of AMS, high altitude pulmonary edema (HAPE), and high altitude cerebral edema (HACE), as well as high altitude GIB. This paper describes the incidence, clinical features, and risk factors for GIB in the railroad construction workers on Mountain Tanggula.
MATERIALS AND METHODS
Areas and subjects
Between June 29, 2001 and October 31, 2003, altitude gastrointestinal problems including altitude GIB were studied at two hospitals near the construction site. One hospital is located on the Fenghoushan at an altitude of 4779 m and the other hospital is situated in the Kekexili area at an altitude of 4505 m. These two hospitals received patients from the construction sites, working at altitudes between 3486 m and 4905 m. A total of 8014 workers worked at Fenghoushan and 5488 in Kekexili over the past three years. The weather conditions in the two surveying regions and the evacuated areas in Golmud and Xining are summarized in Table 1.
Table 1.
Weather conditions in the two surveying regions and the two evacuated areas-Golmud and Xining
| Area | Fenghoushan | Kekexili | Golmud | Xining |
| Altitude (m) | 4905 | 4905 | 2808 | 2261 |
| PB (mmHg) | 417 | 440 | 538 | 585 |
| Average annual temperature (°C) | -7.0 | -2.6 | 3.6 | 6.7 |
| Annual precipitation (mm) | 317 | 291 | 42 | 371 |
| Annual sunshine time (h) | 2712 | 2764 | 3101 | 2793 |
| Relative humility (%) | 57 | 58 | 34 | 57 |
The weather and climatologic data were provided by the Tanggula Meteorological Observatory Station and the Qinghai Weather Bureau. Workers were not only exposed to a hypoxic environment, but also to severe cold. The temperature in winter ranged between -27°C and -36°C, with an annual average temperature of -3°C to -7°C.
A questionnaire was delivered to the persons to be investigated, including age, gender, ethnicity, occupation, place of birth, length of time at low altitude, length of time after ascending to high altitude, history of smoking and consumption of alcoholic beverages, current and past medical history, and family history.
All subjects underwent a careful medical evaluation before and after ascending to high altitude. Physical examination, routine blood tests, chest roentgenograms, electrocardiograms, etc were performed. The protocol was approved by the Qinghai High Altitude Medical Research Institute Committee on Human Research. Informed consent was obtained verbally for each subject.
Diagnosis
The diagnosis of AMS was made using the Lake Louise scoring system (LLSS) in which two or more of symptoms monitored were defined as AMS[6]. The clinical diagnosis of GIB was based on the following criteria: (1) occurrence in unacclimatized individuals who were rapidly exposed to altitudes exceeding 3000 m; (2) onset of typical symptoms including epigastric discomfort, epigastric pain, haematemesis, melaena, or hematochezia; (3) significant decrease in hemoglobin concentration (Hb) or hematocrit value (Hct); (4) endoscopic diagnosis of GIB after descending to the Golmud (2808 m) or Xining (2261 m); (5) disappearance of symptoms and signs after treatment with blood transfusion and oxygen. Outcome was assessed according to the clinical and laboratory results.
Statistical analysis
Statistical analysis was made by the IBM 3990 system. The incidence (cumulative case rate over a defined period in a defined population) of GIB in these populations was calculated. The frequency of risk factors for GIB was examined, using two by two tables, odds ratios, and chi square test. Comparison of mean numerical values was made by t test. P < 0.05 was considered statistically significant.
RESULTS
Overall incidence
We selected two typical areas where the local hospitals are located to investigate the altitude illness. From 2001 to 2003, GIB was found in 66 cases of 13 502 workers on Mountain Tanggula during the period with an incidence of 0.49%.
Predisposing factors
The incidence of GIB was also found to be dependent upon many variables, including altitude, length of stay at high altitude, age, sex, labouring conditions, and ethnicity.
Altitude: The incidence of GIB at various altitudes is shown in Figure 1. Occurrence of GIB was rarely found below 3500 m. The highest frequency of GIB was observed between 4500 m and 5000 m, its incidence increased gradually with altitudes being 0.2% at 3500 m and 1.1% at 4905 m (P < 0.01).
Figure 1.
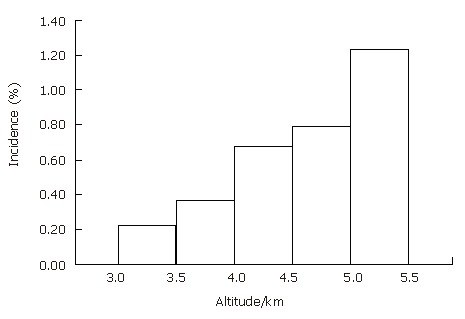
Frequency distribution of altitudes in patients with gastrointestinal bleeding diagnosed at two hospitals on Mountain Tanggula. The incidence of GIB increases with increasing altitude.
Onset time of symptoms: Symptoms suggestive of GIB occurred in 17 out of 66 cases (25.8%) within 5-10 d after arrival at high altitude, in 24 cases (36.3%) within 11-15 d, 14 cases (21.2%) within 16-20 d, the remaining 11 cases(16.7%) within 21-122 d (16.7%) (Figure 2). The onset time of most symptoms was within three weeks after arrival at high altitude.
Figure 2.

Time lag between ascent and onset of illness.
Age and gender: Many of the patients were young or middle-age adults, and the oldest was 46 years of age. The mean age of all cases was 34 ± 7.8 years.
GIB occurred frequently in men. Since the total number of females was small (21 persons), and could be neglected.
Occupation: The incidence of GIB in workers and carders was 0.51% and 0.46%, respectively. There was no significant difference between the two groups (P > 0.05).
Ethnicity: Interestingly, all the GIB patients were Han Chinese lowlanders. Over one-third of the workers were native highlanders (most of them were Tibetans who permanently lived at altitudes from 2500 m to 3200 m) and no GIB was found in them.
Endoscopic findings
All patients with altitude GIB were evacuated to the hospitals in Golmud or Xining. Among them, 28 had an endoscopic examination either at admission or within 24 h after admission and others were not able or refused to undergo an endoscopic examination. Endoscopic examination showed gastric ulcer in 11 cases, duodenal ulcer in 4, combined ulcers in 4, hemorrhage erosion in 5, bleeding gastritis in 4 and chronic atrophic gastritis in 1, respectively.
Risk factors
GIB was obviously related to drinking alcohol and use of aspirin and/or dexamethasone in 3 patients. Case one was a 37-year old railroad worker from lowland to a construction site at 4505 m. During the ascent, he was given 8 mg dexamethasone followed by 4 mg every eight hours for AMS prophylaxis. In the morning after arrival at 4505 m, he complained of severe headache. He was given 0.5 g of aspirin and dexamethasone, which did not relieve his headache. He drank approximately 300 mL of liquor (50% alcohol). After eight hours he suddenly became incapacitated with symptoms of upset stomach, abdominal pain, and severe fatigue. At about 6.0 AM on the third day, he had melaena and tarry black stool, thus aspirin and dexamethasone were immediately stopped. Within a few hours his condition became progressively worsened, and he was promptly evacuated to the Golmud Hospital (2808 m). At admission, his BP was 90/50 mmHg and Hb level was below 65 g/L. Gastro-fiberscopic examination was performed within six hours after admission and revealed diffuse gastric bleeding and erosion, and linear gastric ulcer combined with duodenal ulcer. Supplementary oxygen was given and an intravenous drip was put up. After 600 mL whole blood transfusion over about five hours, and administration of H2 blocker (ranitidine), his BP gradually increased (110/80 mmHg), and malaena was stopped. He slowly improved over two weeks, his Hb increased to 105 g/L. He was discharged 21 d after admission and returned to his lowland home.
In addition to this case, we encountered 2 similar cases at the Kekexili construction site. Case two was a healthy young man who took aspirin and dexamethasone to prevent AMS and drank alcohol in the evening, he had brisk melaena in the next morning. Case three was a middle age worker, with a previous history of gastric peptic ulcer. He took aspirin for headache, after drinking 100 mL of hard liquor, he developed acute melaena.
Polycythemia (Hb > 210 g/L) was found in 5 patients with GIB having lived at altitude above 4000 m for more than 45 d.
Moreover six patients with GIB had a previous history of potential peptic ulcer and 5 had chronic gastritis.
Outcomes
Once the diagnosis was confirmed, the patients were either evacuated to the Golmud Hospital (2808 m), or treated as outpatients or sent to Xining (2261 m). Their conditions gradually improved after effective treatments.
DISCUSSION
Nomenclature and relation between AMS and altitude GIB
High-altitude GIB is a distinct clinical entity. However, the different terms of this syndrome have been used by different authors. The term “hypoxic gastric bleeding” is used loosely in some Peruvian scientists[8], “altitude digestive hemorrhage” is also used for this illness[9]. Since hemorrhage could occur in buccal mucosa, digestive mucosa, finger nails, as well as in gastrointestinal tract, urinary tract, retina and gums[10,11], it is named as “high altitude hemorrhage syndrome”. GIB is one of the clinical manifestations of this syndrome[11]. However, GIB is almost an independent digestive mucosal lesion, causing gastrointestinal bleeding at high altitude. We hold that the term “high altitude gastrointestinal bleeding” (altitude GIB) is more suitable for this condition.
We also noted that approximately 58% of GIB patients are accompanied with AMS, and about 42% have altitude GIB alone. However, GIB has not been found to be associated with HAPE or HACE. Thus whether altitude GIB is a gastrointestinal type of AMS should be further studied.
Incidence of altitude GIB
The incidence of altitude GIB among workers constructing Qinghai-Tibetan highway on Mountain Tanggula from 1978 to 1984 was 1.1%[4]. The incidence of altitude GIB in workers constructing the Qinghai-Tibetan railroad at the same mountainous areas was 0.49% in 2001-2003, which is much lower than the reported incidence in mountaineers on Everest. During 1988 the China-Japan-Nepal Friendship Expedition to Mountain Qomolungma (Everest), a total of 52 Japanese mountaineers climbed from Tibetan (north) side (5154 m) to the summit (7790 m), five on the north side suffered from upper alimentary bleeding with an incidence of 9.6%[12], suggesting that the incidence of GIB increases with the increase of altitude.
Liu[13] reported that the occurrence of GIB in soldiers stationed between 3700 m and 5380 m for one year is 0.8% of the total patients and 1.5% of AMS cases at a Chinese Army Hospital located at the foot of Mountain Karakoram (3550 m) during the same period. However, endoscopy examination showed that the incidence of acute gastric mucosal lesion (AGML) in mountaineers is as high as 16%-49%[14-16], suggesting that some subclinical GIB exists.
Clinical features of altitude GIB
Of the 66 cases, 17 had altitude GIB within 10 d after arrival at above 3500 m. Most patients (55) had altitude GIB within 20 d, and 11 had altitude GIB after 21 d. These observations were incomparable with the onset of HAPE or HACE. In general, the mean time of HAPE or HACE occurrence after arrival at above 3500 m was three days with a range of 1-5 d.
The victims of GIB include both mountaineers and native highlanders[8,17]. Macedo[8] reported that two adult male native Quechua Indians presented a sudden and severe gastric bleeding of unknown etiology in the Andes. However, in our GIB patients, there were no Tibetan natives. It is possible that these individuals have greater genetic resistance to hypoxia at high altitude.
At high altitude, GIB may be manifested as haematemesis (vomiting of blood, either bright red or brown in color), melaena (tarry black, sticky stool) or hematochezia (fresh red blood per rectum, ruling out the diagnosis of piles). However, hemorrhage was manifested as melaena in almost all 64 patients except for two with haematemesis. Bleeding, however, might be occult, with normal appearance of stools. Occult blood in stools was detected in 10 mountaineers by Naito et al[18] using “OC-Hemodia Kit” which can detect only human hemoglobin without cross-reaction in any other animals during their Iwate Karakoram expedition in 1989, a total of 8 persons presented a positive reaction, suggesting that silent bleeding from gastrointestinal mucosa commonly exists in mountaineers.
GIB gives rise to symptoms and signs depending upon the rate and extent of bleeding. In our experiences, acute moderate bleeding (blood loss greater than 500 to 1000 mL) results in drowsiness, dizziness, oliguria, sweating and pallor. BP changes occur first in the form of orthostatic hypotension. Pulse rate seems to be a far less accurate parameter, particularly at high altitude, as tachycardia is common amongst such mountaineers. Acute massive bleeding is characterized by loss of greater than 1500 mL or 25% of the circulating blood volume within a period of minutes to hours, decreased systolic and diastolic BP, increased pulse rate, decreased hemoglobin concentration or Hct values. It is a critical indicator for the desperate situation. Therefore any patient experiencing malaena with or without hematemesis or associated symptoms or hypotension, should be evacuated promptly and hospitalized immediately for further evaluation and treatment[4].
Endoscopic findings and causes of altitude GIB
Endoscopy is highly advisable. Sugie et al[19] found gastro-duodenal mucosa lesions in 13 out of 22 mountaineers at Mountain Xixapangma (5020 m). The results of arterial blood gas analysis reported by Sugie et al[20] are as follows: PaO2 = 43 mmHg, PaCO2 = 23.5 mmHg, pH = 7.51, BE = 1.0. Zhao and Li[15,16] reported that the incidence of gastro-duodenal mucosal lesions is 49% in 51 young healthy male subjects at the altitude between 3658 m and 4200 m. Occasionally, upper digestive hemorrhage may occur in gastric cancer patients at altitude[21,22].
Saito[12] reported a male mountaineer on Mt. Everest expedition who developed massive GIB and serious anemia at the altitude of 7028 m. Endoscopy after his arrival at sea level, showed no abnormality[23]. Zhou[24] reported a case of a healthy lowland Han subject who developed GIB during a sojourn at Lhasa (3658 m) and died of recurrent massive GIB. Postmortem revealed diffuse superficial erosion in the stomach but no peptic ulcers.
Mechanism of altitude GIB
The mechanism of altitude GIB remains unclear. Pathological studies in patients died of altitude GIB revealed significant dilatation of arterioles and venules, formation of extensive blood capillaries in gastric mucosa[25] and hemorrhage into the gastric mucosa[26]. Different kinds of stress can cause AGML. It was reported that cold or hypoxic stress can induce AGML in rats[27,28]. However, on high mountains, cold stress usually accompanies the effects of hypoxic stress in mountaineers, suggesting that hypoxemia is probably the main factor for AGML in mountaineers who are healthy at sea level[19]. Kamiyama et al[29] have attributed the potential difference (PD) to the indicator of gastric integrity or gastric mucosa defensive mechanism that may play an important role in the pathogenesis of hypoxia-induced AGML. The PD is closely related to the transport of electrolytes by gastric mucosa cells depending on aerobic metabolism. Hypoxemia may cause changes in tissue levels of oxygen resulting in decrease of PD. Strenuous exertion and hard work increase hypoxia stress and induce injury of gastric mucosa capillaries[14,17]. Naito et al[30] noted that peroxidation of phosohatidylcholine in gastric mucosa is another possible mechanism underlying AGML at high altitude. It was reported that ulcer index (UI) and phosphatidylcholine hydroperoxide (PCOOH) are higher in hypoxia group than in control group, though thiobarbituric acid (TBA) substance does not differ between the two groups, suggesting that lipid peroxidation in gastric mucosa may play a role in the pathogenesis of hypoxia-induced AGML. Acute diffuse lesions induced by stresses are pathologically and clinically distinct from gastro-duodenal mucosa lesions and present as an upper alimentary bleeding.
Fisk factors for altitude GIB
Alcohol: It is historically believed that alcohol could relieve and protect against AMS[4]. More recently, Houston[31] has recommended less alcohol use on mountains. It appears that alcohol may also be a risk factor for GIB at altitude. Ravenhill[32] has observed that alcohol increases the severity of symptoms of AMS. Those who drink a little alcohol under a simulated hypoxic condition (7620 m), may impair their mental and physical function[33]. Steele[34] has described three Sherpas who had severe epigastric pain, nausea and vomiting after heavy drinking on Mountain Everest. Zhou[24] reported three young men in Lhasa who developed massive gastric hemorrhage due to acute hemorrhagic gastritis after a hard drinking. High altitude native populations, such as Quechua Indians, like to drink inferior rough alcohol, which may be the aetiology of the increased prevalence of gastric ulceration[26]. From 1978 to 1984 when the Qinghai-Tibetan Highway was under construction, the incidence of GIB was higher (1.93%) in workers who drank more of it than in those (0.95%) who drank it less[4], suggesting that drinking alcohol increases the risk of developing GIB at altitude and alcohol should be avoided.
Aspirin or other NSAID agents: Aspirin has been shown to be effective in treating headache due to AMS[35]. Aspirin alone is not very effective in preventing headache due to AMS, whereas aspirin in combination with dexamethasone can achieve rather good results[36]. There is strong but not conclusive evidence that major bleeding episodes could result from acute, diffuse hemorrhagic lesions in the upper GI tract after ingestion of aspirin. Thus, relief of headache due to AMS is a difficult matter because aspirin and other non-steroidal anti-inflammatory drugs (NSAID) lead to GIB[7,37]. It was reported that drugs such as paracetamol (acetaminophen) or ibuprofen, have a strong anti-inflammatory action on headache or other pains and do not cause gastrointestinal bleeding[38].
Dexamethasone: Dexamethasone has been used in the prevention and treatment of AMS[39,40] because administration of it for a short time does not result in any problems at high altitude[31]. However, dexamethasone is one of the drugs that are strongly suspected of being ulcerogenic, especially in patients with a prior history of peptic ulcer disease, and may increase the risk of GIB at altitude. Concomitant use of dexamethasone, aspirin and alcohol has an additive or synergistic effect on the upper GI tract mucosa, and could lead to rapid and serious GIB as in our cases.
High altitude polycythemia: Polycythemia is a common feature seen in altitude residents and patients with hypoxemia[15,16,24]. Digestive symptoms such as epigastric pain, dyspepsia, anorexia, vomiting, and diarrhea can be frequently eliminated in 89%-100% of patients with high altitude polycythemia (HAPC)[24]. GIB is a common complication of HAPC. In our series five patients with GIB had HAPC. Zhou[24] reported polycythemia in 21 young male Chinese soldiers (mean age 26.6 years) stationed in Lhasa (3658 m) who had no previous history of peptic ulcer. GIB occurred following development of HAPC. They found that exposure to cold, strenuous exertion, and drinking alcohol are the main predisposing causes.
Zhao and Li[15,16] have reported their endoscopic examinations in 98 patients with HAPC (Hb > 210 g/L) in Lhasa, showing superficial gastritis in 29, gastric ulcer in 26, duodenal ulcer in 12, complex ulcers in 5, and atrophic gastritis in 3. Chu and Sun[41] examined 5 patients with HAPC (mean Hb = 225 g/L) in Madou (4300 m), diffuse bleeding and erosion as well as ulcerous necrosis were observed in their stomach, and electromicroscopic examination showed the ultrastructural characteristics of their gastric mucosal biopsies, such as irregularly arranged thick microvilli, microfilament enlargement of secretory canaliculus, and high density of enlarged mitochondria in parietal cells, increased zymogen granules and rough endoplasmic reticulum in principal cells, proliferation of vascular endothelial cells, microvilli-like appearance of their surface and basement membrance thickening. Such gastric mucosal lesions may be associated with gastric mucosal ischemia caused by microvascular thrombosis due to excessive polycythemia.
Peptic ulcerations at high altitude: Clinical observations on the Himalayas and Andes suggest that peptic ulcer occurs more frequently at high altitude than at sea level[21,24,42]. At high altitude, the ulceration rate is higher in gastric ulcer than in duodenal ulcer[43,44]. Berrio et al[42] reported that 100 cases of GIB have been diagnosed by endoscopic examinations in General Hospital at La Oroya (3800 m), gastric ulcer accounting for 33%, duodenal ulcer accounting for 23%, gastric erosion accounting for 23%, neoplasias accounting for 2%, respectively. The prevalence of gastric ulcer increases with increasing altitude, while the prevalence of duodenal ulcer does not[42]. Upper digestive hemorrhage is a common complication of peptic ulceration at high altitude[42,45], the hemorrhagic rate is 20%-66%[9,45].
It is well known that the incidence of gastric ulcers and bleeding is increasing in high altitude residents chronically exposed to a hypoxic environment[42,45-47]. In addition, hypoxic and cold stress-induced gastric mucosal lesion may explain in part, the high incidence of gastric ulcers in altitude populations.
In the present 66 cases of GIB, 4 had a previous history of peptic ulcer. Among them, GIB occurred rapidly in 1 patient after using aspirin, suggesting that persons with known peptic ulceration should not go to high altitude mountains unless their symptoms have been well controlled before they go to high altitude mountains as complications in the field can be fatal[37].
Course and prognosis of altitude GIB
Altitude GIB can be life threatening and acute massive bleeding due to secondary effects of shock-increasing anoxia, cellular dysfunction and acidosis at high mountains may lead to death[4]. We have reported that the mortality of altitude GIB is as high as 6.8% in Qinghai-Tibetan Highway construction workers on Mountain Tanggula[4].
The emergency measures taken for acute altitude GID include early evacuation or just descent with oxygen inhalation and saline-infusion or blood transfusion. Drugs, such as H2 blockers or proton pump inhibitors have been shown to be more effective in ameliorating GIB[4]. Mountaineers and highlanders should know well about the symptomatic self care (SSC) for altitude GIB[48], that is when symptoms such as epigastric pain or dyspepsia are present, a H2-receptor antagonist is effective for ulcers and GIB and the current therapy for altitude GIB.
In conclusion, early diagnosis, treatment and evacuation lead to an early recovery. Death due to altitude GIB can be avoided if early symptoms and signs are recognized.
Footnotes
Supported by the grant LS-CNNSF-30393130, and 973 Program 2006 CB 504100, CB708514, China
S- Editor Wang GP L- Editor Wang XL E- Editor Ma WH
References
- 1.Bhattacharjya B, editor . Mountain Sickness. Toronto: Bristol John Wright & Sons LTD; 1964. [Google Scholar]
- 2.Hu HC, Wu TY, Li TL, editors . High Altitude Disease. (In Chinese) Xining: Qinghai Publishing House; 1997. pp. 65–68. [Google Scholar]
- 3.Berrios J. Consideraciones sobre la pathologia digestive en los habitentes de las grandes alturas del Peru. (In Spanish) Rev Gastroenterol Peru. 1982;2:21–28. [Google Scholar]
- 4.Wu TY. Take note of altitude gastrointestinal bleeding. Newsletter Int Soc Mountain Med. 2001;10:9–11. [Google Scholar]
- 5.Sampson JB, Cymerman A, Burse RL, Maher JT, Rock PB. Procedures for the measurement of acute mountain sickness. Aviat Space Environ Med. 1983;54:1063–1073. [PubMed] [Google Scholar]
- 6.Roach RC, Bärtsch P, Hackett PH, Oelz O. The Lake Louse acute mountain sicknedd scoring system. In: Sutton JR, Houston CS, Coates G, editors. Hypoxia and Molecular Biology. Burlington, VT: Queen City Press; 1995. pp. 272–274. [Google Scholar]
- 7.Editorial. October case discussion. ISMM Newsletter. 1999;9:13–15. [Google Scholar]
- 8.Macedo Dianderas J. Hemorragias gastricas por hipoxia de altura. (In Spanish) Arch Inst Biol Andina Lima. 1968;2:183–187. [Google Scholar]
- 9.Monge ES, Diaz JF. Aparato gastrointestinal. En: C.C. Monge and F. Leon-Velarde, editors. El RETO Fisiologico de vivir en los ANDES. (In Spanish) Lima: Universidad Peruana Cayatano Heredia; 2003. pp. 227–229. [Google Scholar]
- 10.Heath D. The morbid anatomy of high altitude. Postgrad Med J. 1979;55:502–511. doi: 10.1136/pgmj.55.645.502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Li SP. High-altitude hemorrhage syndrome. J Wilderness Med. 1993;4:115–117. [Google Scholar]
- 12.Saito A. The medical reports of the China-Japan-Nepal Friendship Expedition to Mt. Qomolungma/Sagamatha (Everest) Jap J Mount Med. 1989;9:83–87. [Google Scholar]
- 13.Liu MF. Upper alimentary bleeding at high altitude. In: Lu YD, Li KX, Yin ZY, editors. High Altitude Medicine and Physiology. (In Chinese) Tianjing: Tianjing Science & Technology Press; 1995. p. 586. [Google Scholar]
- 14.Nakashima M, Saito A, Endo K, Matsubayashi K, Jin-Nouchi Y, Seto T, Demizu A, Hirata K. Sugie T, Kan N, Tobe T, Nayashi K, Adachi M, Kubo S. The report of Kyoto University Medical Research Expedition to Xixabangma (8027 m) 1999 (KUMREX' 90) Jap J Mount Med. 1990;10:135–144. [Google Scholar]
- 15.Zhao GB, Li R. The gastrointestinal mucosal lesions in patients with high altitude polycythemia. Zhonghua Yixue Zazhi. 1991;71:611–612. [Google Scholar]
- 16.Zhao GB, Li L. Impairment of the digestive system in high altitude erythrocythemia. Zhonghua NeiKe ZaZhi. 1991;30:492–494. [PubMed] [Google Scholar]
- 17.Macedo Dianderas J, Hemorragia gastricas en la altura (4540 m. Sebre el nivel del mar). (In Spanish) Arch Inst Biol Andina Lima. 1965;1:53–56. [Google Scholar]
- 18.Naito H, Matuno A, Sakai I, Kamiyama Y, Doi T, Kobari M, Rahman M, Takita A, Matsuda T. Gastrointestinal symptoms in high mountain climbing-Medical report in Iwate Karakoram Friendship Expedition on 1989. In: G. Ueda, JT Reeves, M Sekigushi., editors. High Altitude Medicine. Matsumoto: Shinshu University Press; 1992. pp. 286–299. [Google Scholar]
- 19.Sugie T, Adachi M, Jin-Nouchi Y, Matsubayashi K, Nakashima M, Saito A. Gastroduodenal mucosa lesion at high altitude. Jap J Mount Med. 1991;11:55–58. [Google Scholar]
- 20.Sugie T, Kan N, Saito A, Tobe T, Adachi M, Jin-Nouchi Y, Matsubayashi K, Nakashima M. Acute gastric mucosal lesion at the high altitude. In: Sutton JR, Coates G, Houston C, editors. Hypoxia and Mountain Medicine. Burlington: Queen City Printers Inc; 1992. p. 320. [Google Scholar]
- 21.Berrios J, Zapata C, Nago A, Bussaleu A, Farfan G. Estudio comparativo de la patologia digestiva de las grandes Alturas y del nivel del mar en el Peru. (In Spanish). En: III Jornades Cientificas. En bomenaje al centenario del nacimiento del professor doctor Carlos Monge Medrano. Enero 21-26 de 1985. Lima: Universidad Peruana Cayatano Heredia; 1985. p. 197. [Google Scholar]
- 22.Villanueva Palacios J, López de Guimaraes D, Avila Polo F. Upper digestive tract hemorrhage in the Peruvian Andes: report of 115 cases observed in Huaraz. Rev Gastroenterol Peru. 1976;16:99–104. [PubMed] [Google Scholar]
- 23.Masuyama M. A discussion on the October case discussion. ISMM Newsletter. 1999;9:13–15. [Google Scholar]
- 24.Cao ZW. editor. High Altitude Polycythemia. Beijing: Military Medical Science Press; 1996. pp. 96–97. [Google Scholar]
- 25.Zevallos G, Meiller M. Algunos aspectos histopathologicos de la ulcers gastroduodenal en la altura. (In Spanish) Rev Asoc Med Prov Yauli (Peru) 1959;4:66–73. [Google Scholar]
- 26.Heath D, Williams DR, editors . High Altitude Medicine and Pathology. Oxford: Oxford University Press; 1995. pp. 258–259. [Google Scholar]
- 27.Kamiyama Y, Sakai I, Naito H, Kobari M, Matsuno S, Tsuchiya T, Oketani K. Pathogenesis and prevention of experimental acute gastric ulcers by cold restraint stress. In: Ueda G, Kusama GS, Voelkel NF, editors. High Altitude Medical Science. Matsumoto: Shinshu University Press; 1988. pp. 454–457. [Google Scholar]
- 28.Aichi M. Experimental studies on development of gastric mucosal damage following acute hypoxemia in rats (author's transl) Nihon Shokakibyo Gakkai Zasshi. 1980;77:1223–1233. [PubMed] [Google Scholar]
- 29.Kamiyama Y, Matsuno S, Sakai I, and Naito H. Pathogenesis of experimental acute mucosal lesion induced by hypoxia in rats. In: Ueda G, Reeves JT, Sekiguch IM, editors. editors. High Altitude Medicine. Matsumoto: Shinshu University Press; 1992. pp. 280–285. [Google Scholar]
- 30.Naito H, Masuko T, Kamiyama Y, Sakai I, Matsuno S. A possible role of lipid peroxidation in the pathogenesis of acute gastric mucosal lesion induced by hypoxia. Abstracts of the Third World Congress on Mountain Medicine. Matsumoto: Shinshu University Press; 1998. p. 111. [Google Scholar]
- 31.Houston CS. editor. Go Higher, Oxygen, Man, and Mountain. 4th edition. Shrewsbury: Swan Hill Press; 1998. p. 157, 164. [Google Scholar]
- 32.Ravenhill TH. Some experience of mountain sickness in the Andes. J Tropical Med & Hygiene. 1913;16:313–320. [Google Scholar]
- 33.Nettles JL, Olson RN. Effects of alcohol on hypoxia. JAMA. 1965;194:1193–1194. [PubMed] [Google Scholar]
- 34.Steele P. Medicine on Mount Everest 1971. Lancet. 1971;2:32–39. doi: 10.1016/s0140-6736(71)90019-5. [DOI] [PubMed] [Google Scholar]
- 35.Burtscher M, Likar R, Nachbauer W, Philadelphy M. Aspirin for prophylaxis against headache at high altitudes: randomised, double blind, placebo controlled trial. BMJ. 1998;316:1057–1058. doi: 10.1136/bmj.316.7137.1057. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Burtscher MB, Philadelphy M, Likar R, and Nachbauer W. Aspirin versus diamox plus aspirin for headache during physical activity at high altitude (Abst.) In: Roach RC, Wagner PD, Hackett PH, editors. Hypoxia: Into the Next Millennium. New York: Plenum/Kluwer; 1999. p. 133. [Google Scholar]
- 37.Ward MP, Milledge JS, West JB, editors . High Altitude Medicine and Physiology. New York: Oxford University Press Inc; 2000. pp. 326–327. [Google Scholar]
- 38.Broome JR, Stoneham MD, Beeley JM, Milledge JS, Hughes AS. High altitude headache: treatment with ibuprofen. Aviat Space Environ Med. 1994;65:19–20. [PubMed] [Google Scholar]
- 39.Hackett PH, Roach RC, Wood RA, Foutch RG, Meehan RT, Rennie D, Mills WJ. Dexamethasone for prevention and treatment of acute mountain sickness. Aviat Space Environ Med. 1988;59:950–954. [PubMed] [Google Scholar]
- 40.Rabold M. Dexamethasone for prophylaxis and treatment of acute mountain sickness. J Wilderness Med. 1992;2:54–60. [Google Scholar]
- 41.Chu XQ, Sun HF. Ultrastructural characteristics of gastric mucosa inpatients with high altitude polycythemia. Abstracts of the Third World Congress on Mountain Medicine and High Altitude Physiology. Matsumoto: Shinshu Universith Press; 1998. p. 164. [Google Scholar]
- 42.Berríos J, Sedano O, Calle E, Montero F, Manrique J, Hinostroza E. [Upper digestive hemorrhage in the inhabitants of high altitudes in Peru] Rev Gastroenterol Peru. 1996;16:13–18. [PubMed] [Google Scholar]
- 43.Garrido-Klinge G, Pena L. Ulcera peptica en la altura. (In Spanish) Diagnostico (Peru) 1982;10:70–72. [Google Scholar]
- 44.Garrido-Klinge G, Pena L. The gastro-duodenal ulcer in high altitudes. Gastroenterology. 1959;37:390–400. [Google Scholar]
- 45.Garrido-Klinge G, Pena L. La ulcera gastroduodenal en las grandes Alturas (Andes Peruanos). (In Spanish) An Fac Med (Lima) 1960;43:419–436. [PubMed] [Google Scholar]
- 46.Maccagno FV. Ulcera gastro-duodenal en la altura. (In Spanish) Rev Asoc Med Prov Yauli (Peru) 1960;5:74–100. [Google Scholar]
- 47.Garrido-Klinge G, Pena L. Ulcera peptica en la altura. (In Spanish) Diagnostico (Peru) 1982;10:70–72. [Google Scholar]
- 48.Editorial. The Symptomatic Self Care for prevention and treatment of patients with peptic ulcerations. Chinese Health News. 1999-11-11 [Google Scholar]