

Abstract
Malignant gastrointestinal stromal tumors (GIST) are rare mesenchymal tumors originating from the wall of the gastrointestinal tract. Their coexistence with other tumors originating from other germ layers is unique. We have reported a case of a 63-year-old GIST patient presenting as an epigastric mass associated with hepatic tumor. Histologically, the mesenteric tumor was composed of spindle cells showing both neural and smooth muscle differentiation. Immunohistochemical examination showed positive staining for CD117, vimentin, S-100, and SMA, while CD34 antigen was negative. The hepatic tumor was diagnosed as hepatocellular carcinoma (HCC). To the best of our knowledge, this is the first case of GIST and HCC coexistence. The rarity of the case, however, should not lead to ignoring such a possibility in differential diagnosis.
Keywords: Malignant GIST, Hepatocellular carcinoma, Coexistence of GIST and HCC
INTRODUCTION
Malignant gastrointestinal stromal tumors (GIST) are rare mesenchymal tumors originating from the wall of the gastrointestinal tract[1,2]. Majority of GIST are positive for CD117 and vimentin in immunohistochemical staining[3-5]. Coexistence of malignant GIST and other malignancies have been reported in some unique cases[6-10]. Such cases always require differential diagnosis for metastatic GIST[3,4]. We have described a case of a 63-year-old male patient who was admitted to our clinic with liver tumor mass and mesenteric tumor. Preoperative biopsy performed under computed tomography (CT) scanning showed a mesenteric tumor as GIST, which was confirmed by postoperative histopathology. The liver tumor was verified as hepatocellular carcinoma (HCC). This case presents a coexistence of two independent tumors. To our knowledge, the coincidence of GIST and HCC has not been reported in the literature.
CASE REPORT
A 63-year-old male patient with a palpable epigastric mass was admitted to the Department of Surgical Oncology, Medical University of Gdansk. His medical history was significant for insulin dependent diabetes mellitus and ischemic heart disease. No other clinical symptoms were present. The morphology, serum alpha-fetoprotein (AFP), liver enzymes and other blood tests were normal.
CT of the patient’s abdomen showed an 80 mm×50 mm pathological mass in the right side of abdomen and a 65 mm×53 mm solid mass within the liver (Figures 1A and 1C). Abdominal sonography showed a 80-mm mass in diameter in the mesentery at the right side of the abdomen with mediocre flow in Doppler option and a 60-mm solid mass in diameter in the left lobe of the liver with low flow in Doppler option (Figures 1B and 1D). Laparotomy revealed a mesenteric tumor on the intestinal wall and a hepatic tumor of the same size as in ultrasonographic description (Figures 2A and 2B). No other malignant pathologies in the abdomen were found. Left hemihepatectomy and resection of mesenteric tumor with side-to-side jejunojejunostomy were performed.
Figure 1.
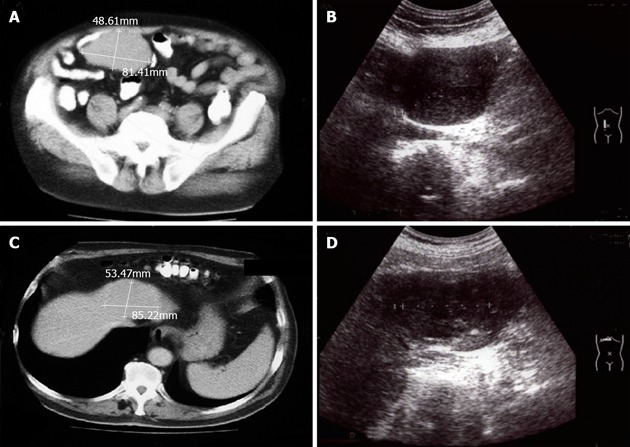
Computed tomography and sonography of mesenteric mass (A and B) and liver tumor (C and D).
Figure 2.
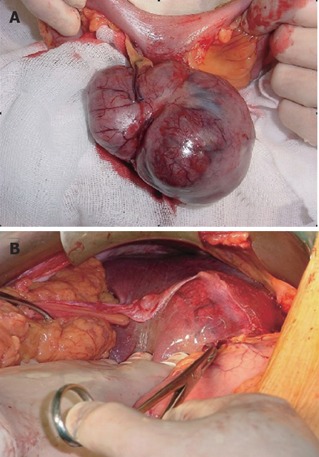
Mesenteric (A) and hepatic (B) tumors (intraoperative view).
Histologically, the liver tumor was described as HCC. The mesenteric tumor 70 mm×80 mm×60 mm in size was composed of spindle cells showing both neural and smooth muscle differentiation. Resection margins were histologically negative. Immunohistochemically, the tumor cells were positive for CD117, vimentin, SMA, S-100, and negative for CD34. Mitotic index was 10/50 HPF (10 pathological mitoses per 50 high-power field). The final pathological diagnosis of this tumor was gastrointestinal stromal tumor (GIST). The patient was discharged 9 d after tumor resection without surgical complications. No adjuvant therapy was prescribed, because the liver tumor was not metastasized from GIST. The patient after 18 mo of follow-up showed no signs of recurrent disease.
DISCUSSION
GIST are rare tumors that may arise from anywhere in the tubular gastrointestinal tract and give rise to metastases predominantly in the liver (more than 60% of metastases) or in the peritoneum[1,2,4,11,12]. In the present case, the solid mass in the liver was metastasized from the GIST. The histopathology showed that the tumor was a HCC. Coexistence of GIST and other primary tumors: renal carcinoma, bilateral pheochromocytoma, gastric cancer, and leiomyoma of the anorectum has been reported[6-10].
GIST may coexist also with inflammatory pseudotumors of the liver. These lesions are benign and characterized by proliferating fibrovascular tissue with inflammatory cells. They are associated with fever, pain and a mass effect. These clinical symptoms were not observed in our patient. The inflammatory pseudotumors are commonly mistaken for malignant tumors[13].
The described case is unique and should draw physicians’ attention to the possibility of independent tumor coexistence when GIST occurs. In patient with two tumors in the abdomen, GIST and HCC coexistence must be excluded. This is especially important in making a decision of adjuvant therapy. The current GIST treatment guidelines established by European Society for Medical Oncology (ESMO) for adjuvant therapy with imanitib can be applied in non-operable and/or metastatic tumors. Patients with resectable tumors without metastases should not receive adjuvant therapy. The radiotherapy value as an adjuvant treatment method for GIST is not documented in the literature[5].
The presence of hepatic tumor in patients with GIST should not judge the metastatic nature of liver tumors, though in the literature it is the most common cause of the coexisting liver tumor. Although two independent tumors in patients with GIST are unique, we must not exclude such a possibility and only careful histopathological examination gives us a correct diagnosis.
Footnotes
S- Editor Wang XL and Guo SY L- Editor Elsevier HK E- Editor Bi L
References
- 1.Tran T, Davila JA, El-Serag HB. The epidemiology of malignant gastrointestinal stromal tumors: an analysis of 1,458 cases from 1992 to 2000. Am J Gastroenterol. 2005;100:162–168. doi: 10.1111/j.1572-0241.2005.40709.x. [DOI] [PubMed] [Google Scholar]
- 2.Connolly EM, Gaffney E, Reynolds JV. Gastrointestinal stromal tumours. Br J Surg. 2003;90:1178–1186. doi: 10.1002/bjs.4352. [DOI] [PubMed] [Google Scholar]
- 3.Noguchi T, Sato T, Takeno S, Uchida Y, Kashima K, Yokoyama S, Müller W. Biological analysis of gastrointestinal stromal tumors. Oncol Rep. 2002;9:1277–1282. [PubMed] [Google Scholar]
- 4.Miettinen M, Sobin LH, Sarlomo-Rikala M. Immunohistochemical spectrum of GISTs at different sites and their differential diagnosis with a reference to CD117 (KIT) Mod Pathol. 2000;13:1134–1142. doi: 10.1038/modpathol.3880210. [DOI] [PubMed] [Google Scholar]
- 5.Blay JY, Bonvalot S, Casali P, Choi H, Debiec-Richter M, Dei Tos AP, Emile JF, Gronchi A, Hogendoorn PC, Joensuu H, et al. Consensus meeting for the management of gastrointestinal stromal tumors. Report of the GIST Consensus Conference of 20-21 March 2004, under the auspices of ESMO. Ann Oncol. 2005;16:566–578. doi: 10.1093/annonc/mdi127. [DOI] [PubMed] [Google Scholar]
- 6.Antonini C, Forgiarini O, Chiara A, Briani G, Belmonte P, Zucconelli R, Fiaccavento G, Sacchi G. [Stromal tumor of the ileum (GIST) at the same time as a renal carcinoma. Description of a case and review of the literature] Pathologica. 1998;90:160–164. [PubMed] [Google Scholar]
- 7.Fraggetta F. [On the latest case of renal carcinoma associated with GIST] Pathologica. 1999;91:62–63. [PubMed] [Google Scholar]
- 8.Rizzo S, Bonomo S, Moser A, Bottura D, Castellini C, Mazzola F, Lauro E, Vicenzi L, Betresini B, Angeli G, et al. [Bilateral pheochromocytoma associated with duodeno-jejunal GIST in patient with von Recklinghausen disease: report of a clinical case] Chir Ital. 2001;53:243–246. [PubMed] [Google Scholar]
- 9.Liu SW, Chen GH, Hsieh PP. Collision tumor of the stomach: a case report of mixed gastrointestinal stromal tumor and adenocarcinoma. J Clin Gastroenterol. 2002;35:332–334. doi: 10.1097/00004836-200210000-00010. [DOI] [PubMed] [Google Scholar]
- 10.Huilgol RL, Young CJ, Solomon MJ. The gist of it: Case reports of a gastrointestinal stromal tumour and a leiomyoma of the anorectum. ANZ J Surg. 2003;73:167–169. doi: 10.1046/j.1445-2197.2003.02643.x. [DOI] [PubMed] [Google Scholar]
- 11.Joensuu H, Kindblom LG. Gastrointestinal stromal tumors--a review. Acta Orthop Scand Suppl. 2004;75:62–71. doi: 10.1080/00016470410001708340. [DOI] [PubMed] [Google Scholar]
- 12.DeMatteo RP, Lewis JJ, Leung D, Mudan SS, Woodruff JM, Brennan MF. Two hundred gastrointestinal stromal tumors: recurrence patterns and prognostic factors for survival. Ann Surg. 2000;231:51–58. doi: 10.1097/00000658-200001000-00008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Lo OS, Poon RT, Lam CM, Fan ST. Inflammatory pseudotumor of the liver in association with a gastrointestinal stromal tumor: a case report. World J Gastroenterol. 2004;10:1841–1843. doi: 10.3748/wjg.v10.i12.1841. [DOI] [PMC free article] [PubMed] [Google Scholar]