

Abstract
Objectives
Examine the reliability of sociodemographic variables in predicting initiation of breastfeeding within an hour of birth (EarlyBF), using data from 1998, 2003 and 2008–2009.
Study design
A replication analysis using the Kenya Demographic and Health Survey (KDHS) data collected in 1998, 2003 and 2008–2009. The candidate predictor variables were child's gender, home or health facility place of birth, vaginal or caesarean mode of birth, urban or rural setting, province of residence, Wealth Index and maternal education, occupation, literacy and media exposure.
Setting
Kenya.
Participants
6375 dyads of mothers aged 15–49 and their children aged 0–23 months (2125 dyads in each of the survey years).
Results
Mode of birth and province were statistically significant predictors of EarlyBF in 1998, 2003 and 2008–2009. Children delivered through caesarean section were non-EarlyBF in 1998 (OR 2.63, 95% CI 1.72 to 4.04), 2003 (OR 3.36, 95% CI 1.83 to 6.16) and 2008 (OR 3.51, 95% CI 2.17 to 5.69). The same was true of those living in the Western province in 1998 (OR 2.67, 95% CI 1.61 to 4.43), 2003 (OR 4.92, 95% CI 3.01 to 8.04) and 2008 (OR 6.07, 95% CI 3.54 to 10.39).
Conclusions
The 1998 KDHS data do not provide the basis for reliable prediction of EarlyBF, with reliability conceptualised as replicability of findings using highly similar data sets from 2003 and 2008–2009. Most of the demographic and socioeconomic variables were unreliable predictors of EarlyBF. We speculate that activities in parts or all of Kenya changed the analysis context in the period between 1998 and 2008–2009, and these changes were of a sufficient magnitude to affect the relationships under investigation. The degree to which this is a general problem in child health research is not known, calling for further research to investigate this methodological issue with other health end points and other data.
Keywords: PUBLIC HEALTH
Strengths and limitations of this study.
The usage of highly comparable nationally representative data from three time periods to study the reliability of sociodemographic variables in predicting the timing of initial breastfeeding after birth.
The elimination of most method-related explanations to explain lack of reliability in the findings.
The data available do not include possibly reliable predictors including measures of maternal childcare knowledge, attitudes, beliefs and values.
Introduction
Researchers and policymakers need reliable statistical models that describe the relationship of possible risk and protective factors to child feeding end points such as early initiation of breastfeeding (EarlyBF). A statistical model showing significant associations is reliable if it can be replicated with data other than the original data that were used to generate the model. A reliable model increases one's confidence in hypothesised risk and protective factors generated by observational research. A reliable model does not permit conclusions about causal relationships, but it does add impetus to further research to test hypotheses rigorously. The development of reliable models in which the early initiation of child breastfeeding (BF) is in focus is imperative, because this feeding behaviour has such profound consequences for the mother's and child's health. Yet the investigation of the reliability of statistical models is hampered by methodological problems and by the funders’ and researchers’ reluctance to invest money and effort in ‘mere’ replication research. This paper explains why this type of research is imperative and should have a high priority. We show how it can be carried out efficiently and cost effectively, using existing data on child health that are freely available to interested researchers.
Early initiation of BF
Among the highly recommended optimal infant and young child feeding practices is EarlyBF in accordance with which newborns should be put to breast within an hour of birth.1 2 Kenya is a signatory to this recommendation and has made efforts towards its actualisation.3 Nonetheless, over 40% of children in Kenya do not receive EarlyBF,4 making late initiation of BF an issue of significant public health concern. The failure to practise EarlyBF not only endangers the health and development of the newborns, but also the mother's health may be compromised, and mother–child bonding may be suboptimal.5 6 The multifaceted benefits of EarlyBF are so important, and the practice of early BF is so practical to implement, that EarlyBF is one of the most fundamental behaviours promoting child and maternal health. It is among the relatively few childcare behaviours that require no special training, equipment or facilities and in practice could be universal.7
The biomedical and psychosocial mechanisms linking EarlyBF to child health include the transmission of colostrum constituents, which are vital in boosting the neonate's immunity system. Colostrum contains antibodies that are transferred from the mother's mammary glands to the newborn's intestinal mucosa, exposing it to microbes that limit bacterial infection.8 The protective effect of colostrum works against common neonatal respiratory infections, otitis media and diarrhoea that are the major causes of childhood morbidity and mortality, especially in the developing world.9 EarlyBF also stimulates mother–infant bonding and makes a significant contribution to the cognitive development of the child.6
The skin-to-skin contact and suckling is understood to lessen the birth stress experienced by children and modulates the child's temperature, helping to prevent hypothermia and hypoglycaemia which can endanger the neonate's survival in the first week of life.10 11 This early contact, either through suckling of the breast or hand massage by the newborn, has benefits to the mother as it causes uterine involution, which in turn reduces postpartum haemorrhage, aids expulsion of the placenta and triggers early milk let-down.12 13 It is estimated that EarlyBF could reduce neonatal mortality by up to 22%.14 EarlyBF has also been linked to successful practice of other optimal BF behaviours, such as exclusive BF for 6 months, and longer BF duration after complementary foods are introduced.6 14 15
It may seem a puzzle why humans do not practise EarlyBF universally, as other BF mammals do. At least part of the answer is that the human instinct to breastfeed is tempered by social forces. The female breast is not just a milk delivery mechanism; “in the eyes of the beholder, babies see food, men see sex, physicians see disease, business sees dollar signs, religion sees spiritual symbols and psychoanalysis places them in the centre of the unconscious”.16 This clever citation makes a point that is captured more sombrely by a prominent health promotion model advanced by UNICEF more than two decades ago, as depicted in an adapted version in figure 1. Two main points are: (1) the chain of factors that influence childcare has origins in macrocontextual factors far removed from the control of mothers and their significant others and (2) the link between context and childcare is mediated by a host of maternal, household and community resources which may be more or less available. In child health research, the factors in the model have been operationalised in many ways. Using data from the Demographic and Health Surveys (DHS; which are not, however, intended primarily to test and develop a model), it is possible to specify variables at each level of the model, as shown in figure 1. The model is hierarchical; it is possible to conduct multivariate analyses hierarchically and to model the variance in childcare that is accounted for by the model's operationalised constructs. An array of studies have looked at the determinants of various optimal BF practices,15 17–22 but we are not aware of any that has looked at the reliability of these determinants over time.
Figure 1.
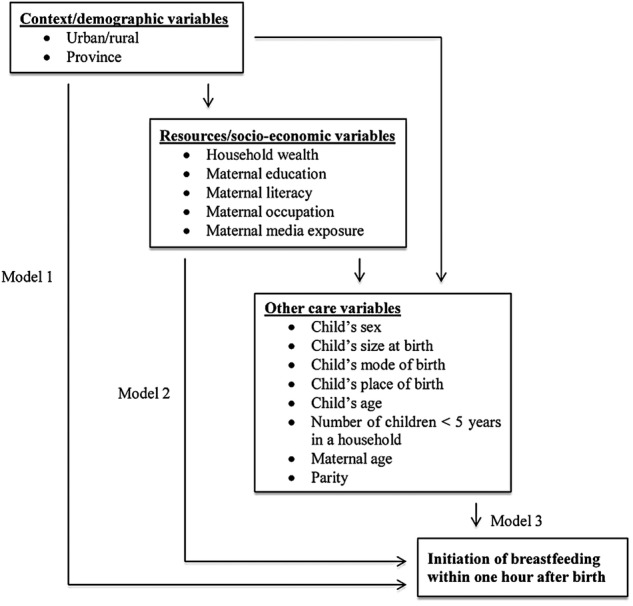
Analytical framework based on the UNICEF model (as extended by Engle et al23) for hierarchical regression analyses.
Analysis framework
The analytical framework for the models presented in this paper is an extended UNICEF model by Engle et al23 and Victora et al,24 further adapted and specified for this study as shown in figure 1. The limited aim of figure 1 is to organise the investigation of EarlyBF with attention to the possible predictor variables at several levels. The most distal level is the social, cultural, political and economic context, presented in the current analysis by just two indicators, urban/rural living conditions and province of residence. The intermediate level is household and household member resources, represented by several classical measures including household wealth and maternal education. The proximal level focuses on intrahousehold and community factors that may affect a mother's/family's ability to provide EarlyBF, such as mode and place of birth. For example, a vaginal home birth may be attended primarily by female relatives whose ideas about EarlyBF may have a powerful influence on a mother's behaviour, contra perhaps to what might be experienced in a hospital birth. The paths in figure 1 theorise partial mediation, an alternative to the original UNICEF model which is a fully mediated model. However, the UNICEF model is more of a conceptual framework than an analytical framework. There is no evidence in the literature as far as we are aware, nor any formally held theoretical position, that the distal, intermediate and proximal factors linked to child health are connected in a fully mediated manner. It is an empirical question if this is so, and tests of the three models are needed to provide evidence on the matter.
This health promotion framework is distinct from health behaviour change models that focus on psychological factors related to behaviour change, such as the Theory of Reasoned Action or the Health Belief Model. The extended UNICEF conceptual framework focuses both on macro contextual factors and on the resources needed to support good childcare, leading to good child health. The type of care given to a child (EarlyBF) is subject to availability and accessibility of resources at a household level and the support accorded to the caregiver at the family and community levels. Thus, the overarching framework for this study places emphasis on health promotion and resources for health, rather than on disease prevention and a risk factor orientation.
Replication analysis
Replication analysis is a form of scientific validation that examines the reliability of statistical models across data sets.25 It provides a means of distinguishing the effect of sampling differences from (1) measurement variation and/or (2) statistical model instability, by attempting the replication of an analysis of a common set of measures across different samples of known characteristics. The replication analysis confirms the robustness of the relationships in a statistical model developed with one data set by testing the model with other data sets. In survey research, the general form of this type of analysis is termed ‘retest replication’, the distinguishing feature of which is to repeat an original study with few if any significant changes in the research design.26 In Lindsay and Ehrenberg's27 theory of replication, the general form of this analysis is a ‘close replication’, compared to a ‘differentiated replication’, which extends the range of conditions being studied. In Tsang and Kwan's28 replication typology, this form of analysis is labelled ‘empirical generalisation’, the use of the same measurement and analysis with data from different populations. This is distinct from replication analysis in which cross-validation, jack-knife and bootstrap methods can be used to examine replicability when only one sample is available.29
Replication analysis is rarely undertaken, even if replicability is in the abstract a highly regarded quality criterion in the positivist tradition.30 Studies of replicability are not in fact prioritised and they have always been difficult to publish across the wide range of social sciences that contribute to public health research.27 31 32 At the statistical level, researchers are encouraged to focus on the analysis of a single study, not the coordinated analysis of multiple data sets with the aim of studying replicability.27 This is not to be confused with meta-analysis, which analyses effects across similar studies that were not undertaken with replication as a main goal. When the study of replicability is a goal, it is difficult to undertake. Most research reports do not contain enough information to allow high fidelity replication, and studies of the same phenomena often measure constructs in different ways. Measurement variation can have many causes, among the most obvious of which are differences in how the measurement of a construct is operationalised. Measurement variation complicates not only replication analysis, but also other forms of comparative studies such as systematic reviews.33
When replication analysis is to be undertaken, several strategies are available: replication of methodology, of analyses and of statistical models. Graves used common methodology to compare the relationship between infant nutrition and behaviour in Nepal with earlier findings from West Bengal.34 The comparison of the two studies was undertaken in the Discussion section of the paper, which otherwise focused only on the analysis and interpretation of the data from Nepal. In contrast, Miller et al25 investigated the replicability of regression analyses relating caregiver distress to social support and stressors in four data sets. They carried out four analyses separately within data sets, and compared results across data sets for consistency. The comparison of the analysis was undertaken in the Results as well as the Discussion sections of the paper. An alternative approach that is somewhat more stringent is to develop a statistical model with one data set and test the replicability of precisely that model with other data.
Study aim
The aim of this study was to undertake a replication analysis using the 1998, 2003 and 2008–2009 DHS data sets. The objective was to examine the reliability of demographic and socioeconomic (SES) variables in predicting EarlyBF, by comparing analyses of three highly similar yet independent data sets from 1998, 2003 and 2008–2009.
Methods
Data
The study used data from the Kenya Demographic and Health Survey (KDHS), a nationally representative cross-sectional survey project conducted in 1998, 2003 and 2008–2009. Periods of data collection for the 1998, 2003 and 2008–2009 surveys varied, starting from February to July 1998, April to September 2003 and November 2008 to February 2009, respectively.4 35 36 These cross-sectional surveys are among a series of DHS conducted in developing countries through the MEASURE DHS programme aimed at assisting developing countries in collecting data on fertility, family planning and maternal and child health.4 35 36 The data sets are public and required no further ethical clearance for use in this paper.37
The KDHS is a household based survey that uses a multistage sampling procedure. The first stage uses the master sampling frames maintained by the Kenya National Bureau of Statistics to select data collection points, also referred to as clusters or sample units. A total of 536, 400 and 400 clusters were selected in 1998, 2003 and 2008–2009, respectively. In the second stage, households were systematically selected from clusters with eligible women in the households interviewed. A total of 7881, 8195 and 8444 women aged 15–49 years were successfully interviewed in 1998, 2003 and 2008–2009, respectively, with a response rate of over 94% across the three surveys. The KDHS sampling design calls for the use of sampling weights.38
Data used in the present study were selected from the data described above. The starting point was to select all children aged 0–23 months in the 2008–2009 data (n=2125), the survey in which the fewest children participated. Same-sized samples of children were then selected at random from the 1998 and 2003 data sets using the Statistical Package for Social Sciences (SPSS) random selection procedure. The data associated with each child were collected from its mother in a household.
Analysis
The dependent variable Early BF was coded zero if the mother initiated BF within an hour of birth and one if BF was initiated later. Independent continuous variables were child's age, birth order, mother's age and number of children in a household aged 5 years and below. Independent categorical variables were:
Child's sex;
Mother's perceived child's size at birth (small, medium or large);
Child's place of birth (home or health facility);
Mode of child's birth (vaginal or caesarean section);
Province (Nairobi, Central, Coast, Eastern, Nyanza, Rift Valley and Western);
Residence (urban or rural);
Wealth Index (richest, richer, middle, poorer or poorest);
Maternal education (completed secondary and/or higher education, incomplete secondary, complete primary, incomplete primary or no education);
Maternal occupation (white collar, blue collar or not working);
Maternal literacy (reads easily, reads with difficulty or cannot read);
Maternal weekly exposure to media (read newspaper at least once a week or not, watched television at least once a week or not and listened to radio at least once a week or not).
The North-Eastern province was excluded from the analysis because KDHS did not collect data in this province in 1998.35 The Wealth Index measures household assets.39
Statistical analysis was carried out using SPSS V.19. SPSS’ complex samples module was used to account for the multistage sampling strategy through weighting and controlling for the primary sampling unit (clusters) and sample domain (strata) in all the analyses. Logistic regression was employed to determine the net effects of each independent variable in the regression model for each survey year. As illustrated in figure 1, the study's statistical models first examined the associations of the outcome variable with the context variables (model 1), followed by the associations of resource variables adjusted for the context (model 2), and lastly the associations of other potential care determinants (eg, child's age) adjusted for context and resources (model 3).
Results
Description of samples
The average age of children was 12 months in 1998, 11 months in 2003 and 11 months in 2008–2009, while that for mothers interviewed was 27 years across the three surveys. On average, households in all the three surveys had two children aged below 5 years of age. Maternal parity averaged four births in 1998 and three births in 2003 and 2008–2009. Table 1 summarises the national sample size distribution for timing of initiation of BF after birth and subgroup samples from 1998 to 2008–2009.
Table 1.
Characteristics of the samples by outcome and potential predictor variables included in logistic regression analyses
| Variables | KDHS 1998 |
KDHS 2003 |
KDHS 2008–2009 |
|||
|---|---|---|---|---|---|---|
| n | Per cent | n | Per cent | n | Per cent | |
| Total sample | 2125 | 100.0 | 2125 | 100.0 | 2125 | 100.0 |
| Initiation of breastfeeding | ||||||
| Within 1 h after birth | 1024 | 54.5 | 988 | 48.7 | 1156 | 54.9 |
| Later than 1 h after birth | 892 | 45.5 | 1129 | 51.3 | 948 | 45.1 |
| Sex | ||||||
| Girls | 973 | 45.3 | 802 | 37.3 | 783 | 37.2 |
| Boys | 1152 | 54.7 | 1323 | 62.7 | 1342 | 62.8 |
| Child’s place of birth | ||||||
| Health facility | 827 | 42.7 | 918 | 41.2 | 1013 | 46.1 |
| Home | 1292 | 57.3 | 1203 | 58.8 | 1106 | 53.9 |
| Mode of birth | ||||||
| Vaginal | 1780 | 92.3 | 2024 | 95.9 | 1963 | 92.6 |
| Caesarean section | 137 | 7.7 | 100 | 4.1 | 162 | 7.4 |
| Child’s size at birth | ||||||
| Large | 406 | 21.3 | 557 | 27.1 | 677 | 31.9 |
| Average | 1353 | 62.1 | 1219 | 57.3 | 1118 | 52.5 |
| Small | 353 | 16.6 | 341 | 15.6 | 307 | 15.6 |
| Province | ||||||
| Nairobi | 83 | 7.3 | 188 | 6.1 | 160 | 5.8 |
| Central | 178 | 9.3 | 277 | 10.8 | 166 | 7.2 |
| Coast | 323 | 8.0 | 285 | 9.2 | 357 | 9.8 |
| Eastern | 285 | 16.5 | 275 | 16.2 | 300 | 15.4 |
| Nyanza | 358 | 21.2 | 285 | 15.4 | 432 | 20.1 |
| Rift Valley | 617 | 25.1 | 493 | 29.1 | 414 | 30.2 |
| Western | 281 | 12.6 | 322 | 13.2 | 296 | 11.5 |
| Residence | ||||||
| Urban | 340 | 20.0 | 527 | 18.5 | 554 | 19.9 |
| Rural | 1785 | 80.0 | 1598 | 81.5 | 1571 | 80.1 |
| Maternal education | ||||||
| Secondary+ | 313 | 16.0 | 303 | 12.4 | 354 | 16.4 |
| Incomplete secondary | 209 | 10.4 | 192 | 9.0 | 178 | 8.9 |
| Complete primary | 557 | 25.5 | 582 | 28.2 | 587 | 31.4 |
| Incomplete primary | 819 | 38.5 | 753 | 37.5 | 715 | 33.3 |
| No education | 227 | 9.5 | 295 | 12.9 | 291 | 10.1 |
| Wealth index | ||||||
| Richest | 341 | 18.7 | 479 | 18.8 | 483 | 19.6 |
| Richer | 402 | 18.2 | 358 | 17.4 | 380 | 19.0 |
| Middle | 417 | 19.4 | 400 | 19.0 | 344 | 18.3 |
| Poorer | 468 | 20.5 | 412 | 21.1 | 392 | 20.3 |
| Poorest | 497 | 23.2 | 476 | 23.7 | 526 | 22.8 |
| Maternal occupation | ||||||
| White collar | 393 | 20.5 | 382 | 17.1 | 553 | 25.6 |
| Blue collar | 734 | 35.7 | 916 | 45.6 | 626 | 33.0 |
| Not working | 995 | 43.8 | 825 | 37.3 | 942 | 41.4 |
| Maternal literacy | ||||||
| Reads easily | 1280 | 61.3 | 1453 | 68.5 | 1383 | 69.3 |
| Reads with difficulty | 499 | 23.7 | 163 | 8.4 | 298 | 14.0 |
| Cannot read | 339 | 15.1 | 502 | 23.1 | 426 | 16.2 |
| Mother reads newspaper | ||||||
| Yes | 665 | 32.9 | 728 | 32.8 | 752 | 36.8 |
| No | 1457 | 67.1 | 1393 | 67.2 | 1368 | 63.2 |
| Mother watches television | ||||||
| Yes | 417 | 21.0 | 611 | 27.1 | 781 | 36.5 |
| No | 1690 | 79.0 | 1513 | 72.9 | 1344 | 63.5 |
| Mother listens to radio | ||||||
| Yes | 1206 | 56.6 | 1763 | 82.7 | 1735 | 85.1 |
| No | 910 | 43.4 | 362 | 17.3 | 389 | 14.9 |
Secondary+, complete secondary and/or higher education.
KDHS, Kenya Demographic and Health Survey.
Logistic regression results
Examining the tables showing the results of logistic regression, there are two patterns of reliability that can be discerned: a finding of no significant association across all surveys, or a finding that all associations are significant across all surveys. Here we comment only on the latter expression of reliability. Model 1, shown in table 2, examines the 1998, 2003 and 2008–2009 unadjusted associations of the context variables urban–rural residence and province with EarlyBF. The odds of non-EarlyBF were significantly greater than 1:1 in the Nyanza and Coast provinces compared to the Eastern province in all three surveys. All other year-by-year comparisons failed to support the reliability hypothesis, and thus these analyses present mixed evidence for the reliability of these contextual variables as correlates of EarlyBF.
Table 2.
Unadjusted logistic regression models with context variables as predictors of EarlyBF
| Variables | KDHS 1998 |
KDHS 2003 |
KDHS 2008–2009 |
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | OR | 95% CI | Significance (p value) | β | OR | 95% CI | Significance (p value) | β | OR | 95% CI | Significance (p value) | |
| Residence | 0.012 | 0.602 | 0.072 | |||||||||
| Urban (reference) | ||||||||||||
| Rural | 0.503 | 1.65 | 1.12 to 2.44 | −0.095 | 0.91 | 0.64 to 1.30 | −0.394 | 0.67 | 0.44 to 1.04 | |||
| Province | 0.000 | 0.000 | 0.000 | |||||||||
| Eastern (reference) | ||||||||||||
| Nyanza | 0.952 | 2.59 | 1.67 to 4.02 | 0.514 | 1.67 | 1.06 to 2.64 | 0.292 | 1.34 | 0.82 to 2.19 | |||
| Western | 0.883 | 2.42 | 1.50 to 3.90 | 1.552 | 4.72 | 2.96 to 7.55 | 1.675 | 5.34 | 3.22 to 8.84 | |||
| Central | −0.307 | 0.74 | 0.44 to 1.23 | −0.010 | 0.99 | 0.65 to 1.51 | 0.910 | 2.48 | 1.48 to 4.18 | |||
| Rift Valley | −0.116 | 0.89 | 0.57 to 1.40 | −0.037 | 0.96 | 0.63 to 1.47 | 0.342 | 1.41 | 0.80 to 2.49 | |||
| Nairobi | 0.761 | 2.14 | 1.08 to 4.24 | 0.259 | 1.30 | 0.72 to 2.33 | 0.128 | 1.14 | 0.57 to 2.27 | |||
| Coast | 0.854 | 2.35 | 1.45 to 3.80 | 1.848 | 6.35 | 3.29 to 12.26 | 1.432 | 4.19 | 2.20 to 7.98 | |||
| r2=0.060 | r2=0.095 | r2=0.078 | ||||||||||
EarlyBF, early initiation of breastfeeding; KDHS, Kenya Demographic and Health Survey; r2, Cox and Snell pseudo r2.
The effects of resource variables adjusted for the possible confounding role of context are examined in table 3. In the presence of the resource variables, the relationships of the context variables to early BF did not differ markedly from the findings in table 2. For maternal education, the sole finding was of increased risk of non-EarlyBF among mothers with incomplete primary education, compared to those with secondary or higher education in 2003 and 2008–2009. None of the other resource variables exhibited reliable statistically significant associations with EarlyBF.
Table 3.
Adjusted logistic regression model with context and resource variables as predictors of EarlyBF
| Variables | KDHS 1998 |
KDHS 2003 |
KDHS 2008–2009 |
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | OR | 95% CI | Significance (p value) | β | OR | 95% CI | Significance (p value) | β | OR | 95% CI | Significance (p value) | |
| Residence | 0.052 | 0.583 | 0.124 | |||||||||
| Urban (reference) | ||||||||||||
| Rural | 0.411 | 1.51 | 1.00 to 2.29 | 0.109 | 1.12 | 0.76 to 1.65 | −0.404 | 0.67 | 0.40 to 1.12 | |||
| Province | 0.000 | 0.000 | 0.000 | |||||||||
| Eastern (reference) | ||||||||||||
| Nyanza | 0.874 | 2.40 | 1.55 to 3.71 | 0.485 | 1.63 | 1.03 to 2.57 | 0.310 | 1.36 | 0.83 to 2.23 | |||
| Western | 0.956 | 2.60 | 1.58 to 4.28 | 1.575 | 4.83 | 3.02 to 7.73 | 1.824 | 6.20 | 3.68 to 10.43 | |||
| Central | −0.302 | 0.74 | 0.44 to 1.26 | −0.018 | 0.98 | 0.64 to 1.51 | 1.013 | 2.75 | 1.61 to 4.71 | |||
| Rift Valley | −0.126 | 0.88 | 0.56 to 1.38 | 0.023 | 1.02 | 0.68 to 1.54 | 0.423 | 1.53 | 0.83 to 2.79 | |||
| Nairobi | 0.674 | 1.96 | 0.95 to 4.04 | 0.225 | 1.25 | 0.69 to 2.28 | 0.288 | 1.33 | 0.67 to 2.67 | |||
| Coast | 0.842 | 2.32 | 1.37 to 3.95 | 2.016 | 7.51 | 3.92 to 14.37 | 1.430 | 4.18 | 2.16 to 8.07 | |||
| Wealth Index | 0.206 | 0.761 | 0.945 | |||||||||
| Richest (reference) | ||||||||||||
| Richer | −0.125 | 0.88 | 0.55 to 1.41 | −0.218 | 0.80 | 0.54 to 1.19 | −0.137 | 0.87 | 0.51 to 1.48 | |||
| Middle | −0.166 | 0.85 | 0.52 to 1.38 | −0.282 | 0.75 | 0.48 to 1.18 | −0.062 | 0.94 | 0.52 to 1.71 | |||
| Poorer | 0.206 | 1.23 | 0.75 to 2.03 | −0.241 | 0.79 | 0.51 to 1.22 | −0.108 | 0.90 | 0.50 to 1.62 | |||
| Poorest | 0.072 | 1.07 | 0.63 to 1.82 | −0.173 | 0.84 | 0.53 to 1.35 | 0.013 | 1.01 | 0.55 to 1.86 | |||
| Maternal education | 0.141 | 0.011 | 0.003 | |||||||||
| Secondary+ (reference) | ||||||||||||
| Incomplete secondary | 0.586 | 1.80 | 1.08 to 2.98 | 0.410 | 1.51 | 0.95 to 2.40 | 0.245 | 1.28 | 0.72 to 2.28 | |||
| Complete primary | 0.369 | 1.45 | 0.96 to 2.19 | 0.340 | 1.41 | 0.97 to 2.04 | 0.324 | 1.38 | 0.86 to 2.24 | |||
| Incomplete primary | 0.484 | 1.62 | 1.07 to 2.46 | 0.611 | 1.84 | 1.24 to 2.74 | 0.786 | 2.19 | 1.37 to 3.52 | |||
| No education | 0.548 | 1.73 | 0.92 to 3.25 | 0.122 | 1.13 | 0.57 to 2.24 | 0.428 | 1.53 | 0.70 to 3.36 | |||
| Maternal literacy | 0.106 | 0.924 | 0.045 | |||||||||
| Reads easily (reference) | ||||||||||||
| Reads with difficulty | −0.243 | 0.63 | 0.38 to 1.05 | −0.072 | 0.93 | 0.61 to 1.43 | −0.386 | 0.68 | 0.44 to 1.05 | |||
| Cannot read | −0.459 | 0.78 | 0.59 to 1.05 | −0.064 | 0.94 | 0.62 to 1.42 | 0.225 | 1.25 | 0.82 to 1.91 | |||
| Maternal occupation | 0.517 | 0.865 | 0.085 | |||||||||
| White collar (reference) | ||||||||||||
| Blue collar | 0.180 | 1.20 | 0.85 to 1.68 | 0.059 | 1.06 | 0.77 to 1.46 | 0.360 | 1.43 | 0.95 to 2.16 | |||
| Not working | 0.164 | 1.18 | 0.87 to 1.61 | 0.087 | 1.09 | 0.79 to 1.50 | 0.468 | 1.60 | 1.06 to 2.41 | |||
| Mother reads newspaper | 0.313 | 0.043 | 0.058 | |||||||||
| Yes (reference) | ||||||||||||
| No | −0.140 | 0.87 | 0.66 to 1.14 | −0.271 | 0.76 | 0.59 to 0.99 | −0.309 | 0.73 | 0.53 to 1.01 | |||
| Mother watches TV | 0.262 | 0.408 | 0.314 | |||||||||
| Yes (reference) | ||||||||||||
| No | −0.203 | 0.82 | 0.57 to 1.16 | −0.109 | 0.90 | 0.69 to 1.16 | −0.170 | 0.84 | 0.61 to 1.18 | |||
| Mother listens to radio | 0.047 | 0.210 | 0.054 | |||||||||
| Yes (reference) | ||||||||||||
| No | 0.211 | 1.24 | 1.00 to 1.52 | −0.206 | 0.81 | 0.59 to 1.12 | −0.375 | 0.69 | 0.47 to 1.01 | |||
| r2=0.075 | r2=0.110 | r2=0.106 | ||||||||||
EarlyBF, early initiation of breastfeeding; KDHS, Kenya Demographic and Health Survey; r2, Cox and Snell pseudo r2; Secondary+, complete secondary and/or higher education; TV, television.
Model 3 results are shown in table 4. This examines the effects of other care determinants adjusted for the confounding roles of context and resources. Only two variables were reliably related to EarlyBF, province and mode of birth. As in model 1, the odds of non-EarlyBF were significantly greater than 1:1 in the Western and Coast provinces compared to the Eastern province in all three surveys. This indicates an effect that is not accounted for by other variables in the analysis. Furthermore, the magnitudes of the ORs for the Western and Coast provinces were similar in models 1 and 4, which is another sign of reliability. Regarding the mode of birth, the odds of non-EarlyBF were significantly greater than 1:1 for children delivered via caesarean section compared to those having vaginal births for all three surveys. An examination of the ORs and the CIs for the mode of birth findings shows substantial uniformity from survey to survey.
Table 4.
Adjusted logistic regression models with context, resource and other care determinants as predictors of EarlyBF
| Variables | KDHS 1998 |
KDHS 2003 |
KDHS 2008–2009 |
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | OR | 95% CI | Significance (p value) | β | OR | 95% CI | Significance (p value) | β | OR | 95% CI | Significance (p value) | |
| Residence | 0.083 | 0.871 | 0.120 | |||||||||
| Urban (reference) | ||||||||||||
| Rural | 0.390 | 1.48 | 0.95 to 2.30 | 0.035 | 1.04 | 0.68 to 1.58 | −0.430 | 0.65 | 0.38 to 1.12 | |||
| Province | 0.000 | 0.000 | 0.000 | |||||||||
| Eastern (reference) | ||||||||||||
| Nyanza | 0.914 | 2.50 | 1.60 to 3.90 | 0.522 | 1.69 | 1.04 to 2.75 | 0.316 | 1.37 | 0.81 to 2.31 | |||
| Western | 0.983 | 2.67 | 1.61 to 4.43 | 1.593 | 4.92 | 3.01 to 8.04 | 1.803 | 6.07 | 3.54 to 10.39 | |||
| Central | −0.277 | 0.76 | 0.44 to 1.30 | −0.049 | 0.95 | 0.61 to 1.48 | 1.036 | 2.82 | 1.61 to 4.92 | |||
| Rift Valley | −0.167 | 0.85 | 0.54 to 1.33 | 0.003 | 1.00 | 0.66 to 1.53 | 0.399 | 1.49 | 0.79 to 2.81 | |||
| Nairobi | 0.702 | 2.02 | 0.98 to 4.14 | 0.169 | 1.18 | 0.63 to 2.23 | 0.292 | 1.34 | 0.64 to 2.80 | |||
| Coast | 0.800 | 2.23 | 1.31 to 3.79 | 2.031 | 7.62 | 3.90 to 14.90 | 1.519 | 4.57 | 2.30 to 9.05 | |||
| Wealth Index | 0.200 | 0.907 | 0.907 | |||||||||
| Richest (reference) | ||||||||||||
| Richer | −0.155 | 0.86 | 0.53 to 1.37 | −0.135 | 0.87 | 0.57 to 1.34 | −0.146 | 0.87 | 0.50 to 1.50 | |||
| Middle | −0.134 | 0.88 | 0.54 to 1.43 | −0.201 | 0.82 | 0.51 to 1.31 | 0.003 | 1.00 | 0.53 to 1.91 | |||
| Poorer | 0.222 | 1.25 | 0.74 to 2.10 | −0.209 | 0.81 | 0.51 to 1.30 | −0.110 | 0.90 | 0.47 to 1.70 | |||
| Poorest | 0.104 | 1.11 | 0.65 to 1.90 | −0.110 | 0.90 | 0.54 to 1.48 | 0.011 | 1.01 | 0.53 to 1.95 | |||
| Maternal education | 0.163 | 0.024 | 0.003 | |||||||||
| Secondary+ (reference) | ||||||||||||
| Incomplete secondary | 0.625 | 1.87 | 1.10 to 3.17 | 0.481 | 1.62 | 0.97 to 2.69 | 0.243 | 1.28 | 0.70 to 2.33 | |||
| Complete primary | 0.359 | 1.43 | 0.92 to 2.23 | 0.377 | 1.46 | 0.96 to 2.22 | 0.353 | 1.42 | 0.87 to 2.33 | |||
| Incomplete primary | 0.449 | 1.57 | 1.00 to 2.45 | 0.626 | 1.87 | 1.19 to 2.95 | 0.838 | 2.31 | 1.43 to 3.75 | |||
| No education | 0.604 | 1.83 | 0.94 to 3.56 | 0.144 | 1.16 | 0.56 to 2.41 | 0.531 | 1.70 | 0.77 to 3.75 | |||
| Maternal literacy | 0.117 | 0.937 | 0.031 | |||||||||
| Reads easily (reference) | ||||||||||||
| Reads with difficulty | −0.236 | 0.79 | 0.59 to 1.06 | −0.053 | 0.95 | 0.62 to 1.46 | −0.418 | 0.66 | 0.42 to 1.04 | |||
| Cannot read | −0.473 | 0.62 | 0.37 to 1.06 | −0.071 | 0.93 | 0.61 to 1.43 | 0.259 | 1.30 | 0.82 to 2.06 | |||
| Maternal occupation | 0.609 | 0.769 | 0.103 | |||||||||
| White collar (reference) | ||||||||||||
| Blue collar | 0.126 | 1.13 | 0.80 to 1.61 | 0.083 | 1.09 | 0.79 to 1.50 | 0.384 | 1.47 | 0.98 to 2.20 | |||
| Not working | 0.158 | 1.17 | 0.86 to 1.60 | 0.121 | 1.13 | 0.81 to 1.57 | 0.453 | 1.57 | 1.03 to 2.42 | |||
| Mother reads newspaper | 0.238 | 0.065 | 0.053 | |||||||||
| Yes (reference) | ||||||||||||
| No | −0.167 | 0.85 | 0.64 to 1.12 | −0.255 | 0.78 | 0.59 to 1.02 | −0.325 | 0.72 | 0.52 to 1.00 | |||
| Mother watches TV | 0.211 | 0.289 | 0.287 | |||||||||
| Yes (reference) | ||||||||||||
| No | −0.232 | 0.79 | 0.55 to 1.14 | −0.141 | 0.87 | 0.67 to 1.13 | −0.189 | 0.83 | 0.58 to 1.17 | |||
| Mother listens to radio | 0.106 | 0.195 | 0.041 | |||||||||
| Yes (reference) | ||||||||||||
| No | 0.181 | 1.20 | 0.96 to 1.49 | −0.217 | 0.81 | 0.58 to 1.12 | −0.421 | 0.66 | 0.44 to 0.98 | |||
| Sex | 0.964 | 0.015 | 0.513 | |||||||||
| Girls (reference) | ||||||||||||
| Boys | −0.005 | 1.00 | 0.81 to 1.23 | 0.225 | 1.25 | 1.05 to 1.50 | −0.079 | 0.92 | 0.73 to 1.17 | |||
| Child's size at birth | 0.036 | 0.091 | 0.014 | |||||||||
| Large (reference) | ||||||||||||
| Average | −0.041 | 0.96 | 0.73 to 1.26 | −0.265 | 0.77 | 0.59 to 1.00 | −0.285 | 0.75 | 0.57 to 1.00 | |||
| Small | 0.381 | 1.46 | 1.02 to 2.10 | −0.035 | 0.97 | 0.70 to 1.33 | 0.193 | 1.21 | 0.82 to 1.79 | |||
| Mode of birth | 0.000 | 0.000 | 0.000 | |||||||||
| Vaginal (reference) | ||||||||||||
| Caesarean section | 0.968 | 2.63 | 1.72 to 4.04 | 1.212 | 3.36 | 1.83 to 6.16 | 1.255 | 3.51 | 2.17 to 5.69 | |||
| Place of birth | 0.013 | 0.193 | 0.001 | |||||||||
| Health facility (reference) | ||||||||||||
| Home | 0.341 | 1.41 | 1.08 to 1.84 | 0.187 | 1.21 | 0.91 to 1.60 | 0.492 | 1.64 | 1.21 to 2.21 | |||
| Child’s age (months) | −0.008 | 0.99 | 0.98 to 1.01 | 0.340 | −0.004 | 1.00 | 0.98 to 1.01 | 0.573 | −0.007 | 0.99 | 0.98 to 1.01 | 0.370 |
| No of children aged <5 years | −0.150 | 0.86 | 0.76 to 0.97 | 0.016 | −0.013 | 0.99 | 0.87 to 1.12 | 0.844 | 0.018 | 1.02 | 0.88 to 1.18 | 0.812 |
| Maternal age (years) | −0.016 | 0.98 | 0.96 to 1.01 | 0.294 | 0.004 | 1.00 | 0.97 to 1.04 | 0.787 | −0.002 | 1.00 | 0.96 to 1.04 | 0.921 |
| Parity | 0.040 | 1.04 | 0.95 to 1.14 | 0.375 | −0.016 | 0.98 | 0.89 to 1.09 | 0.749 | −0.093 | 0.91 | 0.80 to 1.04 | 0.172 |
| r2=0.096 | r2=0.125 | r2=0.144 | ||||||||||
EarlyBF, early initiation of breastfeeding; KDHS, Kenya Demographic and Health Survey; r2, Cox and Snell pseudo r2; Secondary+, complete secondary and/or higher education; TV, television.
Discussion
Only province and child's mode of birth were reliably associated with EarlyBF. Children in the Western and Coast provinces were significantly more likely to have not received EarlyBF, compared to the Eastern province, a finding observed in the 1998 data and replicated in the 2003 and 2008–2009 data. The other replicable finding was that non-EarlyBF children were more likely to have been born via caesarean section. Caesarean delivery as a barrier to initiating BF within an hour of birth has been reported in numerous studies.40–42 Explanations advanced for this association include the use of analgesics administered during labour and after delivery that interfere with early development of BF behaviour, and postpartum hospital protocols that separate the mother and the newborn.43 44 However, the effect of caesarean section on EarlyBF is mixed, with some studies reporting a negative correlation and others finding none.45 It is argued that even though obstetric experiences during caesarean mode of delivery may influence a mother's BF behaviours, a window of opportunity still exists to initiate BF within an hour if measures are taken by hospitals to promote it.6 46 47
Returning to the findings of differences between provinces, within-country variation by region and by ethnicity is often observed in child health.48 Mothers from one ethnic group may delay BF because of negative cultural beliefs about BF generally22 49 and about colostrum in particular.15 18 19 It is sensible to assume that unmeasured mediating variables reflecting culture lie in the path between province-of-residence and EarlyBF. One issue is the degree to which the UNICEF analysis framework could account for such unmeasured variables, or whether they belong to constructs that should be in the framework, but are not. This cannot be addressed with the present DHS data, but the findings do provoke this question: what is it about the Western and Coast provinces that results in significantly less EarlyBF compared with the Eastern province? The UNICEF framework may well incorporate the concepts that account for this reliable finding, and further research (perhaps using case study methodology) is needed to illuminate the processes and mechanisms that account for the observed variation in EarlyBF. The framework does not give answers, but it does suggest how to search for answers: findings that distal factors are related to EarlyBF calls for a search for intermediate and proximal factors that explain the link. To give an obvious example, differences in health practices from province to province might be part of the explanation, a factor that could not be detected in the DHS data due to a lack of data on health practices.
The aim of this paper was to undertake a replication analysis. The Introduction section summarised various approaches to this type of research, ending with the suggestion that a rigorous form of replication analysis is to develop a statistical model with one set of data and attempt to replicate it with another set of data. A ubiquitous feature of research is that many data sets on the same subject use different analytical frameworks, different variables and different operationalisation of the same variables. Owing to such differences and other methodological variations, the possibility to implement this rigorous form of replication analysis is quite limited. The problem is that a failure to replicate could be attributed to many factors, only one of which is a poorly fitting model in the original analysis. The DHS offers a rare opportunity to undertake replication analysis with data sets that are highly comparable. The core of DHS questionnaires is essentially the same from year to year and from country to country, as is the methodological approach. Aside from some inevitable variation in content and methodology, the main variation from DHS survey to DHS survey is timing and sample composition. Thus, period effects and sampling effects can be expected to impact analyses and findings. An example of such effects is a large increase from an earlier to a later survey in the level of maternal education, resulting in a rise in health literacy, that in itself might alter the way women responded to survey workers’ interviews, and that actually reflected changes in women's lives and experiences. Such effects might affect associations between variables used in a replication analysis, resulting in poor replication. In such cases, the failure to replicate would be a consequence of changes in the underlying phenomena, and it would be correct to conclude that findings from one context were not applicable to another context, even if both contexts were situated in the same country (periods as contexts).
The Results section did not dwell on the common replicated finding of no association between a possible predictor and the outcome. A good example is the Wealth Index, for which there is no evidence in any of the surveys for an association with EarlyBF. This may be seen as perplexing, given the large literature describing an SES gradient in health. A finding of this type raises some possibilities for further research. There may be an SES gradient in EarlyBF, but the Wealth Index fails to include the SES factors that are important. What is known, because of the replication analysis, is that the Wealth Index is not a reliable predictor of EarlyBF, at least not in Kenya, and this supports the need for further research into the nature of a possible SES association with EarlyBF. As for all analyses, replication analyses may well raise far more questions than they can answer.
This study has strengths and limitations that are interrelated. The study derives its main strength from the usage of national cross-sectional data collected in three surveys to study the reliability of demographic and SES variables in predicting EarlyBF. This is significant because it provides unique data on the degree of confidence nutrition scientists can have about the relative importance of several key putative predictors of early versus late initiation of BF. If the findings from 1998 are closely replicated with data from the succeeding surveys, possible validity problems related to period, cohort and selection effects are ameliorated. The absence of replication calls for further research into such effects. A major limitation of this study relates to the failure to measure a host of sociodemographic, social-psychological, cultural and political variables, which might have effects on EarlyBF. This is an inherent weakness of large-scale survey research, which is unsuited to the detailed investigation of health-related phenomena. It is also important to comment on how the quality of the DHS data limits this study, even if the DHS makes every reasonable effort to produce high-quality data. For example, it is possible that excluded variables such as the number of antenatal visits and type of birth attendant during delivery could have a relationship to EarlyBF. Despite the existence of these variables in the KDHS, these variables were not incorporated in the regression models due to high rates of missing data in one of the surveys.
Conclusions
The objective was to examine the reliability of demographic and SES variables in predicting EarlyBF, by comparing analyses of three highly similar yet independent data sets from 1998, 2003 and 2008–2009. The main finding is that significant predictor variables produced using the 1998 data were poorly replicated using the 2003 and 2008–2009 data. Only mode of birth and province of residence reliably predicted EarlyBF across the three surveys. Children delivered through caesarean section (compared to vaginal birth), and in the Western and Coast provinces (compared to the Eastern province), were at a higher risk of being breastfed later than an hour after birth across all three surveys.
The 1998 KDHS data do not provide the basis for reliable analyses of the correlates of EarlyBF, with reliability conceptualised as replicability using highly similar data sets from 2003 and 2008–2009. We speculate that activities in parts or all of Kenya (eg, political activities leading to changed or new social and welfare programmes, health promotion education and/or policy interventions) changed the analysis context in the period between 1998 and 2008–2009, and that these changes were of a sufficient magnitude to affect the analyses. We cannot pursue this line of reasoning further, because no registry of health-related programmes and activities at local, regional and national levels is available for the study period, as far as we are aware. The establishment of such a registry would be useful as a source of documentation about health interventions undertaken to improve child health. We conclude that reliability analysis is useful to test hypotheses about putative risk and protective factors in the context of descriptive research, perhaps leading to caution as in the present study.
Supplementary Material
Acknowledgments
The authors acknowledge the Kenya Demographic and Health Survey (KDHS) team and all the participants who participated in the 1998, 2003 and 2008–2009 surveys.
Footnotes
Contributors: DJM and MBM conceived the study. DJM conducted the data analysis, interpretation of results and drafting of the manuscript. MBM, HBU and DAA participated in a critical review of the manuscript. All authors read and approved the final manuscript.
Funding: This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: None.
Ethics approval: The scientific and ethical review committee of the Kenya Medical and Research Institute approved the KDHS study protocols.
Provenance and peer review: Not commissioned; externally peer reviewed.
Data sharing statement: No additional data are available.
References
- 1.WHO, UNICEF. Global strategy for infant and young child feeding. Geneva: World Health Organization, 2003. [cited 27 Jan 2014]. http://www.who.int/nutrition/publications/infantfeeding/9241562218/en/ [Google Scholar]
- 2.WHO. Indicators for assessing infant and young child feeding practices: part II measurement. Geneva: World Health Organization, 2010. [cited 27 Jan 2014]. http://www.who.int/nutrition/publications/infantfeeding/9789241599290/en/ [Google Scholar]
- 3.Ministry of Public Health and Sanitation. National strategy on infant and young child feeding 2007 to 2010. Nairobi: Ministry of Public Health and Sanitation, Kenya, 2007. [cited 27 Jan 2014]. http://www.hennet.or.ke/index.php?option=com_jdownloads&Itemid=42&view=finish&cid=101&catid=31&m=0 [Google Scholar]
- 4.Kenya National Bureau of Statistics (KNBS) and ICF Macro. Kenya demographic and health survey, 2008–09. Calverton, MD: KNBS and ICF Macro, 2010 [Google Scholar]
- 5.Edmond KM, Kirkwood BR, Amenga-Etego S, et al. Effect of early infant feeding practices on infection-specific neonatal mortality: an investigation of the causal links with observational data from rural Ghana. Am J Clin Nutr 2007;86:1126–31 [DOI] [PubMed] [Google Scholar]
- 6.WHO. Evidence for the ten steps to successful breastfeeding. Geneva: World Health Organization, 1998. [cited 26 Feb 2014]. http://apps.who.int/iris/handle/10665/43633 [Google Scholar]
- 7.Bhutta ZA, Chopra M, Axelson H, et al. Countdown to 2015 decade report (2000–10): taking stock of maternal, newborn, and child survival. Lancet Lond Engl 2010;375:2032. [DOI] [PubMed] [Google Scholar]
- 8.Hanson LA, Korotkova M. The role of breastfeeding in prevention of neonatal infection. Semin Neonatol 2002;7:275–81 [DOI] [PubMed] [Google Scholar]
- 9.Lawrence RM, Pane CA. Human breast milk: current concepts of immunology and infectious diseases. Curr Probl Pediatr Adolesc Health Care 2007;37:7–36 [DOI] [PubMed] [Google Scholar]
- 10.Huffman SL, Zehner ER, Victora C. Can improvements in breast-feeding practices reduce neonatal mortality in developing countries? Midwifery 2001;17:80–92 [DOI] [PubMed] [Google Scholar]
- 11.Bystrova K, Widström A-M, Matthiesen A-S, et al. Skin-to-skin contact may reduce negative consequences of “the stress of being born”: a study on temperature in newborn infants, subjected to different ward routines in St. Petersburg. Acta Paediatr 2003;92:320–6 [DOI] [PubMed] [Google Scholar]
- 12.Eglash A, Montgomery A, Wood J. Breastfeeding. Dis Mon 2008;54:343–411 [DOI] [PubMed] [Google Scholar]
- 13.Matthiesen A-S, Ransjö-Arvidson A-B, Nissen E, et al. Postpartum maternal oxytocin release by newborns: effects of infant hand massage and sucking. Birth 2001;28:13–19 [DOI] [PubMed] [Google Scholar]
- 14.Salariya EM, Easton PM, Cater JI. Duration of breast-feeding after early initiation and frequent feeding. Lancet 1978;312:1141–3 [DOI] [PubMed] [Google Scholar]
- 15.Tawiah-Agyemang C, Kirkwood BR, Edmond K, et al. Early initiation of breast-feeding in Ghana: barriers and facilitators. J Perinatol 2008;28:S46–52 [DOI] [PubMed] [Google Scholar]
- 16.Lawrence RA, Lawrence RM. Breastfeeding: a guide for the medical profession. St. Louis: Mosby, Inc., 1999:197 [Google Scholar]
- 17.Huffman SL. Determinants of breastfeeding in developing countries: overview and policy implications. Stud Fam Plann 1984;15:170–83 [PubMed] [Google Scholar]
- 18.Gunnlaugsson G, Da Silva MC, Smedman L. Determinants of delayed initiation of breastfeeding: a community and hospital study from Guinea-Bissau. Int J Epidemiol 1992;21:935–40 [DOI] [PubMed] [Google Scholar]
- 19.Davies-Adetugbo AA. Sociocultural factors and the promotion of exclusive breastfeeding in rural Yoruba communities of Osun State, Nigeria. Soc Sci Med 1997;45:113–25 [DOI] [PubMed] [Google Scholar]
- 20.Thulier D, Mercer J. Variables associated with breastfeeding duration. J Obstet Gynecol Neonatal Nurs 2009;38:259–68 [DOI] [PubMed] [Google Scholar]
- 21.Patel A, Badhoniya N, Khadse S, et al. Infant and young child feeding indicators and determinants of poor feeding practices in India: secondary data analysis of National Family Health Survey 200506. Food Nutr Bull 2010;31:314–33 [DOI] [PubMed] [Google Scholar]
- 22.Kimani-Murage EW, Madise NJ, Fotso J-C, et al. Patterns and determinants of breastfeeding and complementary feeding practices in urban informal settlements, Nairobi Kenya. BMC Public Health 2011;11:396. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Engle PL, Menon P, Garrett JL, et al. Urbanization and caregiving: a framework for analysis and examples from Southern and Eastern Africa. Environ Urban 1997;9:253–70 [Google Scholar]
- 24.Victora CG, Huttly SR, Fuchs SC, et al. The role of conceptual frameworks in epidemiological analysis: a hierarchical approach. Int J Epidemiol 1997;26:224–7 [DOI] [PubMed] [Google Scholar]
- 25.Miller B, Townsend A, Carpenter E, et al. Social support and caregiver distress a replication analysis. J Gerontol B Psychol Sci Soc Sci 2001;56:S249–56 [DOI] [PubMed] [Google Scholar]
- 26.La Sorte MA. Replication as a verification technique in survey research: a paradigm. Sociol Q 1972;13:218–27 [Google Scholar]
- 27.Lindsay RM, Ehrenberg AS. The design of replicated studies. Am Stat 1993;47:217–28 [Google Scholar]
- 28.Tsang EW, Kwan K-M. Replication and theory development in organizational science: a critical realist perspective. Acad Manage Rev 1999;24:759–80 [Google Scholar]
- 29.Thompson B. The pivotal role of replication in psychological research: empirically evaluating the replicability of sample results. J Pers 1994;62:157–76 [Google Scholar]
- 30.Valentine JC, Biglan A, Boruch RF, et al. Replication in prevention science. Prev Sci 2011;12:103–17 [DOI] [PubMed] [Google Scholar]
- 31.Schmidt S. Shall we really do it again? The powerful concept of replication is neglected in the social sciences. Rev Gen Psychol 2009;13:90 [Google Scholar]
- 32.Berthon P, Pitt L, Ewing M, et al. Potential research space in MIS: a framework for envisioning and evaluating research replication, extension, and generation. Inf Syst Res 2002; 13:416–27 [Google Scholar]
- 33.Armstrong R, Waters E, Jackson N, et al. Guidelines for systematic reviews of health promotion. Version 2. Australia: Melbourne University, 2007 [Google Scholar]
- 34.Graves PL. Nutrition and infant behavior: a replication study in the Katmandu Valley, Nepal. Am J Clin Nutr 1978;31:541–51 [DOI] [PubMed] [Google Scholar]
- 35.National Council for Population and Development (NCPD), Central Bureau of Statistics (CBS) (Office of the Vice President and Ministry of Planning and National Development, Kenya), and Macro International Inc. (MI). Kenya Demographic and Health Survey, 1998. Calverton, MD: NCPD, CBS, and MI, 1999 [Google Scholar]
- 36.Central Bureau of Statistics (CBS) Kenya, Ministry of Health (MOH) Kenya, and ORC Macro. Kenya Demographic and Health Survey 2003. Calverton, MD: CBS, MOH, and ORC Macro, 2004 [Google Scholar]
- 37. MEASURE DHS, ICF International, Calverton. [cited 8 Feb 2014]. http://www.measuredhs.com/data/Access-Instructions.cfm.
- 38.Rutstein SO, Rojas G. Guide to DHS statistics [Internet]. Demographic and Health Surveys ORC Macro Calverton, Maryland. 2006. [cited 28 Jan 2014]. http://www.measuredhs.com/pubs/pdf/DHSG1/Guide_DHS_Statistics.pdf [Google Scholar]
- 39.Rutstein SO, Johnson K. The DHS Wealth Index (DHS Comparative Reports No. 6). Calverton: ORC Macro, 2004 [Google Scholar]
- 40.Dewey KG, Nommsen-Rivers LA, Heinig MJ, et al. Risk factors for suboptimal infant breastfeeding behavior, delayed onset of lactation, and excess neonatal weight loss. Pediatrics 2003; 112:607–19 [DOI] [PubMed] [Google Scholar]
- 41.Chapman DJ, Perez-Escamilla R. Identification of risk factors for delayed onset of lactation. J Am Diet Assoc 1999;99:450–4 [DOI] [PubMed] [Google Scholar]
- 42.Yanikkerem E, Tuncer R, Yilmaz K, et al. Breast-feeding knowledge and practices among mothers in Manisa, Turkey. Midwifery 2009;25:e19–32 [DOI] [PubMed] [Google Scholar]
- 43.Righard L, Alade MO. Effect of delivery room routines on success of first breast-feed. Lancet 1990;336:1105–7 [DOI] [PubMed] [Google Scholar]
- 44.Nissen E, Lilja G, Matthiesen A-S, et al. Effects of maternal pethidine on infants’ developing breast feeding behaviour. Acta Paediatr 1995;84:140–5 [DOI] [PubMed] [Google Scholar]
- 45.Dennis C-L. Breastfeeding initiation and duration: a 1990–2000 literature review. J Obstet Gynecol Neonatal Nurs 2002; 31:12–32 [DOI] [PubMed] [Google Scholar]
- 46.Rowe-Murray HJ, Fisher JR. Baby friendly hospital practices: cesarean section is a persistent barrier to early initiation of breastfeeding. Birth 2002;29:124–31 [DOI] [PubMed] [Google Scholar]
- 47.Vestermark V, Høgdall CK, Birch M, et al. Influence of the mode of delivery on initiation of breast-feeding. Eur J Obstet Gynecol Reprod Biol 1991;38:33–8 [DOI] [PubMed] [Google Scholar]
- 48.Wilmoth TA, Elder JP. An assessment of research on breastfeeding promotion strategies in developing countries. Soc Sci Med 1995;41:579–94 [DOI] [PubMed] [Google Scholar]
- 49.Watson BM. Ethnicity and Breastfeeding in Kenya. 2013. [cited 11 Jan 2014]. http://trace.tennessee.edu/cgi/viewcontent.cgi?article=2628&context=utk_chanhonoproj
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.