

Abstract
AIM
To evaluate the central corneal thickness (CCT) measurements of premature infants
METHODS
The premature infants who were born between 25-34wk of gestational age (GA) were retrieved for the study. All CCT measurements were performed within the first 2d of their life under topical anesthesia by using an ultrasonic pachymeter.
RESULTS
The mean CCT of 200 eyes was 647.79±63.94 µm. The mean CCT of the right and left eyes were similar (647.30±64.72 µm and 648.29±63.47 µm consecutively). The mean CCT of the girls was 642.08±54.89 µm and the boys was 653.07±71.14 µm, with no statistically significant difference (P>0.05). But there was a negative correlation of the CCT with GA and birth weight (BW) (P<0.01).
CONCLUSION
The CCT values of premature babies were negatively correlated with GA and BW.
Keywords: central corneal thickness, measurement, prematurity
INTRODUCTION
Many studies formerly evaluated the central corneal thickness (CCT) in children but very little is known about the CCT in premature infants. Several studies showed that the CCT in term infants is relatively higher when compared to adults[1]–[3].
Central corneal thickness measurement has an important role in daily ophthalmology practice. Evaluating the CCT in glaucoma patients is a standart contemporary method. Lopes et al[4] assessed the CCT among pediatric cases with glaucoma and demonstrated higher CCT values in glaucoma group compared to the control group. In other studies demonstrating CCT measurements in congenital glaucoma, CCT was found to be thinner in glaucoma group compared to the control group[5],[6]. Simon et al[7] and Tai et al[8] showed that children with aphakic and pseudophakic glaucoma have thicker corneas compared to healthy subjects. As a result of postoperative endothelial cell damage the CCT increases in these patients. Therefore CCT measurements have a predictive value in aphakic and pseudophakic children who have a higher risk of glaucoma[9].
In a study, CCT was measured in 13 premature infants with a GA of 33wk or smaller, and no difference was found in the first and third postnatal weeks. However it was concluded that the CCT values reduced to levels similar with full-term babies at the age of 3mo[3]. In another study, measurements of the CCT and corneal diameter was performed in 35 premature babies (70 eyes) born at gestational ages of 23-32wk. The CCT showed a statistically significant decrease towards term in that study as well[10].
Only few studies about CCT measurements in premature infants are available in the literature. Therefore we aimed to investigate this important ocular parameter among premature infants in our study.
Statistical Analysis
NCSS (Number Cruncher Statistical System) 2007&PASS (Power Analysis and Sample Size) 2008 Statistical Software (Utah, USA) programme was used for statistical analysis. The descriptive statistics (Minimum, maximum, the mean CCT values of eyes, GA and birth weight (BW) of infants with standard deviation values) were expressed as mean±SD. Pearson correlation analysis was used to assess the relationship between the CCT values with GA and BW in the study. Oneway Anova test was used for the intergroup comparisons of the CCT values and Post-Hoc Tukey HSD test was used for the determination of the group that caused difference. Multivariate Linear regression analysis was used to determine the effects of GA and BW on the CCT values. Significance was assessed as P<0.05.
SUBJECTS AND METHODS
This retrospective study was carried out at the neonatal intensive care unit of Zeynep Kamil Women and Childrens' Diseases Education and Research Hospital. Totally 200 eyes of 100 premature infants were included in the study. The study was adhered to the tenets of the Declaration of Helsinki and a local ethical approvement was taken.
The CCT measurements were performed under topical anesthesia (Proparacaine hydrochloride 0.5%, Alcaine-Alcon, USA). All measurements were performed when the infants were at the supine position. An experienced nurse fixed the infant and a neonatologist attended to monitor the infant during the procedure. All measurements were performed 24-48h after delivery by one of the two observers (Gunary M and Celik G). The infants with neurological and systemic syndromes were excluded from the study.
The measurements were carried out by PalmScan AP2000-Ultima (Micro Medical Devices, USA) ultrasonic pachymeter device. The probe was located on the central cornea gently and several measurements were taken (eight measurements for each eye), and average reading was noted. An alcohol swab was used for disinfection of the probe tip before application to each eye. Prophylactic netilmicin eye drops, two times a day was ordered in both eyes for three days after the procedure. None of the infants had any sign of ocular surface disorder before or after the procedure.
RESULTS
Two-hundred eyes of 100 infants were included in the study. Fifty-two of the subjects were male and 48 were female. The mean GA was 29.50±2.89 (25-34) wk and the mean BW was 1259.80±401.75 (570-2250) g.
The mean CCT of 200 eyes was 647.79±63.94 µm (505-817 µm). The mean CCT of the right and left eyes were 647.30±64.72 µm and 648.29±63.47 µm consecutively (Table 1, Figure 1). The mean CCT of the boys was 653.07±71.14 µm and of the girls was 642.08±54.89 µm.
Table 1. Descriptive characteristics of premature infants.
| Parameters | n | Min-Max | Mean±SD |
| GA | 100 | 25-34 | 29.50±2.89 |
| BW | 100 | 570-2250 | 1259.80±401.75 |
| Right eyes CCT (µm) | 100 | 506-817 | 647.30±64.72 |
| Left eyes CCT (µm) | 100 | 505-807 | 648.29±63.47 |
| Mean CCT (µm) | 200 | 505-817 | 647.79±63.94 |
GA: Gestational age; BW: Birth weight; CCT: Central corneal thickness; SD: Standard deviation.
Figure 1. Mean CCT values of right, left and all eyes.
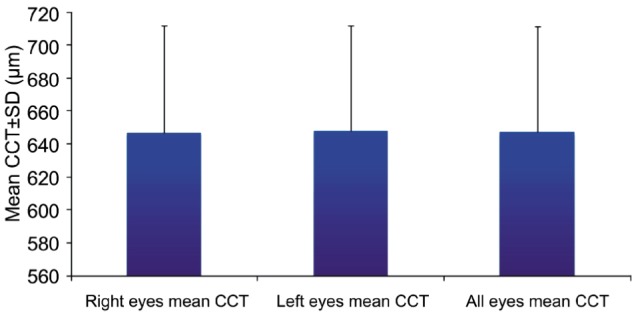
CCT: Central corneal thickness; SD: Standart deviation.
The mean CCT of infants GA with 25wk was 652.20±36.48 µm, 26wk was 676.10±53.17 µm, 27wk was 719.90±34.06 µm, 28wk was 679.30±48.22 µm, 29wk was 641.60±46.46 µm, 30wk was 638.25±42.56 µm, 31wk was 619.55±35.18 µm, 32wk was 605.80±59.52 µm, 33wk was 614.90±93.17 µm and 34wk was 630.35±77.70 µm. Post-Hoc Tukey HSD test was performed to determine the groups that caused the difference. The mean CCT of infants GA with 26wk was significantly higher compared to the infants GA with 31-33wk (P=0.048; P=0.004; P=0.022; P<0.05). The mean CCT of infants GA with 27wk was significantly higher compared to the infants GA with 25, 29-34wk (P=0.006; P=0.001; P=0.001; P=0.001; P=0.001; P=0.001; P=0.001; P<0.01). The mean CCT of infants GA with 28wk was significantly higher compared to the infants GA with 31-33wk (P=0.029; P=0.002; P=0.012; P<0.05). There was no statistical difference between the mean CCT values among the other GA groups (P>0.05) (Table 2, Figure 2).
Table 2. Mean CCT values and standard deviations for each GA week.
| GA (n=200) | Mean CCT (µm) |
||
| n | Mean | SD | |
| 25wk | 20 | 652.20 | 36.48 |
| 26wk | 20 | 676.10 | 53.17 |
| 27wk | 20 | 719.90 | 34.06 |
| 28wk | 20 | 679.30 | 48.22 |
| 29wk | 20 | 641.60 | 46.46 |
| 30wk | 20 | 638.25 | 42.56 |
| 31wk | 20 | 619.55 | 35.18 |
| 32wk | 20 | 605.80 | 59.52 |
| 33wk | 20 | 614.90 | 93.17 |
| 34wk | 20 | 630.35 | 77.70 |
GA: Gestational age; CCT: Central corneal thickness; SD: Standard deviation. Oneway Anova Test.
Figure 2. Mean CCT values for GA of all eyes.
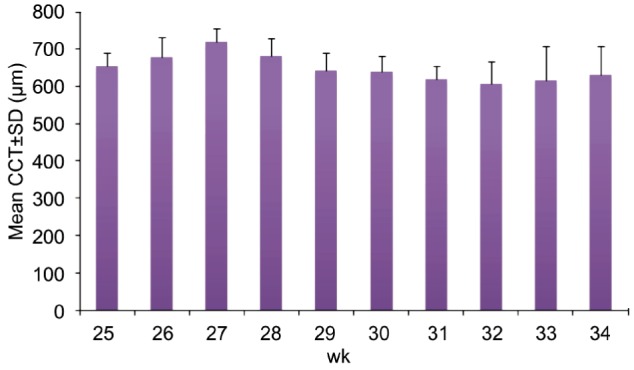
CCT: Central corneal thickness; SD: Standard deviation.
There was a negative correlation between the CCT of right, left and all eyes with GA and BW. The CCT showed a decrease with the increase of GA and BW (P<0.05). Furthermore, there was not a strong correlation of the CCT with GA and BW (Table 3, Figures 3–6).
Table 3. Correlation between central corneal thickness (CCT) and gestational age (GA) and birth weight (BW).
| Parameters | Right eye mean CCT (µm) (n=100) |
Left eye mean CCT (µm) (n=100) |
All eyes mean CTT (µm) (n=200) |
|||
| r | P | r | P | r | P | |
| GA (wk) | -0.391 | 0.001a | -0.361 | 0.001a | -0.376 | 0.001a |
| BW (g) | -0.275 | 0.006a | -0.252 | 0.012a | -0.264 | 0.001a |
r: Pearson correlation coefficient; aP<0.05.
Figure 3. Correlation between the mean CCT values of all eyes with GA.
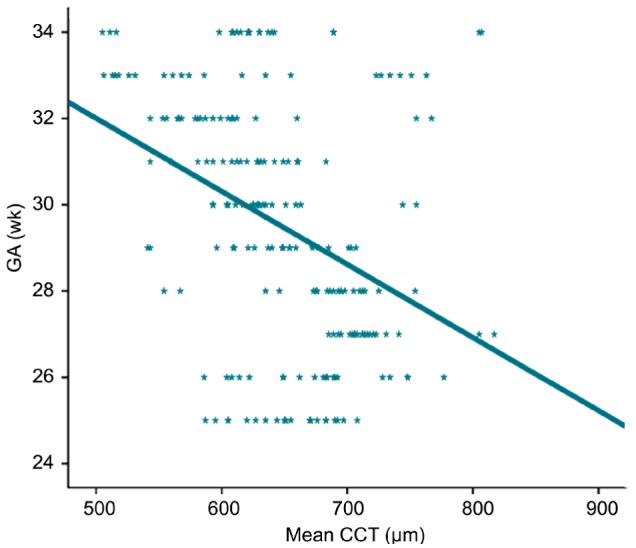
CCT: Central corneal thickness; GA: Gestational age.
Figure 6. Correlation between the mean CCT values of the right and left eyes with BW.
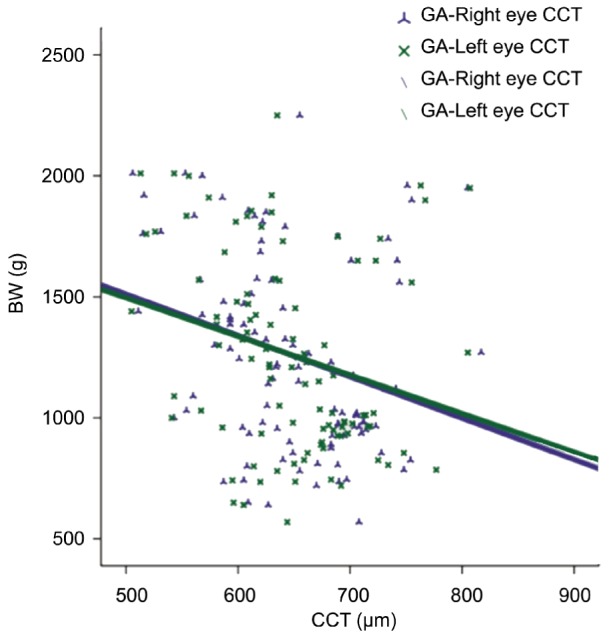
CCT: Central corneal thickness; BW: Birth weight.
There was no significant relationship of CCT measurements in males and females.
Figure 4. Correlation between the mean CCT values of the right and left eyes with GA.
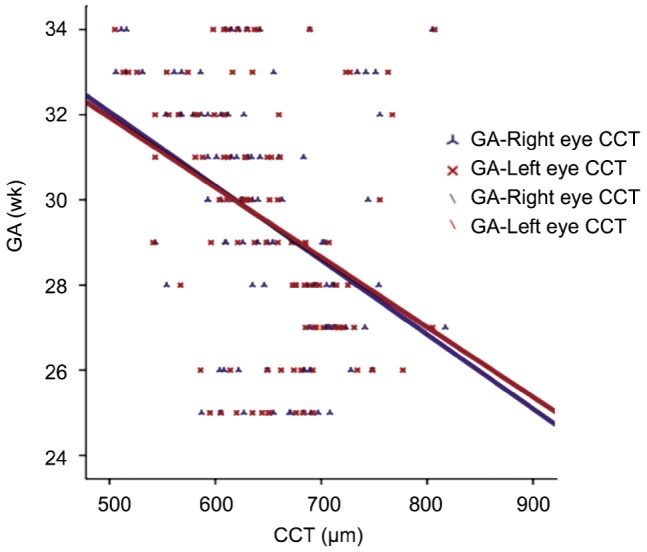
CCT: Central corneal thickness; GA: Gestational age.
Figure 5. Correlation between the mean CCT values of all eyes with BW.
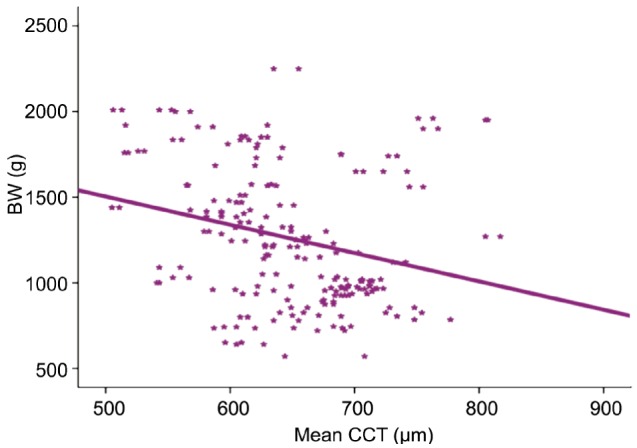
CCT: Central corneal thickness; BW: Birth weight.
The relationship between GA, BW and CCT was tested by a regression model. And the regression analysis demonstrated that the two predictors (GA and BW) were negatively correlated to the CCT (Table 4).
Table 4. The regression analysis of the parameters.
| Parameters | Unstandardized coefficients |
Standardized coefficients β | t | P | |
| β | Standart error | ||||
| CCT (µm) | 993.012 | 65.445 | 15.173 | 0.001b | |
| GA (wk) | -13.522 | 2.961 | -0.609 | -4.567 | 0.001b |
| BW (g) | 0.043 | 0.021 | 0.267 | 2.003 | 0.046a |
GA: Gestational age; BW: Birth weight. aP<0.05; bP<0.01.
DISCUSSION
Both central and peripheral corneal thickness measurements have been performed in several studies in adults[11]–[13]. The relationship between CCT and intraocular pressure (IOP) is also a well-known entity. The CCT should be assessed to obtain correct IOP values especially in daily glaucoma practice[14]–[19]. But the literature data demonstrating CCT measurements in children indicate a lesser extent than in adults and especially very little is known about the CCT in premature infants.
Autzen and Bjornstrom[3] have found the mean CCT as 654 µm in 13 premature infants in their study. They showed that CCT decreased significantly in the first few months. Also they could not demonstrate a correlation between CCT with GA and BW. This may be possible due to the small sample size of this study. In another study, CCT measurements were performed in 70 eyes of 35 premature babies[10]. The CCT decreased from 31wk to term in this study. Also we could not demonstrate a strong correlation of CCT with GA and BW in our study.
In a study including 200 eyes of 100 full-term newborns, the mean CCT was found as 616±61 µm. The mean CCT of males was significantly higher than females. Furthermore, the investigators did not mention any correlation of CCT with GA, BW, birth length and head circumference[20]. In our study we did not measure the birth length and head circumference of the infants. We aimed to reveal the correlation of CCT with GA and BW. We did not find any significant correlation between CCT measurements in males and females. But contrary to the aforementioned study we have observed a statistically significant but not a strong correlation of CCT with GA and BW. The CCT showed a decrease with the increase of GA and BW in our present study. Moreover we assessed our correlation of CCT with GA and BW by a regression model. And the results of the regression indicated that GA and BW significantly predicted the CCT values (GA; β=-13.52, P<0.01, BW; β=0.04, P<0.05).
Uva et al[21] evaluated IOP and CCT measurements in 33 premature and 33 full-term infants in their study. They found the mean CCT as 600 µm in premature infants and 580 µm in full-term infants. They observed higher IOP values in premature infants compared to full-term infants. Here it was emphasized that higher CCT can be shown as a reason for reading high IOP values. As can be seen here, measurement of the corneal thickness takes an important place especially in premature neonates.
Our study is primarily distinct because of a large number of premature infants. In our study, the mean GA at delivery was 30wk and the mean BW was 1260 g. These values were lower than the previosly mentioned studies which examined the CCT values in premature infants. Also in terms of the number of cases, our study had a greater range than above-mentioned studies. In our study the mean CCT showed a reduction with increasing GA and BW. This result was consistent with the literature data. But the relationship between the CCT with GA and BW was not clear in the previous studies as well as we did not observe a strong correlation between these parameters[3],[10],[21]. However, our study has a disadvantage because of its retrospective nature.
Better controlling of corneal hydration and increase in evaporation rate may be considered for the reduction in corneal thickness after premature and full-term birth. Also increase in corneal diameter and decrease in corneal curvature may cause this decrease in corneal thickness providing a kind of remodelling[2],[3],[10],[22].
In a study performed by Hussein et al[23] CCT measurements were performed in 198 eyes of 108 children with ages ranging between 6mo to 14y old. The mean CCT and the mean paracentral corneal thickness was 549 µm and 571 µm prospectively in this pediatric cohort. This study carried out beneficial results about pediatric corneal thickness especially to obtain more accurate IOP readings and for pre-operative examination in pediatric refractive surgery. However, this study does not display CCT measurements of children who are in their earlier periods, especially in premature babies.
When we combine previous literature data with our current study, central cornea is thicker both in premature and full-term births. The CCT value depicting a rapid decrease in first few months increases gradually for more than 9y of age[1]–[3].
It is argued that high CCT value in a premature newborn is related especially to corneal hydration. A hazy cornea is the typical view in a premature newborn with reduced corneal transparency. But in fact corneal transparency develops during fetal life. Studies on chick corneas showed that after embryonic 14th day chick stroma has a progressive dehydration and water proportion of the cornea decreases. The onset of transparency is linked with this dehydration. After arrangement of uniform and thin collagen fibrils as a consequence of some ultrastructural mechanisms like stromal matrix compaction and bioassembly, the transparent cornea becomes permanent[24].
Our main goal in this study was to assess the CCT in premature newborns. Congenital glaucoma can be a serious problem in such neonates doubtlessly. In this study we aimed to illuminate the diagnosis and monitoring of such diseases that can be seen in premature infants. The CCT is necessary to fix the IOP readings in routine ophthalmology practice. However there are other parameters affecting the IOP measurements in a newborn baby, assessing only IOP and CCT measurements may not be so helpful. An accurate evaluation of IOP in a premature infant requires some other parameters such as axial length, corneal curvature and diameter, corneal astigmatism and refractive error[25].
Our study with a large number of subjects displays significant results in CCT changes in premature infants but disadvantageous because of its retrospective nature. In order to obtain more accurate results, prospective and large-scale studies should be performed.
Acknowledgments
Conflicts of Interest: Gunay M, None; Celik G, None; Gunay BO, None; Dogru M, None; Gursoy T, None; Ovali HF, None.
REFERENCES
- 1.Ehlers N, Sorensen T, Bramsen T, Poulsen EH. Central corneal thickness in newborns and children. Acta Ophthalmol (Copenh) 1976;54(3):285–290. doi: 10.1111/j.1755-3768.1976.tb01257.x. [DOI] [PubMed] [Google Scholar]
- 2.Portellinha W, Belfort R., Jr Central and peripheral corneal thickness in newborns. Acta Ophthalmol (Copenh) 1991;69(2):247–250. doi: 10.1111/j.1755-3768.1991.tb02719.x. [DOI] [PubMed] [Google Scholar]
- 3.Autzen T, Bjørnstrøm L. Central corneal thickness in premature babies. Acta Ophthalmol (Copenh) 1991;69(2):251–252. doi: 10.1111/j.1755-3768.1991.tb02720.x. [DOI] [PubMed] [Google Scholar]
- 4.Lopes JE, Wilson RR, Alvim HS, Shields CL, Shields JA, Calhoun J, Fontanarosa J, Steinmann WC. Central corneal thickness in pediatric glaucoma. J Pediatr Ophthalmol Strabismus. 2007;44(2):112–117. doi: 10.3928/01913913-20070301-05. [DOI] [PubMed] [Google Scholar]
- 5.Henriques MJ, Vessani RM, Reis FA, de Almeida GV, Betinjane AJ, Susanna R., Jr Corneal thickness in congenital glaucoma. J Glaucoma. 2004;13(3):185–188. doi: 10.1097/00061198-200406000-00002. [DOI] [PubMed] [Google Scholar]
- 6.Wygnanski-Jaffe T, Barequet IS. Central corneal thickness in congenital glaucoma. Cornea. 2006;25(8):923–925. doi: 10.1097/01.ico.0000225712.62511.1c. [DOI] [PubMed] [Google Scholar]
- 7.Simon JW, O'Malley MR, Gandham SB, Ghaiy R, Zobal-Ratner J, Simmons ST. Central corneal thickness and glaucoma in aphakic and pseudophakic children. J AAPOS. 2005;9(4):326–329. doi: 10.1016/j.jaapos.2005.02.014. [DOI] [PubMed] [Google Scholar]
- 8.Tai TY, Mills MD, Beck AD, Joos KM, Ying GS, Liu C, Piltz-Seymour JR. Central corneal thickness and corneal diameter in patients with childhood glaucoma. J Glaucoma. 2006;15(6):524–528. doi: 10.1097/01.ijg.0000212293.93292.c9. [DOI] [PubMed] [Google Scholar]
- 9.Muir KW, Duncan L, Enyedi LB, Wallace DK, Freedman SF. Central corneal thickness: congenital cataracts and aphakia. Am J Ophthalmol. 2007;144(4):502–506. doi: 10.1016/j.ajo.2007.06.004. [DOI] [PubMed] [Google Scholar]
- 10.Kirwan C, O'Keefe M, Fitzsimon S. Central corneal thickness and corneal diameter in premature infants. Acta Ophthalmol Scand. 2005;83(6):751–753. doi: 10.1111/j.1600-0420.2005.00559.x. [DOI] [PubMed] [Google Scholar]
- 11.Tomlinson A. A clinical study of the central and peripheral thickness and curvature of the human cornea. Acta Ophthalmol (Copenh) 1972;50(1):73–82. doi: 10.1111/j.1755-3768.1972.tb05643.x. [DOI] [PubMed] [Google Scholar]
- 12.Iester M, Telani S, Frezzotti P, Manni G, Uva M, Figus M, Perdicchi A, Italian Glaucoma Register Differences in central corneal thickness between the paired eyes and the severity of the glaucomatous damage. Eye (Lond) 2012;26(11):1424–1430. doi: 10.1038/eye.2012.179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Brandt JD, Gordon MO, Beiser JA, Lin SC, Alexander MY, Kass MA, Ocular Hypertension Treatment Study Group Changes in central corneal thickness over time: the ocular hypertension treatment study. Ophthalmology. 2008;115(9):1550–1556. doi: 10.1016/j.ophtha.2008.02.001. [DOI] [PubMed] [Google Scholar]
- 14.Iester M, Telani S, Brusini P, Rolle T, Fogagnolo P, Martini E, Milano G, Paoli D, Italian Glaucoma Register D Central corneal thickness and glaucoma treatment: an Italian multicenter cross-sectional study. J Ocul Pharmacol Ther. 2013;29(5):469–473. doi: 10.1089/jop.2012.0116. [DOI] [PubMed] [Google Scholar]
- 15.Viswanathan D, Goldberg I, Graham SL. Relationship of change in central corneal thickness to visual field progression in eyes with glaucoma. Graefes Arch Clin Exp Ophthalmol. 2013;251(6):1593–1599. doi: 10.1007/s00417-013-2295-6. [DOI] [PubMed] [Google Scholar]
- 16.Ntim-Amponsah CT, Seidu AY, Essuman VA, Fordjour G, Tagoe NN, Coker A, Adam-Zakariah LI. A study of central corneal thickness in glaucoma and nonglaucoma patients in a West African population. Cornea. 2012;31(10):1093–1096. doi: 10.1097/ICO.0b013e31823c51f7. [DOI] [PubMed] [Google Scholar]
- 17.Azar G, Voigt M, Al-Arabi Z, Lachkar Y. Primary open-angle glaucoma (POAG), retinal vein occlusions (RVO) and central corneal thickness (CCT): What is the relationship? J Fr Ophtalmol. 2013;36(5):449–454. doi: 10.1016/j.jfo.2012.11.009. [DOI] [PubMed] [Google Scholar]
- 18.Wells M, Wu N, Kokkinakis J, Sutton G. Correlation of central corneal thickness measurements using Topcon TRK-1P, Zeiss Visante AS-OCT and DGH Pachmate 55 handheld ultrasonic pachymeter. Clin Exp Optom. 2013;96(4):385–387. doi: 10.1111/cxo.12013. [DOI] [PubMed] [Google Scholar]
- 19.Al-Farhan HM, Al-Otaibi WM. Comparison of central corneal thickness measurements using ultrasound pachymetry, ultrasound biomicroscopy, and the Artemis-2 VHF scanner in normal eyes. Clin Ophthalmol. 2012;6:1037–1043. doi: 10.2147/OPTH.S32955. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Rushood AA, Zahrani MH, Khamis A, Rushood AA. Central corneal thickness in full-term Saudi newborns. Acta Ophthalmol. 2012;90(5):355–358. doi: 10.1111/j.1755-3768.2012.02412.x. [DOI] [PubMed] [Google Scholar]
- 21.Uva MG, Reibaldi M, Longo A, Avitabile T, Gagliano C, Scollo D, Lionetti E, Reibaldi A. Intraocular pressure and central corneal thickness in premature and full-term newborns. J AAPOS. 2011;15(4):367–369. doi: 10.1016/j.jaapos.2011.04.004. [DOI] [PubMed] [Google Scholar]
- 22.Remón L, Cristóbal JA, Castillo J, Palomar T, Palomar A, Pérez J. Central and peripheral corneal thickness in full-term newborns by ultrasonic pachymetry. Invest Ophthalmol Vis Sci. 1992;33(11):3080–3083. [PubMed] [Google Scholar]
- 23.Hussein MA, Paysse EA, Bell NP, Coats DK, Brady McCreery KM, Koch DD, Orengo-Nania S, Baskin D, Wilhelmus KR. Corneal thickness in children. Am J Ophthalmol. 2004;138(5):744–748. doi: 10.1016/j.ajo.2004.06.030. [DOI] [PubMed] [Google Scholar]
- 24.Quantock AJ, Young RD. Development of the corneal stroma, and the collagen-proteoglycan associations that help define its structure and function. Dev Dyn. 2008;237(10):2607–2621. doi: 10.1002/dvdy.21579. [DOI] [PubMed] [Google Scholar]
- 25.Broman AT, Congdon NG, Bandeen-Roche K, Quigley HA. Influence of corneal structure, corneal responsiveness, and other ocular parameters on tonometric measurement of intraocular pressure. J Glaucoma. 2007;16(7):581–588. doi: 10.1097/IJG.0b013e3180640f40. [DOI] [PubMed] [Google Scholar]