

Abstract
AIM: To investigate whether microproteinuria in patients with inflammatory bowel disease (IBD) is associated with the disease activity or the treatment with 5-aminosalicylic acid (5-ASA).
METHODS: We prospectively studied microproteinuria in 86 consecutive patients with IBD, 61 with ulcerative colitis (UC) and 25 with Crohn’s disease (CD), before as well as 2 and 6 months after their inclusion in the study. Forty-six patients received 5-ASA for a period of 28.8 months (range 1-168 mo). Microalbuminuria (mALB) and urine levels of the renal tubular proteins β2-microglobulin (β2mGLB) and β-N-acetyl-D-glucosamidase (β-NAG) as well as the creatinine clearance were determined in a 12-h overnight urine collection. Tumor necrosis factor-α (TNF-α) serum levels were also measured.
RESULTS: A total of 277 measurements (194 in UC patients and 83 in CD patients) were performed. The prevalence of abnormal microproteinuria in UC and CD patients was 12.9% and 6.0% for mALB, 22.7% and 27.7% for β2mGLB, and 11.3% and 8.4% for β-NAG, respectively. mALB was not associated with IBD activity. β2mGLB and β-NAG urine levels were correlated to UC activity (UCAI: P<0.01; UCEI: P<0.005). mALB in UC patients and β-NAG urine levels in CD patients were related to TNF-α serum levels. An association was noticed between microproteinuria and smoking habit. Treatment with 5-ASA was not correlated to the severity of microproteinuria or to the changes of creatinine clearance.
CONCLUSION: Microproteinuria is mainly associated with UC and its activity but not affected by 5-ASA.
Keywords: Inflammatory bowel disease, Micropro-teinuria, 5-aminosalicylic acid
INTRODUCTION
Complications of the urinary system are not uncommon in patients with inflammatory bowel disease (IBD). Their incidence has been reported to vary from 4% to 23% and is greater in patients with more severe and long-standing disease[1]. Apart from secondary complications, such as nephrolithiasis, hydronephrosis and amyloidosis, other associations between IBD and renal disorders have also been described, regardless of treatment[2-5]. Membranous glomerulonephritis, rapidly progressive glomerulonephritis, mesangiocapillary glomerulonephritis, IgA nephropathy, thin basement membrane disease and kidney granuloma are connected with IBD[6-10]. In addition, non-specific morphological changes in the glomeruli of patients with IBD, such as podocyte effacement and mesangial deposition of immunoglobulin and complement have also been well documented[11]. On the contrary, cases of interstitial nephritis are attributed to the nephrotoxic effect of aminosalicylates[11]. However, before the establishment of 5-ASA as a treatment of choice in IBD, studies have identified renal tubular lesions in a proportion of patients[12]. Till date, more than 37 cases implicating the drug in interstitial nephritis (mainly mesalazine but also sulfasalazine, balsalazide, and olsalazine) have been reported to the Committee on Safety of Medicines (CSM)[13].
Abnormal microproteinuria [microalbuminuria (mALB) and/or tubular proteinuria] has been reported both in patients with ulcerative colitis (UC) and in those with Crohn’s disease (CD)[13-17]. Increased mALB, equivalent to an albumin excretion rate of 20-200 μg/min, is generally regarded as a sensitive indicator of glomerular disease and has been widely used as a clinical marker of incipient diabetic nephropathy[18]. Mahmud et al.[14] have found that there is a significant correlation between mALB and IBD activity. Increased urine levels of some tubular proteins, such as β-N-acetyl-D-glucosamidase (β-ΝAG), α1-microglobulin, β2-microglobulin (β2mGLB), alkaline phosphatase and gamma-glutamyltransferase, have been reported to be reliable indirect indices of renal tubular dysfunction[19]. Moreover, Riley et al.[15] have also found that the incidence of elevated urinary β-NAG is low in patients with quiescent UC, which is irrelevant to the dose and duration of mesalazine treatment. Kreisel et al.[17] reported that there is a strong correlation between abnormal tubular proteinuria and the activity of UC but not the activity of CD. On the contrary, Schreiber et al.[20] showed that increased prevalence of tubular proteinuria is attributed to high dosages of 5-ASA.
The etiology of abnormal microproteinuria in patients with IBD remains ambiguous. We conducted the present 6-month prospective study in order to investigate the incidence of mALB and tubular proteinuria in patients with IBD, emphasizing on the possible relationship between microproteinuria and the disease activity or the treatment with 5-ASA.
MATERIALS AND METHODS
Patients and sample selection
A total of 86 out of 166 screened consecutive Caucasian patients with confirmed chronic IBD (61 with UC and 25 with CD), treated at the Gastroenterology Department of the Red Cross Hospital of Athens from June 1998 to April 2001, were prospectively included in this study. Patients with signs of urinary tract infection and a history of acute or chronic nephropathy, diabetes mellitus, hypertension, severe liver disease, cardiac failure, use of non-steroidal anti-inflammatory drugs (NSAIDs) or other nephrotoxic drugs, patients with a present or recent pregnancy, patients treated with olsalazine, and patients who refused to participate in this study were excluded. Fifty patients were male, 36 were female and their mean age was 42.7 (range 15-77 years) years. Fifty-nine were out-patients and 27 were in-patients. At the time of their inclusion in this study, the IBD was active in 38 patients (27 with UC and 11 with CD) and inactive in 48 patients. Thirty out of eighty-six patients were first diagnosed with IBD (23 with UC and 7 with CD). The mean duration of the disease was 69.8 months (range 0-576 months). The group of patients with UC consisted of 16 patients with total colitis and 45 with left sided colitis (two of them with rectal disease only). The group of patients with CD included 11 patients with ileo-colonic disease, 8 with small bowel disease only and 6 with colonic disease only. Due to the small number of patients, two subgroups of patients with CD were considered in the subsequent analysis, one consisted of the patients with ileo-colonic or colonic disease and the other consisted of those suffering from small bowel disease only.
Extra-intestinal manifestations at present or during the last 2 months before the first meeting or during follow-up, were recorded in 29 patients (14 with UC, 15 with CD). Forty-six patients received mesalazine (Salofalk 2-3 g/day or Asacol 1.6-2.4 g/day) for a mean period of 28.8 months (range 1-168 months). During the last year, 20 of them were treated with prednisolone for a mean period of 1.9 months (range 1-12 months) and 6 with azathioprine for a mean period of 4.9 months (range 1-10 months).
According to the study design, all patients were evaluated at the time of their inclusion in the study (stage 1), two (stage 3) and six (stage 4) months afterwards. Twenty-seven patients (19 with UC, 8 with CD) with severely exacerbated disease at the time of their inclusion in the study were re-evaluated 10 days after intensive corticosteroid-based treatment (stage 2). A meticulous routine and more specific clinical and laboratory evaluation of the patients was conducted in each stage of the study, including determination of the hematocrit value, white blood cell and platelet count, serum levels of C-reactive protein (CRP) and tumor necrosis factor-alpha (TNF-α), usual urinalysis, levels of mALB and tubular proteinuria (β2mGLB, β-NAG) and creatinine clearance. Measurements of microproteinuria and creatinine clearance were performed using a 12-h urine collection, which has been proved equivalent to a 24-h urine collection[21] or an 8-h urine collection[22]. The criterion of our choice was the better compliance of our patients. The clinical disease activity quantifications were performed on the day of urine collection, using reliable activity indices for UC[23] and CD[24]. All patients with UC underwent colonoscopy at the 1st, 3rd, and 4th stages of the study and an endoscopic index of the activity of UC (UCEI)[25] was calculated for these patients[25]. Finally, a detailed drug history was taken from all the patients to confirm the type, dose and duration of medication.
The blood samples for the measurement of serum levels of TNF-α after centrifugation were stored at -48 °C. The urine samples for the determination of urine levels of microalbumin were stored at 2-8 °C for a time not exceeding 2 weeks, at -20 °C for β2mGLB and at -48 °C for β-NAG, respectively.
Microproteinuria (mALB and tubular proteinuria) was correlated to patients’ characteristics including sex, age, smoking habits; features of the diseases including activity, extent, duration, presence of extraintestinal manifestations; medication including type (mesalazine, corticosteroids, azathioprine) and duration. Furthermore, separate analyses of the courses of microproteinuria were conducted for patients with highly active disease at the time of their inclusion in the study and those with a first diagnosis of the disease, who did not receive any medication.
Analytical techniques (chemical analysis)
Urea and creatinine in serum as well as creatinine in urine were measured with standard techniques. Serum CRP concentrations were determined by nephelometry.
Urinary albumin concentrations were measured using a radioimmunologic assay (125I radioimmunologic analysis, EURO/DPC, Glyn Rhonwy, UK), which could indicate subtle increases in albumin excretion above the normal range but below that was detected by standard “dipstick” analysis (equivalent to a urinary albumin excretion rate of 20-200 μg/min)[26].
Urinary β2mGLB concentrations were measured using a radioimmunologic assay (125I radioimmunologic analysis, RADIM)[27].
Urinary β-NAG concentrations were determined colorimetrically using a commercially available kit (Boehringer-Mannheim, Germany). The optical density of the samples was measured at 580 nm (Cobas Bioanalyser, Roche). Results were calculated by reference to a standard curve[15,28].
Serum TNF-α was measured using a sandwich enzyme-linked immunosorbent assay (ELISA; Quantikine, R&D Systems Inc., Minneapolis, MN, USA: sensitivity 0.35 pg/mL)[29,30].
Quantification of disease activity
The activity of UC was quantified using the UC activity index (UCAI) introduced by Rachmilewitz[23]. A score greater than or equal to six was considered to be suggestive of active UC. The activity of CD was estimated according to the Best CD activity index (CDAI)[24]. CD was considered to be active in cases with CDAI greater than 150. Finally, the endoscopic activity of UC was also evaluated according to a reliable endoscopic index established by other researchers[25].
Statistical analysis
The Mann-Whitney U-test, the Wilcoxon rank-sum W-test and the Spearman’s rank correlation test were used for statistical evaluation of the non-parametric data. Student’s t-test was applied for statistical analysis of all parametric data. P<0.05 was considered statistically significant.
RESULTS
Eighty-two out of eighty-six patients participating in three stages of the study (time: 0, 2nd, and 6th month) completed the follow-up. Twenty-seven of them participated in one more stage (time: 10th day). Two out of eighty-six patients participated in two stages (time: 0, 10th day) and two in one stage only (time: 0). A total of 277 distinct evaluations were performed in 86 IBD patients, 194 in patients with UC and 83 in patients with CD. The IBD was active in 38 out of 86 patients at the 1st stage, in none out of 27 patients at the 2nd stage, in 7 out of 82 patients at the 3rd stage and in 6 out of 82 patients at the 4th stage of the study.
Abnormal urine levels of albumin (>18 μg/min), β2mGLB (>120 μg/min) and β-NAG (>5.9 U/L) were found in 12.9%, 22.7%, and 11.3% of the patients with UC and in 6%, 27.7%, and 8.4% of those with CD, respectively, more frequently in active than in inactive disease (Table 1). The mean values of mALB, tubular microproteinuria and creatinine clearance in active and inactive IBD are shown in Table 2. No differences in albuminuria were found between active or inactive UC and CD. In contrast, significantly higher urine levels of β2-mGLB were detected both in patients with active UC and in those with active CD. Urine levels of β-NAG were higher in active UC, but not in active CD.
Table 1.
Incidence of abnormal microproteinuria in patients with active and inactive IBD (%)
|
Ulcerative colitis (n = 194) |
Crohn's disease (n = 83) |
|||||
| Active (n = 49) UCAI ≥ 6 | Inactive (n = 145) UCAI < 6 | P | Active (n = 15) CDAI ≥ 150 | Inactive (n = 68) CDAI < 150 | P | |
| Urine m-ALB (>18 μg/min) | 16.3 | 11.7 | NS | 13.3 | 4.4 | 0.06 |
| Urine β2 mGLB (>120 μg/min) | 40.8 | 16.6 | < 0.001 | 53.3 | 22.1 | < 0.05 |
| Urine β-NAG (>5.9 U/L) | 26.5 | 6.2 | < 0.001 | 13.3 | 7.4 | NS |
Table 2.
Microproteinuria and creatinine clearance in active and inactive IBD (mean±SE)
|
Ulcerative colitis (n = 194) |
Crohn's disease (n = 83) |
|||||
| Active (n=49) | Inactive (n=145) | P | Active (n=15) | Inactive (n=68) | P | |
| Urine m-ALB (μg/min) | 11.89 ± 3.19 | 9.0 ± 1.03 | NS | 8.59 ± 2.65 | 7.02 ± 1.07 | NS |
| Urine β2mGLB (μg/min) | 204 ± 50.2 | 88.0 ± 10.28 | <0.01 | 359 ± 130.9 | 92.2 ± 16.26 | <0.05 |
| Urine β-NAG (U/L) | 4.69 ± 0.64 | 2.39 ± 0.16 | <0.001 | 3.07 ± 0.90 | 2.36 ± 0.25 | NS |
| Urine Kcr (mL/min) | 114.4 ± 6.03 | 120.3 ± 3.24 | NS | 135.6 ± 8.34 | 127.7 ± 3.96 | NS |
NS: Not significant.
Serum creatinine and its clearance
The levels of serum creatinine were normal in all the patients. Although creatinine clearance values varied widely, its mean values did not differ significantly between the patients with active and those with inactive UC (114.4±6.03 mL/min vs 120.3 ± 3.24 mL/min, P > 0.10) as well as between the patients with active and those with inactive CD (135.6±8.34 mL/min vs 127.7 ± 3.96 mL/min, P > 0.10). Our male IBD patients showed higher creatinine clearance values than female IBD patients (UC: 134 ± 3.19 mL/min vs 95 ± 4.07 mL/min, P < 0.001; CD: 137.1 ± 5.16 mL/min vs 118.8 ± 4.22 mL/min, P < 0.05). Creatinine clearance values were inversely correlated with the age of UC patients (ulcerative colitis: rp = -0.374, P < 0.001; CD: rp = -0.164, P > 0.10).
In addition, creatinine clearance values were higher in smokers with UC (smokers: 127 ± 4.04 mL/min; non- smokers: 114 ± 3.81 mL/min, P < 0.05) and in those with CD (smokers: 137.3 ± 4.50 mL/min; non-smokers: 113.1 ± 4.50 mL/min, P <0.001). Finally, no correlation of creatinine clearance values with 5-ASA treatment was observed (UC patients treated with and without 5-ASA: 119 ± 3.11 mL/min and 117 ± 7.25 mL/min, respectively, P = 0.987; CD patients treated with and without 5-ASA: 129±4.05 mL/min and 130±7.62 mL/min, respectively, P = 0.713).
Microproteinuria and IBD patients’ parameters
No correlation was found between microproteinuria (mALB or tubular proteinuria) and the age or the sex of our IBD patients (data not shown). However, albuminuria was significantly lower in smokers with UC than in non- smokers (smokers: 8.22±2.16 μg/min; non-smokers: 10.6±1.23 μg/min, P=0.021) and the urine levels of β-NAG were significantly lower in non-smokers with CD than in smokers (non-smokers: 1.62±0.19 U/L; smokers: 2.93±0.37 U/L, P = 0.023).
Microproteinuria and IBD activity
In our patients with UC, urinary concentrations of β-NAG were significantly correlated with the UCAI (rs = 0.26, P < 0.0005), the UCEI (rs = 0.23, P < 0.005) and the serum CRP levels (rs = 0.14, P < 0.05). Similarly, in these patients urinary levels of β2 mGLB were significantly associated with the UCAI (rs = 0.2, P < 0.01) but not with the UCEI or the serum CRP levels (Table 4). On the contrary, the patients with CD did not show any correlation of tubular microproteinuria with the parameters of their disease activity (Table 5).
Table 4.
Correlation between microproteinuria in patients with ulcerative colitis and disease activity parameters (n=194 measurements)
|
Ulcerative colitis activity parameters |
|||||||
| UCAI | UCEI | CRP | ESR | Platelets | Serum TNF-α | ||
| Urine m-ALB | rS | 0.0283 | 0.0420 | 0.0232 | 0.0091 | 0.0826 | 0.1665 |
| (μg/min) | P | 0.6954 | 0.5612 | 0.7479 | 0.9001 | 0.2520 | 0.0203 |
| Urine β2mGLB | rS | 0.1957 | 0.1037 | 0.1059 | 0.0033 | 0.0540 | 0.0123 |
| (μg/min) | P | 0.0062 | 0.1501 | 0.1414 | 0.9634 | 0.4543 | 0.8648 |
| Urine β-NAG | rS | 0.2633 | 0.2335 | 0.1438 | 0.1224 | 0.2336 | 0.1057 |
| (U/L) | P | 0.0002 | 0.0010 | 0.0455 | 0.0891 | 0.0010 | 0.1426 |
rS: Spearman’s correlation coefficient; rP: Pearson’s correlation coefficient.
Table 5.
Correlation between microproteinuria in patients with Crohn’s disease and disease activity parameters (n=83 measurements)
|
Crohn's disease activity parameters |
||||||
| CDAI | CRP | ESR | Platelets | Serum TNF-α | ||
| Urine m-ALB | rS | 0.1186 | 0.0326 | 0.0352 | 0.1483 | 0.1537 |
| (μg/min) | P | 0.2856 | 0.7686 | 0.7522 | 0.1810 | 0.1654 |
| Urine β2mGLB | rS | 0.0813 | 0.0187 | 0.0624 | 0.1727 | 0.2100 |
| (μg/min) | P | 0.4648 | 0.8669 | 0.5751 | 0.1184 | 0.0568 |
| Urine β-NAG | rS | 0.1106 | 0.0319 | 0.0947 | 0.0527 | 0.2676 |
| (U/L) | P | 0.3196 | 0.7744 | 0.3347 | 0.6359 | 0.0145 |
rS: Spearman’s correlation coefficient; rP: Pearson’s correlation coefficient.
No significant relationship was found between the levels of mALB and the disease activity in patients with UC neither in those with CD (Tables 4 and 5). A significant association between mALB and serum levels of TNF-α was noticed only in UC patients. Finally, a history of recent or present extra-intestinal manifestations did not influence the levels of mALB and tubular microproteinuria in IBD patients (data not shown).
Microproteinuria and IBD duration and extent
A significant inverse relationship was found between the levels of mALB and the duration of UC (rs = -0.24, P < 0.001). In contrast, a tendency towards a positive association was noticed between the severity of mALB and the duration of CD (rs = 0.19, P = 0.078). No significant differences were found between the levels of microproteinuria (mALB and tubular microproteinuria) and the extent of UC (total vs left side colitis) as well as the extent of CD (small intestine+colon vs small intestine only).
Microproteinuria and IBD therapy
No differences were found in the levels of mALB and tubular microproteinuria between the IBD patients who received or did not receive 5-ASA therapy (Table 3 and Figure 1). Moreover, no differences were found between the duration of 5-ASA treatment and the levels of mALB (UC: rs = -0.06, P = 0.43; CD: rs = 0.05, P = 0.70), the urinary levels of β2mGLB (UC: rs = 0.06, P = 0.42; CD: rs = 0.17, P = 0.16) and β-NAG (UC: rs = -0.02, P = 0.77; CD: rs = 0.02, P = 0.88). The levels of microproteinuria were also similar in the patients treated and those not treated with corticosteroids and/or azathioprine (data not shown).
Table 3.
Correlation of microproteinuria and creatinine clearance of IBD patients after 5-ASA treatment (mean±SE)
|
Ulcerative colitis (n=194)
5-ASA treatment |
P |
Crohn's disease (n=83)
5-ASA treatment |
P | |||
| No (n=37) | Yes (n=157) | No (n=15) | Yes (n=68) | |||
| Urine m-ALB (μg/min) | 8.99 ± 2.10 | 9.90 ± 1.29 | 0.794 | 8.08 ± 2.57 | 7.13 ± 1.08 | 0.562 |
| Urine β2mGLB (μg/min) | 163 ± 61.16 | 107 ± 12.07 | 0.852 | 274 ± 129.2 | 111.0 ± 20.15 | 0.083 |
| Urine β-NAG (U/L) | 4.22 ± 0.82 | 2.67 ± 0.18 | 0.118 | 2.79 ± 0.91 | 2.42 ± 0.26 | 0.845 |
| Urine Kcr (mL/min) | 117 ± 7.25 | 119 ± 3.11 | 0.987 | 130 ± 7.62 | 129 ± 4.05 | 0.713 |
Figure 1.
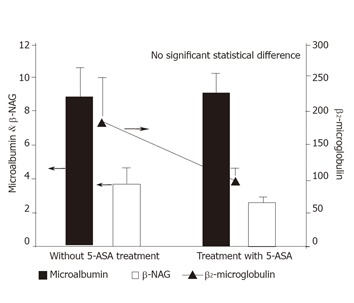
Correlation of IBD patients’ microproteinuria (mALB, β2mGLB, β-NAG) with 5-ASA treatment.
Microproteinuria in the first-diagnosed patients with active IBD
Among the 30 IBD patients with a first diagnosis of the disease at the time of their inclusion in this study, 22 had active IBD (17 had UC, 5 had CD). The 6-month course of mALB and tubular microproteinuria in the patients with an initially active IBD never treated with 5-ASA, exhibited a particular interest (Figure 2). In these patients, microproteinuria showed a tendency of gradual reduction by the time when IBD remission was achieved, although this reduction was statistically significant for β-NAG only.
Figure 2.
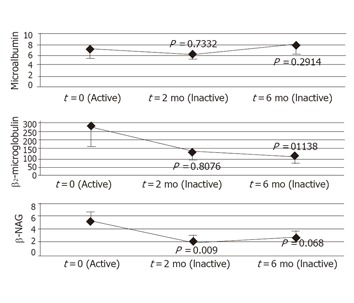
Changes of microproteinuria in the first-diagnosed patients with active IBD (n = 22) before and after inducing remission.
Microproteinuria in patients with severely active IBD
Twenty-seven of the patients (19 with UC, 8 with CD) were admitted to our hospital due to severely active disease. In these patients, we also evaluated the levels of microproteinuria in one more stage 10 days after the initiation of an intensive therapy (including corticosteroids). An early (10 days after) reduction of mALB (10.56 ± 2.27 μg/min vs 6.13 ± 1.43 μg/min, P < 0.01) as well as urine levels of β-NAG (5.60±1.10 U/L vs 3.17±0.60 U/L, P < 0.05) and β2mGLB (241.2 ± 96.82 μg/min vs 99.6 ± 33.33 μg/min, P > 0.10) was observed.
DISCUSSION
Although the incidence of renal complications is relatively low in patients with IBD, none of our patients developed clinically significant renal disease. No significant changes in serum creatinine and its clearance were recorded during the 6-month follow-up period. Furthermore, creatinine clearance was not correlated with the type, activity or the extent of IBD, which is in accordance with the majority of the published studies[13-17].
We observed a moderately abnormal mALB in 12.9% and 6% of our patients with UC and CD, respectively, which is in agreement with Fraser et al [13], Riley et al [15], Bonnet et al [31] and Zehnter et al [32]. Increased mALB reliably predicts diabetic nephropathy and an increased incidence of cardiovascular-related morbidity and mortality in diabetic and hypertensive patients as well as in the elderly[18,33,34]. Moreover, mALB has been described as a non-specific marker for acute illness[35], most probably as a result of the acute phase response to inflammatory mediators. It has been suggested that mALB in IBD patients may result from increased renal microvascular permeability in response to increased circulating cytokines[14,30,36]. This hypothesis is compatible with our finding of a significant relationship between mALB and serum TNF-α levels in our UC patients (P < 0.05), a thesis which is also supported by other researchers[13,15,31,32].
We did not find any significant correlation between the levels of mALB and the IBD activity, which is in agreement with many published studies[13,15]. In contrast, Mahmud et al.[14,37] found that increased mALB in the vast majority of IBD patients is related to both clinical and histopathological activities of the disease. Differences between these studies may be attributed to the varied disease activity. In our study, a relatively small proportion of the patients had a considerable disease activity.
Abnormal tubular microproteinuria, reflecting sub-clinical tubular damage, is a quite common finding among IBD patients[15,17]. However, its incidence varies widely[13-17,31,32,38], from 0% in the studies by Biddle et al [38] (β-NAG and β2mGLB) and Mahmud et al [14] (glutathione-S-transferase) to 75% in the study by Bonnet et al [31] (γ-glutamyl transferase and alkaline phosphatase). Hitherto, it has been difficult to prove whether tubular microproteinuria results from the effect of 5-ASA or is an extra-intestinal manifestation of the IBD itself[13]. Its structural similarity to other salicylates and non-steroidal anti-inflammatory drugs has led to the speculation that 5-ASA may cause tubulointerstitial damage of the kidney[11].
A significant correlation between tubular micropro-teinuria and IBD activity was found only in our patients with UC. This might be due to the fact that our patients with severely active CD were much fewer than those with UC. Kreisel et al.[17] have observed an increased urinary β-NAG excretion in 28% of the patients with UC and in 19% of those with CD, especially higher in active disease. Schreiber et al.[28] acknowledged their inability to determine whether high levels of tubular microproteinuria are attributable to the severity of the disease’s activity or 5-ASA treatment (or both), since 11% of their patients not receiving 5-ASA also had a tubular microproteinuria. Fraser et al.[13] found that urinary excretion of β-NAG and α1-microglobulin was increased in 48% and 52% of patients with IBD at diagnosis, respectively. A positive relationship between the urine levels of several tubular proteins and the IBD activity has been proposed by the majority of the inv-estigators[13-17,31,39]. In contrast, Zehnter et al.[32] showed that increased urine levels of β2-mGLB, alanine aminopeptidase and β-NAG in IBD patients were not correlated with the disease activity.
In this study, 22 first-diagnosed patients with active IBD had increased levels of tubular microproteinuria at diagnosis, which decreased after treatment with corticosteroids and 5-ASA. Moreover, 27 IBD patients with severely active disease manifested an early significant decrease of both microalbuminuria and tubular microproteinuria after being treated with corticosteroids. In addition, we found that there was a positive relationship between microalbuminuria and serum TNF-α levels, as well as between tubular microproteinuria and serum CRP and TNF-α levels, suggesting that microproteinuria in IBD patients may be related to a systemic inflammatory response and that it is an extra-intestinal manifestation of the active disease rather than a consequence of a subclinical renal injury due to 5-ASA treatment[13,15,17,20,31,32,37]. However, We did not find any differences in the severity of microproteinuria between the IBD patients with and those without a recent or present extra-intestinal manifestation of the disease, which is in agreement with Kreisel et al [17] and Mahmud et al [30].
Activation of the intestinal immune system, production of inflammation mediators or imbalance between activating and suppressing mediators play a pivotal role in the pathogenesis of IBD. In particular, TNF-α may play an important role in the inflammatory cascade of IBD and increased serum TNF-α levels have been reported in active IBD[40]. It has been reported that interleukin-1 and TNF-α inhibit the synthesis and induce a shedding of cell surface glycosaminoglycans[41], which might lead to an increased microvascular permeability and tissue damage[36,42].
No relationship was found between the severity of microproteinuria and the extent as well as the duration of IBD in our study, which is in concordance with other studies[14,20,32,43]. It is worth emphasizing on our finding of a significant correlation between microproteinuria and the smoking habit, which was negative in UC and positive in CD, because smoking alters the colonic mucosal blood flow[44] and decreases its permeability. Epidemiologic data suggest that smoking exerts a protective effect against UC[45] and is harmful to CD[45,46]. Consequently, differences in microproteinuria between smokers with UC and those with CD may be related to these pathophysiologic and epidemiologic data.
In this study, mALB was not correlated with the IBD treatment as it is almost universally accepted[13,15,31,32,37]. In addition, using sensitive markers of renal tubular toxicity[19], we were unable to find any evidence that treatment with mesalazine, corticosteroids or azathioprine was related to an increased tubular damage. However, this lack of correlation does not necessarily exclude nephrotoxicity. A potential nephrotoxicity of aminosalicylates, although rare, remains an existent possibility[11].
Riley et al [15] showed that there was no evidence of nephrotoxicity in a cohort of patients with quiescent UC receiving mesalazine or sulfasalazine. Furthermore, Kreisel et al [17] have demonstrated that there is no positive relationship between the cumulative dose of 5-ASA and the severity of tubular microproteinuria. In accordance to these studies, we observed that tubular microproteinuria in patients with active IBD at diagnosis decreased after inducing remission of the disease, even though the patients received the treatment with 5-ASA and corticosteroids. Fraser et al [13] have demonstrated that both the prevalence and degree of tubular microproteinuria in patients with a new diagnosis of IBD are relatively unaffected by 5-ASA treatment, which is in agreement with a number of studies[14,38,43,47]. In contrast, Schreiber et al [20] have reported that there is a positive relationship between tubular microproteinuria and cumulative 5-ASA exposure, but they questioned whether their study could provide a definite answer to the possible impact of chronic inflammation on microproteinuria. A similar positive relationship between tubular microproteinuria and 5-ASA treatment has also been reported[31,32].
In conclusion, abnormal mALB and tubular microproteinuria are quite frequent in IBD patients. Subclinical renal tubular and/or glomerular damage are related to the IBD itself, representing an extra-intestinal manifestation of the disease. Moreover, treatment with 5-ASA does not affect microproteinuria in IBD patients, microproteinuria in IBD patients does not predict an adverse renal response to 5-ASA.
Footnotes
S- Editor Wang XL and Guo SY L- Editor Elsevier HK E- Editor Li HY
References
- 1.Allan RN, Rhodes JM, Hanauer SB, Keighley MRB, Alexander-Williams J, Fazio VW (EDS) Inflammatory bowel disease. 3rd edition. New York: Churchill Livingstone; 1997. [Google Scholar]
- 2.Katsanos KH, Tsianos EV. The kidney in inflammatory bowel disease. Annals Gastroenterol. 2002;15:41–52. [Google Scholar]
- 3.Goerig M. Renal Complications and Manifestations in Crohn’s Disease. In: Lingua Med-Publishers Ltd. Extraintestinal Manifestations of Crohn’s Disease; 1992. pp. 57–60. [Google Scholar]
- 4.Pardi DS, Tremaine WJ, Sandborn WJ, McCarthy JT. Renal and urologic complications of inflammatory bowel disease. Am J Gastroenterol. 1998;93:504–514. doi: 10.1111/j.1572-0241.1998.156_b.x. [DOI] [PubMed] [Google Scholar]
- 5.Fitchen JH. Amyloidosis and granulomatous ileocolitis. Regression after surgical removal of the involved bowel. N Engl J Med. 1975;292:352–353. doi: 10.1056/NEJM197502132920709. [DOI] [PubMed] [Google Scholar]
- 6.Moayyedi P, Fletcher S, Harnden P, Axon AT, Brownjohn A. Mesangiocapillary glomerulonephritis associated with ulcerative colitis: case reports of two patients. Nephrol Dial Transplant. 1995;10:1923–1924. [PubMed] [Google Scholar]
- 7.Wilcox GM, Aretz HT, Roy MA, Roche JK. Glomerulonephritis associated with inflammatory bowel disease. Report of a patient with chronic ulcerative colitis, sclerosing cholangitis, and acute glomerulonephritis. Gastroenterology. 1990;98:786–791. [PubMed] [Google Scholar]
- 8.Dhiman RK, Poddar U, Sharma BC, Arora P, Saraswat VA, Pandey R, Naik SR. Membranous glomerulonephritis in association with ulcerative colitis. Indian J Gastroenterol. 1998;17:62. [PubMed] [Google Scholar]
- 9.McCallum D, Smith L, Harley F, Yiu V. IgA nephropathy and thin basement membrane disease in association with Crohn disease. Pediatr Nephrol. 1997;11:637–640. doi: 10.1007/s004670050355. [DOI] [PubMed] [Google Scholar]
- 10.Archimandritis AJ, Weetch MS. Kidney granuloma in Crohn's disease. BMJ. 1993;307:540–541. doi: 10.1136/bmj.307.6903.540. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Corrigan G, Stevens PE. Review article: interstitial nephritis associated with the use of mesalazine in inflammatory bowel disease. Aliment Pharmacol Ther. 2000;14:1–6. doi: 10.1046/j.1365-2036.2000.00683.x. [DOI] [PubMed] [Google Scholar]
- 12.Chapin LE, Scudamore HH, Baggenstoss AH, Bargen JA. Regional enteritis: associated visceral changes. Gastroenterology. 1956;30:404–415. [PubMed] [Google Scholar]
- 13.Fraser JS, Muller AF, Smith DJ, Newman DJ, Lamb EJ. Renal tubular injury is present in acute inflammatory bowel disease prior to the introduction of drug therapy. Aliment Pharmacol Ther. 2001;15:1131–1137. doi: 10.1046/j.1365-2036.2001.01041.x. [DOI] [PubMed] [Google Scholar]
- 14.Mahmud N, Stinson J, O'Connell MA, Mantle TJ, Keeling PW, Feely J, Weir DG, Kelleher D. Microalbuminuria in inflammatory bowel disease. Gut. 1994;35:1599–1604. doi: 10.1136/gut.35.11.1599. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Riley SA, Lloyd DR, Mani V. Tests of renal function in patients with quiescent colitis: effects of drug treatment. Gut. 1992;33:1348–1352. doi: 10.1136/gut.33.10.1348. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Herrlinger KR, Noftz MK, Fellermann K, Schmidt K, Steinhoff J, Stange EF. Minimal renal dysfunction in inflammatory bowel disease is related to disease activity but not to 5-ASA use. Aliment Pharmacol Ther. 2001;15:363–369. doi: 10.1046/j.1365-2036.2001.00940.x. [DOI] [PubMed] [Google Scholar]
- 17.Kreisel W, Wolf LM, Grotz W, Grieshaber M. Renal tubular damage: an extraintestinal manifestation of chronic inflammatory bowel disease. Eur J Gastroenterol Hepatol. 1996;8:461–468. [PubMed] [Google Scholar]
- 18.Mogensen CE. Microalbuminuria as a predictor of clinical diabetic nephropathy. Kidney Int. 1987;31:673–689. doi: 10.1038/ki.1987.50. [DOI] [PubMed] [Google Scholar]
- 19.Price RG, Whiting PH. Urinary enzymes and nephrotoxicity in humans. In: Jung K, Mattenheimer H, Burchardt U, eds , editors. Urinary Enzymes. Berlin: Springer-Verlag; 1992. pp. 203–221. [Google Scholar]
- 20.Schreiber S, Hämling J, Zehnter E, Howaldt S, Daerr W, Raedler A, Kruis W. Renal tubular dysfunction in patients with inflammatory bowel disease treated with aminosalicylate. Gut. 1997;40:761–766. doi: 10.1136/gut.40.6.761. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Gabriel R. Time to scrap creatinine clearance. Br Med J (Clin Res Ed) 1986;293:1568. doi: 10.1136/bmj.293.6561.1568. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Markantonis SL, Agathokleous-Kioupaki E. Can two-, four- or eight-hour urine collections after voluntary voiding be used instead of twenty-four-hour collections for the estimation of creatinine clearance in healthy subjects. Pharm World Sci. 1998;20:258–263. doi: 10.1023/a:1008674625308. [DOI] [PubMed] [Google Scholar]
- 23.Rachmilewitz D. Coated mesalazine (5-aminosalicylic acid) versus sulphasalazine in the treatment of active ulcerative colitis: a randomised trial. BMJ. 1989;298:82–86. doi: 10.1136/bmj.298.6666.82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Best WR, Becktel JM, Singleton JW, Kern F. Development of a Crohn's disease activity index. National Cooperative Crohn's Disease Study. Gastroenterology. 1976;70:439–444. [PubMed] [Google Scholar]
- 25.Taguchi Y, Miyaoka M, Saito T. [Endoscopic diagnosis of ulcerative colitis] Nihon Rinsho. 1999;57:2453–2456. [PubMed] [Google Scholar]
- 26.Osberg I, Chase HP, Garg SK, DeAndrea A, Harris S, Hamilton R, Marshall G. Effects of storage time and temperature on measurement of small concentrations of albumin in urine. Clin Chem. 1990;36:1428–1430. [PubMed] [Google Scholar]
- 27.Schweizer RT, Moore R, Bartus SA, Bow L, Hayden J. Beta 2-microglobulin monitoring after renal transplantation. Transplant Proc. 1981;13:1620–1623. [PubMed] [Google Scholar]
- 28.Yakata M, Sugita O, Sakai T, Uchiyama K, Wada K. [Urinary enzyme determination and its clinical significance. C. Enzyme derived from the kidney tubular epithelium--N-acetyl-beta-D-glucosaminidase. 4. Preclinical evaluation of the urinary NAG activity and changes in renal diseases] Rinsho Byori. 1983;Spec No 56:90–101. [PubMed] [Google Scholar]
- 29.Sharief MK, Hentges R. Association between tumor necrosis factor-alpha and disease progression in patients with multiple sclerosis. N Engl J Med. 1991;325:467–472. doi: 10.1056/NEJM199108153250704. [DOI] [PubMed] [Google Scholar]
- 30.Mahmud N, O'Connell MA, Stinson J, Goggins MG, Weir DG, Kelleher D. Tumour necrosis factor-alpha and microalbuminuria in patients with inflammatory bowel disease. Eur J Gastroenterol Hepatol. 1995;7:215–219. [PubMed] [Google Scholar]
- 31.Bonnet J, Lemman M, Prunat A. Renal function in patients with inflammatory bowel disease on long term mesalamine or olsalazine. Gastroenterology. 1995;108:A786(abstract). [Google Scholar]
- 32.Zehnter E, Dorhofer H, Ziegenhagen DJ, Scheurlen C, Baldamns CA, Kruis W. Renal damage in patients with IBD treated with 5-aminosalicylic acid and sulphasalazine. Gastroenterology. 1994;100:A264(abstract). [Google Scholar]
- 33.Mogensen CE, Keane WF, Bennett PH, Jerums G, Parving HH, Passa P, Steffes MW, Striker GE, Viberti GC. Prevention of diabetic renal disease with special reference to microalbuminuria. Lancet. 1995;346:1080–1084. doi: 10.1016/s0140-6736(95)91747-0. [DOI] [PubMed] [Google Scholar]
- 34.Jarrett RJ, Viberti GC, Argyropoulos A, Hill RD, Mahmud U, Murrells TJ. Microalbuminuria predicts mortality in non-insulin-dependent diabetics. Diabet Med. 1984;1:17–19. doi: 10.1111/j.1464-5491.1984.tb01915.x. [DOI] [PubMed] [Google Scholar]
- 35.Gosling P, Shearman CP. Increased levels of urinary proteins: marker of vascular permeability. Ann Clin Biochem. 1988;25(suppl):150–151. [Google Scholar]
- 36.Yi ES, Ulich TR. Endotoxin, interleukin-1, and tumor necrosis factor cause neutrophil-dependent microvascular leakage in postcapillary venules. Am J Pathol. 1992;140:659–663. [PMC free article] [PubMed] [Google Scholar]
- 37.Mahmud N, McDonald GS, Kelleher D, Weir DG. Microalbuminuria correlates with intestinal histopathological grading in patients with inflammatory bowel disease. Gut. 1996;38:99–103. doi: 10.1136/gut.38.1.99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Biddle W, Miner PB. Evaluation of potential nephrotoxicity of oral 5-ASA treatment of patients with ulcerative colitis abstract. Gastroenterology. 1989;96:A44. [Google Scholar]
- 39.Winstanley PA, Young JB, Axon AT, Brownjohn AM, Cooper EH. Renal proximal tubular dysfunction in Crohn's disease. Br Med J (Clin Res Ed) 1984;288:1612–1613. doi: 10.1136/bmj.288.6430.1612-e. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Maeda M, Watanabe N, Neda H, Yamauchi N, Okamoto T, Sasaki H, Tsuji Y, Akiyama S, Tsuji N, Niitsu Y. Serum tumor necrosis factor activity in inflammatory bowel disease. Immunopharmacol Immunotoxicol. 1992;14:451–461. doi: 10.3109/08923979209005404. [DOI] [PubMed] [Google Scholar]
- 41.Murch SH, MacDonald TT, Walker-Smith JA, Levin M, Lionetti P, Klein NJ. Disruption of sulphated glycosaminoglycans in intestinal inflammation. Lancet. 1993;341:711–714. doi: 10.1016/0140-6736(93)90485-y. [DOI] [PubMed] [Google Scholar]
- 42.Klein NJ, Shennan GI, Heyderman RS, Levin M. Alteration in glycosaminoglycan metabolism and surface charge on human umbilical vein endothelial cells induced by cytokines, endotoxin and neutrophils. J Cell Sci. 1992;102(Pt 4):821–832. doi: 10.1242/jcs.102.4.821. [DOI] [PubMed] [Google Scholar]
- 43.Sninsky C, Hanauer S, Powers B, Robinson M, Mayel F, Elson C, et al. Sensitive markers of renal dysfunction are elevated in chronic ulcerative colitis (abstract) World Congress of Gastroenterology. 1994;(Pt 4):A1778. [Google Scholar]
- 44.Srivastava ED, Russell MA, Feyerabend C, Rhodes J. Effect of ulcerative colitis and smoking on rectal blood flow. Gut. 1990;31:1021–1024. doi: 10.1136/gut.31.9.1021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Calkins BM. A meta-analysis of the role of smoking in inflammatory bowel disease. Dig Dis Sci. 1989;34:1841–1854. doi: 10.1007/BF01536701. [DOI] [PubMed] [Google Scholar]
- 46.Sutherland LR, Ramcharan S, Bryant H, Fick G. Effect of cigarette smoking on recurrence of Crohn's disease. Gastroenterology. 1990;98:1123–1128. doi: 10.1016/0016-5085(90)90324-t. [DOI] [PubMed] [Google Scholar]
- 47.Roth M, Steinhauer HB, Gerok W, Schlmerich J. Beta2 microglobulin and prostagladin E2 excretion is increased in patients with inflammatory bowel diseases- a new extraintestinal manifestation (abstract) Gastroenterology. 1991;100:A245. [Google Scholar]