

Abstract
Objectives:
The objective of the following study is to evaluate the usefulness of ultrasonography (USG) in comparison with conventional radiography and computed tomography (CT) scan in the diagnosis of zygomatic arch and mandibular fractures.
Materials and Methods:
A total of 40 patients with suspected fracture of the zygomatic arch and/or mandibular fractures were included in the study. Two groups (one for zygomatic arch fractures and the other for mandibular fractures) of 20 patients each were designed for the study. Ultrasonographic examinations were performed using small linear probe (LA435, Siemens Acuson Antares) with 10 MHz frequency. Data from CT and conventional radiography were compared with that of USG.
Results:
Sensitivity and specificity of USG in assessing zygomatic arch fractures were 100% and 100%, respectively; and that of mandibular fractures were 94.74% and 100%, respectively. Overall sensitivity, specificity, positive predictive value, and negative predictive value of USG against CT in diagnosing zygomatic arch and mandibular fractures were found out to be 97.4%, 100%, 100%, and 66.7%, respectively.
Conclusion:
USG is a very reliable tool in detection of fractures involving zygomatic arch and mandible. It can be used for screening of suspected fractures of zygomatic arch and mandible to avoid unnecessary radiation exposure from conventional radiography and CT scans.
Keywords: Computed tomography, mandibular fracture, orthopantomogram, submentovertex, ultrasonography, zygomatic arch fracture
Introduction
Maxillofacial injuries such as mandibular and zygomatic arch fractures are usually the result of acute and direct trauma to the side of the face. The zygomatic arch, a laterally positioned element of the craniofacial skeleton and mandible, which gives the contour to the lower third of the face, is susceptible to local trauma. Leading causes of fractures include assault, motor vehicle or motorcycle accidents, sports injuries, and falls. The mandible and zygomatic arch play an important role in facial contour and their malposition can also affect the cosmetic and normal unhindered excursion of the coronoid process of the mandible. Therefore, for both cosmetic and functional reasons, it is imperative that maxillofacial injuries be properly and fully diagnosed, and adequately treated.[1]
Rapid developments in computing hardware and microelectronic technology have facilitated technological advancement in ultrasonography (USG) in the last 3 decades, making it applicable not only to soft-tissues, but also to bony lesions of the head and neck.[2,3] This has increased interest in evaluating ultrasound imaging as an alternative to conventional radiography and computed tomography (CT) in the diagnostic evaluation of maxillofacial fractures.[4]
This study highlights the prospect of radiation free USG in diagnosis of facial fractures like zygomatic arch and mandible in comparison with CT and conventional radiography.
Materials and Methods
In this study, a total of 40 patients with clinically suspected fracture of zygomatic arch and mandibular fractures were included and were divided into two groups-Group I (20 patients with zygomatic arch fracture) and Group II (20 patients with mandibular fracture). The study was carried out after the approval by the Institutional Ethical Committee. After explaining thoroughly the procedures to be performed to the patients regarding the study, an informed consent was obtained.
Conventional radiographs (submentovertex for suspected zygomatic arch fracture and orthopantomogram for suspected mandible fracture) and CT scans (axial and coronal sections) were taken for all patients. The X-ray machine used for taking submentovertex view was 60 mA X-ray unit with parameters set at 65 KV and 40 mA. Proline orthopantomogram machine was used for mandibular exposure with parameters set at 76 KV, 8 mA and exposure time of 18 s. Asteion 5th generation spiral CT machine was used to take axial and coronal sections.
A small linear transducer or probe (LA435, Siemens Acuson Antares ultrasound system) with 10 MHz was used for ultrasonographic examinations. Patient was kept in supine position and a sterile gel was applied over the areas to be examined [Figure 1]. The probe was used to spread the gel over the areas of suspected fracture in zygomatic arch or mandible; and examination of the whole arch or mandible was carried out. Any break or displacement or step in the continuity of the outer cortex of the arch contour as seen on conventional radiography [Figure 2a] or CT scan [Figure 2b] or ultrasonography [Figure 2c] or mandible was considered to be a fracture. Any breach if detected, the distance between the two fragments was measured using ultrasonographic calipers to determine the displacement between the fracture fragments. All of the ultrasonographic examinations were done and interpreted by the same sonologist, who was blinded to the results of the CT scan and the conventional radiography. Sensitivity, specificity, and predictive values were calculated by comparing data obtained from ultrasound examination with the CT and conventional radiographic findings.
Figure 1.

Ultrasonographic examination of zygomatic arch with probe
Figure 2.

(a) Cropped submentovertex radiograph showing zygomatic arch fracture. (b) Cropped computed tomography showing the same zygomatic arch fracture. (c) Ultrasonography showing the same zygomatic arch fracture
Results
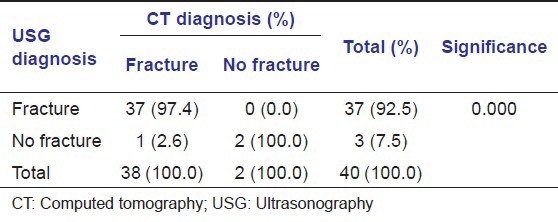
The patients were 39 men and one women aged from 18 to 54 years (mean 34.03 years). Scanning and processing of CT took an average of 20.90 min while conventional radiography took an average of 9.35 min. On the other hand, USG took an average of 3.50 min [Table 1]. Zygomatic arch fractures were more common on right side (60%) when compared to left side (35%). Mandibular fractures were most common on right side condyle (19%) and left mandibular angle (19%) followed by left condyle (14%) and left parasymphysis (14%), symphysis (10%) and body (10%), and right parasymphysis (9%). Overall sensitivity, specificity, positive predictive value and negative predictive value of USG against CT in diagnosing zygomatic arch and mandibular fractures were found out to be 97.4% [Table 2], 100%, 100%, and 66.7%, respectively. The diagnostic power of conventional radiography and USG in diagnosing zygomatic arch and mandibular fractures were same in this study but lower than CT.
Table 1.
Scanning and processing time (min)
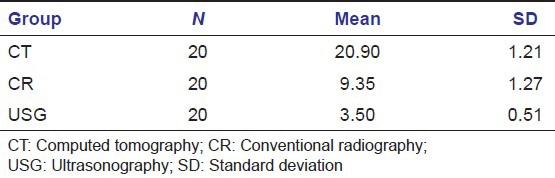
Table 2.
Overall fracture diagnosis of USG against CT scan
Discussion
Ultrasonography is a quick, noninvasive diagnostic imaging modality with no risk of radiation exposure as it only uses sound waves. It was originally used for soft-tissue evaluation. A breakthrough was made by Ord et al.[5] in the imaging of maxillofacial fractures when they used USG for evaluation of orbital fractures.
Gross swelling and tenderness over the fracture can make the procedure uncomfortable for the patient and can also make scanning of the bony outlines difficult, decreasing the accuracy of the process.[6] In this present study, there was not much difficulty in examination of patients with gross swelling and tenderness. Reduced tenderness may be because of the analgesic effect of medications taken by the patients. Moreover, it was also observed that isolated zygomatic arch or mandibular fractures were associated with minimal degree of swelling and tenderness.
Unlike CT scan or conventional radiography, USG has a drawback of inability to relate a fractured site to surrounding normal anatomical landmarks.
In this study, displaced, minimally displaced, undisplaced, and step-like fractures were well-demonstrated by USG. Step-like, displaced fractures were easier to diagnose when compared to minimally displaced fractures and undisplaced fractures. A minimum of 0.2 mm disruption in the fractured site was identified. This finding is consistent with the report of Hirai et al.[7] that high resolution echography allows the identification of even 0.1 mm wide disruptions of the bony surface. This shows USG is useful not only in detecting displaced fractures, but also may be useful in fractures like greenstick fractures.[6]
For condylar examination, effort must be made to place the probe along an imaginary line [Figure 3] to be able to visualize condyle, condylar neck, and upper part of ramus simultaneously and to avoid diagnostic pitfall. Placement of the USG probe far posterior to this line will show condylar curvature and ramus only without condylar neck region on ultrasonic display due to anatomic curvature of condylar neck. This may lead to misdiagnosis as subcondylar fracture as there will be loss in continuity between condyle and ramus.
Figure 3.
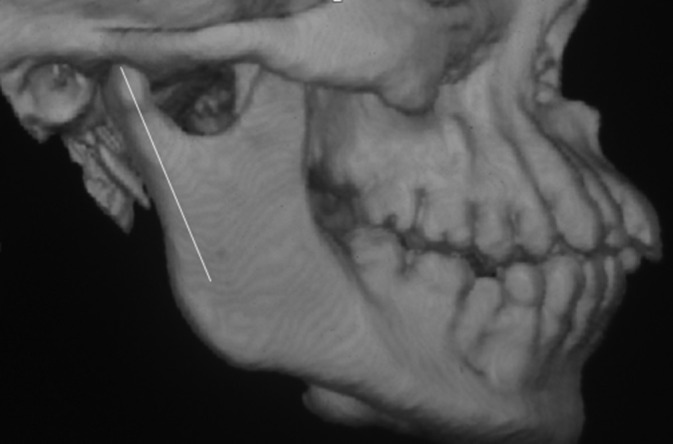
Imaginary line passing through condyle, condylar neck, and upper ramus where probe is to be placed
It was observed in 50% (20) of the cases, that USG was able to show not only the discontinuity in the cortical bone, but also the fashion in which the discontinuity was progressing deeper into the marrow portion of the bone. Oblique fractures were demonstrated in some cases of zygomatic arch and mandibular fractures especially in outer half of the involved bone. The intervening tissues between the probe and the bone; and the density of the bone may play a role in the ability of the sound waves to give details of deeper portions of the bone.
Overall sensitivity, specificity, positive predictive value, and negative predictive values of conventional radiography and USG in diagnosing zygomatic arch and mandibular fractures were calculated with CT as reference in this study and were found to be 97.4%, 100%, 100%, and 66.7%, respectively. This data shows equal reliability of conventional radiography and USG in diagnosing zygomatic arch and mandibular fractures, but their reliabilities are lesser than CT.”
There are factors affecting the validity of diagnostic USG in maxillofacial fractures. These include the experience of the sonographer and the type and resolution of the transducer. The use of regular linear probes leads to problems with poor adaptation to facial topography; some investigators overcome this by using curvilinear and small size probes. Specially designed transducers suited to maxillofacial topography are desirable.[8]
Conclusion
Ultrasonography is a very rapid, cost-effective, and radiation free imaging technique for detection of superficially situated bone fracture such as zygomatic arch and mandibular fractures. It may be used for screening for fracture of superficial bones. USG can replace conventional radiography in cases of isolated uncomplicated fractures. In cases of doubtful fracture, combination of USG and conventional plain films may be considered to avoid unnecessary exposures from higher imaging like CT scan. It can be considered as the imaging of choice when CT or conventional radiography are not advised as in pregnant women.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Stanley RB., Jr The zygomatic arch as a guide to reconstruction of comminuted malar fractures. Arch Otolaryngol Head Neck Surg. 1989;115:1459–62. doi: 10.1001/archotol.1989.01860360061018. [DOI] [PubMed] [Google Scholar]
- 2.Lauria L, Curi MM, Chammas MC, Pinto DS, Torloni H. Ultrasonography evaluation of bone lesions of the jaw. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1996;82:351–7. doi: 10.1016/s1079-2104(96)80365-9. [DOI] [PubMed] [Google Scholar]
- 3.Koischwitz D, Gritzmann N. Ultrasound of the neck. Radiol Clin North Am. 2000;38:1029–45. doi: 10.1016/s0033-8389(05)70219-0. [DOI] [PubMed] [Google Scholar]
- 4.Akizuki H, Yoshida H, Michi K. Ultrasonographic evaluation during reduction of zygomatic arch fractures. J Craniomaxillofac Surg. 1990;18:263–6. doi: 10.1016/s1010-5182(05)80428-7. [DOI] [PubMed] [Google Scholar]
- 5.Ord RA, Le May M, Duncan JG, Moos KF. Computerized tomography and B-scan ultrasonography in the diagnosis of fractures of the medial orbital wall. Plast Reconstr Surg. 1981;67:281–8. doi: 10.1097/00006534-198103000-00001. [DOI] [PubMed] [Google Scholar]
- 6.Hübner U, Schlicht W, Outzen S, Barthel M, Halsband H. Ultrasound in the diagnosis of fractures in children. J Bone Joint Surg Br. 2000;82:1170–3. doi: 10.1302/0301-620x.82b8.10087. [DOI] [PubMed] [Google Scholar]
- 7.Hirai T, Manders EK, Nagamoto K, Saggers GC. Ultrasonic observation of facial bone fractures: Report of cases. J Oral Maxillofac Surg. 1996;54:776–9. doi: 10.1016/s0278-2391(96)90703-x. [DOI] [PubMed] [Google Scholar]
- 8.Adeyemo WL, Akadiri OA. A systematic review of the diagnostic role of ultrasonography in maxillofacial fractures. Int J Oral Maxillofac Surg. 2011;40:655–61. doi: 10.1016/j.ijom.2011.02.001. [DOI] [PubMed] [Google Scholar]