

Abstract
The patient was an 18-year-old female who had an Angle Class I malocclusion with a left palatally impacted maxillary canine. The orthodontic treatment of a palatally impacted canine is aimed at bringing the tooth into its correct position in the dental arch without causing any periodontal damage. To achieve this goal, a variety of surgical and orthodontic techniques have been proposed in relation to the position of the impacted tooth and there are various treatment methods used for traction. The duration of the traction was 3 months and alignment duration was 12 months the total treatment time was 15 months. In the following case, we presented that maxillary palatally impacted canine was brought into the arch with open window method for canine exposure and modified K-9 spring for traction, that is simple spring for orthodontic traction of the palatally impacted canines.
Keywords: Impacted maxillary canine, modified K-9 spring, open window method
Introduction
Maxillary canines are one of the most commonly impacted teeth after the third molars with prevalence in the range of 0.8-2.8%.[1] Maxillary canine impactions occur twice as often in females than in males in the ratio 2.3:1.[2,3] Majority of the canine impactions are palatal (85%).[4,5,6,7,8] It is also reported that only 8% of canine impactions are bilateral. If a maxillary permanent canine appears to be erupting ectopically or not at all, the extraction of the primary canine is recommended in the 10-13 age groups. In a vast majority of cases, extraction of deciduous canine improves the possibilities of eruption or at least changes to a more favorable position, which later improves the prognosis of the permanent canine, if surgical orthodontic guidance is needed.[9] Surgically assisted orthodontic guidance is required when a definite diagnosis of impaction has been made, and all possibilities of its natural eruption have been exhausted, it is done at least 6 months after complete root apex formation in most of the cases.[4] To achieve this goal, a variety of surgical and orthodontic techniques have been proposed in relation to the position of the impacted tooth and there are various treatment method used for traction. In the following case, we presented that maxillary palatally impacted canine was brought into the arch with open window method for surgical canine exposure and modified K-9 spring for the eruption of impacted canine.
Diagnosis
An 18-year-old female patient was referred with the unesthetic appearance of her missing maxillary anterior teeth. On clinical examination revealed that an Angle Class I molar relationship, and the permanent left canine was not seen in the arch [Figure 1a and b] Palatal bulge was identified in the maxillary left palatal region suggestive of the position of the impacted canine. The panoramic radiograph [Figure 1c] showed all permanent teeth including developing third molar buds and maxillary right canine. The left canine was mesially inclined toward the midline and was apparently overlapping the mesial aspect of the maxillary central incisor and impacted tooth lies sector IV in sector classification, angulation to the midline was 31° and distance from occlusion plane was 19 mm.
Figure 1.
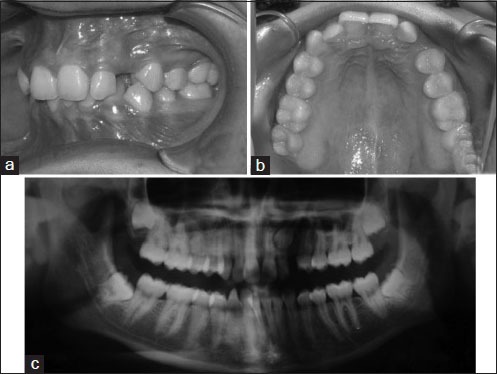
(a and b) Pretreatment photograph, (c) pretreatment orthopantomograph
Mechanism of Modified K-9 Spring [Figure 2c]
Figure 2.
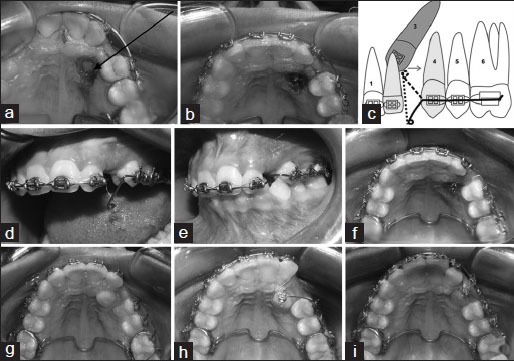
(a) Surgical exposure with open window technique, (b) lingual button bonded over exposed impacted left canine, (c) biomechanics of K-9 spring dotted horizontal arm indicates activation of K-9 spring, arrow indicates distal direction of force, (K-9 spring exerts eruptive force (70 g) and distal force on impacted canine). (d) K-9 spring in inactivated form, (e and f) K-9 spring in activated form, (g) canine erupts in oral cavity 3 months, (h) 014 Cu-nickel-titanium ligated for alignment of palatally impacted canine, (i) alignment in progress
The K-9 spring is made of 0.017 × 0.025 inch titanium molybdenum alloy* wire, it has two arms horizontal and vertical arm. The horizontal arm of the spring is inserted into the first molar buccal tube and the premolar brackets. About 8 mm (can vary according to the position of impacted canine) mesial to the first premolar bracket, the horizontal arm is bent 90° downward to form a vertical arm, which is about 9 mm long (according to distance of impacted canine from alveolar ridge) and ends in a helix [Figure 2d and e] and another bent is given toward palatal side. K-9 spring was ligated to buccal segment and impacted tooth and it provides a gentle extrusive force on the canine the spring also has a buccal component of force due to the arcial pattern of activation and deactivation. When the vertical arm of K-9 spring is rolled upward and inward to be engaged to an impacted palatal canine, the result is that reactive an intrusive force and clockwise moment on the molars and premolars. In general, transpalatal arch is used to control this reactive force and moment, but in most of the cases transpalatal arch fails to do so. Therefore, to minimize reactive force and moment we have put buccal crown torque in the premolar and molar region, and modification in the K-9 spring was done. Distallize force is achieved by cinch back of modified K-9 spring.[10]
Treatment Progress
Initially, molars of maxillary arch were banded and transpalatal arch was placed and all the other remaining teeth were bonded with 0.022 × 0.028 inch pre-adjusted-edge wise appliance. The surgical exposure done by creating a window [Figure 2a] that has been carried out by the oral surgeon in this stage and the attachment was bonded [Figure 2b]. The attachment was ligated to the modified K-9 spring and impacted tooth moves in vertical direction initially [Figure 2d–g]. As the impacted tooth moves vertically, the distal traction force applied by cinch back of modified K-9 spring. After that 0.014 inch Cu-nickel-titanium (NiTi) wire [Figure 2h and i] was ligated and progressively activated to maintain a force of 60-90 g. The bracket was bonded on the labial aspect of the canine was inverted to correct the torque and ligated to the auxiliary 0.016 inch NiTi wire and progressively increased to 0.019 × 0.025 inch stainless steel wire and subsequently, finishing was done.
Treatment Results
Overall, active treatment lasted for 15 months. There was a dramatic improvement in patient's smile. Canine guidance had been established bilaterally during lateral excursive movements. Posttreatment panoramic tracing on comparison with the pretreatment showed that the roots were well-angulated and aligned parallel, and path travelled by the impacted canine was 19 mm [Figure 3a–d].
Figure 3.
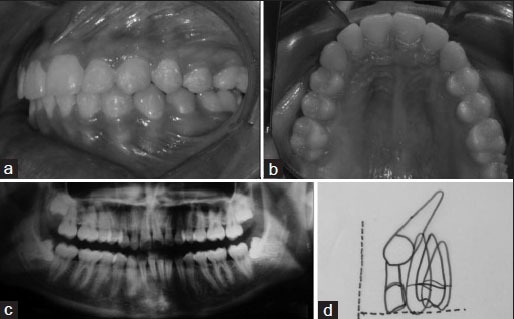
(a and b) Posttreatment intraoral photograph, (c) posttreatment orthopantomograph (OPG) (Treatment duration = 15 months), (d) superimposition of palatally impacted canine on OPG (path travelled by canine = 19 mm)
Discussion
According to the criteria put forth by Lindauer et al.,[1] the present case was diagnosed with a palatally impacted left canine. It consisted of the fact that root formation had been completed for both right and left canines. It is also noted that right canine has erupted for more than 6 months in the oral cavity without any signs of eruption of the left canine. Power and Short[6] predicted the chances of canine impaction based on calculating the angulation of the canine on an orthopantomograph; the angulation of the long axis of the canine to the midline may be monitored from the time root formation is one-third complete to 6 months after root completion, 10-13 years of age. If the tooth is angled more than 31° to the midline. If the crown was mesial to the midline of the lateral incisor root, spontaneous incisor eruption occurred in only 64% cases.[8] In the present case, the impacted maxillary canine was 31° to the midline in the pretreatment stage, which is in agreement with the criteria put forth by Power and Short[6] for successful canine disimpaction; also, the canine crown was distal to the midline of the lateral incisor in agreement with the criteria of Warford et al.[8] Graber and Vanarsdall[11,12] states that as the palate is all masticatory mucosa; therefore, graft is not placed on the tooth. To uncover a palatally impacted tooth, the palatal tissue is reflected, a window is placed and hence that vertical movement of impacted canine becomes easier. A periodontal dressing is kept in place for 7-10 days, and then a bonded attachment is placed and tooth movement is begun. This approach has been successfully used in the current case in terms of adequate attached gingival tissue preservation around the disimpacted canine. Goodsell[13] advocates that any tooth that has been surgically uncovered and is under orthodontic traction forces should be periodically checked for excessive mobility or bleeding from gingiva around the tooth. Care must be taken to ensure that periodontal attachment is following the tooth as it is guided into the arch. In the present case, the whole of the mucoperiosteum removed so that the tooth erupts into the oral cavity rapidly due to removal of barrier. Light force mechanics applied by modified K-9 spring[10] have been successfully used in the present case to bring the palatally impacted canine into the arch, and due to buccal crown torque in the premolar and molar region to minimize the intrusive force and clockwise moment and prevent any adverse effects and nonvitality of the adjacent teeth. Correction of torque, labio-palatal root angulation in basal bone, in the impacted canine tooth is important to achieve proper functional occlusion. This has been achieved successfully by the method advocated by McLaughlin et al.[14]
Conclusion
Treatment of impacted tooth is almost always a clinical challenge. By using open window for surgical exposure and modified K-9 spring for traction of impacted canine and minimize the side effect, decreases the treatment duration and improves periodontal health and functional occlusion for longterm results.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Lindauer SJ, Rubenstein LK, Hang WM, Andersen WC, Isaacson RJ. Canine impaction identified early with panoramic radiographs. J Am Dent Assoc. 1992;123:91. doi: 10.14219/jada.archive.1992.0069. [DOI] [PubMed] [Google Scholar]
- 2.Aydin U, Yilmaz HH, Yildirim D. Incidence of canine impaction and transmigration in a patient population. Dentomaxillofac Radiol. 2004;33:164–9. doi: 10.1259/dmfr/15470658. [DOI] [PubMed] [Google Scholar]
- 3.Shapira Y, Kuftinec MM. Early diagnosis and interception of potential maxillary canine impaction. J Am Dent Assoc. 1998;129:1450–4. doi: 10.14219/jada.archive.1998.0080. [DOI] [PubMed] [Google Scholar]
- 4.Coulter J, Richardson A. Normal eruption of the maxillary canine quantified in three dimensions. Eur J Orthod. 1997;19:171–83. doi: 10.1093/ejo/19.2.171. [DOI] [PubMed] [Google Scholar]
- 5.Kharbanda OP. 1st ed. Gurgaon: Elsevier; 2009. Orthodontics Diagnosis and Management of Malocclusion and Dentofacial Deformities; pp. 415–35. [Google Scholar]
- 6.Power SM, Short MB. An investigation into the response of palatally displaced canines to the removal of deciduous canines and an assessment of factors contributing to favourable eruption. Br J Orthod. 1993;20:215–23. doi: 10.1179/bjo.20.3.215. [DOI] [PubMed] [Google Scholar]
- 7.Becker A. 2nd ed. Jerusalem: Informa Healthcare; 2007. The Orthodontic Treatment of Impacted Teeth; pp. 29–52. (93-168). [Google Scholar]
- 8.Warford JH, Jr, Grandhi RK, Tira DE. Prediction of maxillary canine impaction using sectors and angular measurement. Am J Orthod Dentofacial Orthop. 2003;124:651–5. doi: 10.1016/s0889-5406(03)00621-8. [DOI] [PubMed] [Google Scholar]
- 9.Nagaraj K, Upadhyay M, Yadav S. Impacted maxillary central incisor, canine, and second molar with 2 supernumerary teeth and an odontoma. Am J Orthod Dentofacial Orthop. 2009;135:390–9. doi: 10.1016/j.ajodo.2006.12.023. [DOI] [PubMed] [Google Scholar]
- 10.Kalra V. The K-9 spring for alignment of impacted canines. J Clin Orthod. 2000;34:606–10. [PubMed] [Google Scholar]
- 11.Millet D, Welbury R. 1st ed. New York: Elsevier; 2005. Clinical Problem Solving in Orthodontics and Paediatric Dentistry; pp. 20–5. (90-3). 129-33. [Google Scholar]
- 12.Graber TM, Vanarsdall RL., Jr . 3rd ed. St. Louis: Mosby; 2000. Orthodontics Current Principles and Techniques; pp. 822–38. [Google Scholar]
- 13.Goodsell JF. Surgical exposure and orthodontic guidance of the impacted tooth. Dent Clin North Am. 1979;23:385–92. [PubMed] [Google Scholar]
- 14.McLaughlin R, Bennett C, Trevisi HJ. 1st ed. Barcelona, Spain: Mosby; 2002. Systemized Orthodontic Treatment Mechanics; pp. 55–70. [Google Scholar]