

Abstract
We report a case of surgically proved left-sided torsion of the greater omentum that caused secondary by untreated inguinal hernia. Case A 36-year-old man presented to our hospital with abdominal pain. He had been diagnosed with a left inguinal hernia, but he had not received any treatments. Contrast-enhanced computed tomography (CT) of the abdomen showed a large fat density mass below the Sigmoid colon and left inguinal hernia with incarcerated fat. Exploratory laparotomy revealed torsion of the greater omentum with small bloody ascites. The greater omentum was twisted into one and a half circles and entered into a left inguinal hernia. An omentectomy with a repair of left inguinal hernia was performed. A resected omentum was submitted for pathological examination, which showed hemorrhagic infarction. Omental torsion is a rare cause of acute abdominal pain but should be included in the differential diagnoses of acute abdomen, especially in patients with untreated inguinal hernia.
Keywords: Omental torsion, Acute abdomen, Inguinal hernia
INTRODUCTION
Torsion of the omentum is a rare cause of acute abdomen, and twisting of the omentum may lead to subsequent vascular impairment and eventually progress to infarction of the segment of the omentum distal to the twisting point. In most cases, torsion occurs on the right side of great omentum and left-side torsion is infrequent[1,2].
We have reported a case of surgically proved left-sided torsion of the greater omentum that caused secondary torsion by untreated inguinal hernia.
CASE REPORT
A 36-year-old man presented to our hospital with abdominal pain of sudden onset. He had been diagnosed with a left inguinal hernia, but he had not received any treatment. Physical examination revealed tenderness in the left lower quadrant of the abdomen, but left inguinal swelling was not present. Blood examination showed leukocytosis (white blood cell count = 14 700/mm3), and the C-reactive protein (CRP) level was elevated (3.84 mg/dL). Plain abdominal X-rays showed a right upper deviation of the sigmoid colon. Contrast-enhanced computed tomography (CT) of the abdomen showed a large fat density mass below the sigmoid colon and left inguinal hernia with incarcerated fat (Figure 1). Conservative therapy including intravenous administration of antibiotics was performed. However, his symptoms were not resolved and a small collection of free fluid was noted within the peritoneal cavity by CT. Exploratory laparotomy was performed on March 29, 2004, which revealed torsion of the greater omentum with small amount of bloody ascites. The greater omentum was twisted into one and a half circles and entered into a left inguinal hernia (Figure 2). An omentectomy with a repair of left inguinal hernia was performed. A resected omentum was submitted for pathological examination, which showed hemorrhagic infarction. Post-operative course was uneventful, and the patient has remained healthy with no clinical evidence of recurrent disease since then.
Figure 1.
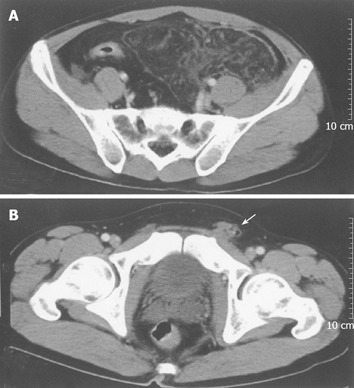
Contrast-enhanced computed tomography showing a large fat density mass below the sigmoid colon and left inguinal hernia with incarcerated fat (arrow).
Figure 2.
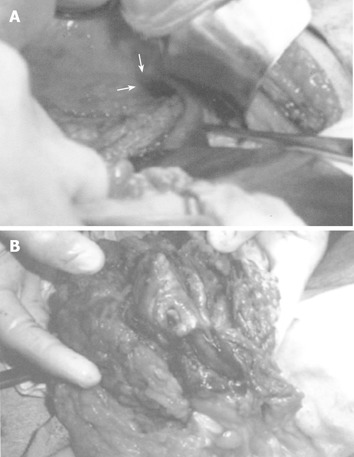
Twisting of greater omentum into one and a half circles and entering into a left inguinal hernia (arrow).
DISCUSSION
Torsion of the omentum is a rare cause of acute abdomen and the majority of cases have right-side torsion. Left-side torsion is extremely rare and there are only sporadic reports in the literature[1,2]. The greater susceptibility to torsion of the right side is due to its greater length and size in relation to the left side and its greater mobility[3].
Omental torsion can be classified as primary and secondary torsion, the latter being more common. Primary torsion is believed to be related to local omental anomalies, such as bulky bifid or accessory omentum or abnormally redundant omental veins, but the exact pathogenesis is yet to be uncovered[4]. Secondary torsion is associated with adhesions to cysts, tumors, inflammatory foci, scars, or hernias. The precipitating factors are shared in both omental torsions, which include sudden increase in intra-abdominal pressure following a heavy meal or exertion, change in body position, coughing or sneezing, and occupational use of vibrating tools[2,3]. These events may result in sudden displacement of the omentum, thus exposing the omentum to greater risk of torsion. Torsion leads to omental infarction and usually presents as acute abdominal pain.
The majority of the cases of omental torsion are torsion involving the right-side of the omentum with the right lower quadrant or right paraumbilical pain. Thus, the differential clinical diagnoses of omental torsion include acute appendicitis, acute cholecystitis, cecal diverticulitis, or appendagitis. Left-sided omental torsion as in our patient is unusual and clinically mimics sigmoid diverticulitis, or appendagitis.
Diagnosis of omental torsion is rarely made preoperatively but should become more frequent with the increasing use of CT in the diagnosis of acute abdominal conditions[5]. The CT findings of fatty mass with a whirling pattern in the greater omentum suggest omental torsion. Although this typical CT finding has been documented in literature from various countries[6,7], it should be made clear that not all omental torsions show this relatively characteristic appearance as in our case. The whirling pattern may not be apparent in cases where the axis of rotation is not perpendicular to the transverse scanning plane.
Concerning the treatment of omental torsion, resection of the involved segment of the omentum has traditionally been the treatment of choice[2]. However, a few reported cases of omental torsion that were successfully treated conservatively have been reported[2,5], especially in patients without associated complications. This may suggest that surgical treatment should be limited to the patients with complications. However, in cases where conservative treatments are not effective, as in our case, surgical treatments should be considered.
In conclusion, omental torsion is a rare cause of acute abdominal pain but should be included in the differential diagnoses of acute abdomen, especially in patients with untreated inguinal hernia. It is necessary to consider radiographic findings to determine how to best manage these patients and treat them.
Footnotes
S- Editor Kumar M, Guo SY and Xu XQ L- Editor Elsevier HK E- Editor Bi L
References
- 1.Balthazar EJ, Lefkowitz RA. Left-sided omental infarction with associated omental abscess: CT diagnosis. J Comput Assist Tomogr. 1993;17:379–381. doi: 10.1097/00004728-199305000-00007. [DOI] [PubMed] [Google Scholar]
- 2.Aoun N, Haddad-Zebouni S, Slaba S, Noun R, Ghossain M. Left-sided omental torsion: CT appearance. Eur Radiol. 2001;11:96–98. doi: 10.1007/s003300000545. [DOI] [PubMed] [Google Scholar]
- 3.Karayiannakis AJ, Polychronidis A, Chatzigianni E, Simopoulos C. Primary torsion of the greater omentum: report of a case. Surg Today. 2002;32:913–915. doi: 10.1007/s005950200180. [DOI] [PubMed] [Google Scholar]
- 4.Naffaa LN, Shabb NS, Haddad MC. CT findings of omental torsion and infarction: case report and review of the literature. Clin Imaging. 2003;27:116–118. doi: 10.1016/s0899-7071(02)00524-7. [DOI] [PubMed] [Google Scholar]
- 5.Kim J, Kim Y, Cho OK, Rhim H, Koh BH, Kim YS, Han DS, Baek HK. Omental torsion: CT features. Abdom Imaging. 2004;29:502–504. doi: 10.1007/s00261-003-0155-2. [DOI] [PubMed] [Google Scholar]
- 6.Maeda T, Mori H, Cyujo M, Kikuchi N, Hori Y, Takaki H. CT and MR findings of torsion of greater omentum: a case report. Abdom Imaging. 1997;22:45–46. doi: 10.1007/s002619900136. [DOI] [PubMed] [Google Scholar]
- 7.Yager A, Carmeci C. Torsion of the greater omentum: CT findings. AJR Am J Roentgenol. 1999;173:1139–1140. doi: 10.2214/ajr.173.4.10511205. [DOI] [PubMed] [Google Scholar]