

Abstract
Study Design
It is a multicenter, controlled case study review of a big scale of pedicle-screw procedures from January 2000 to June 2010. The outcomes were compared to those with no implant failure.
Purpose
The purpose of this study was to review retrospectively the outcome of 100 patients with implant failure in comparison to 100 control-patients, and to study the causes of failure and its prevention.
Overview of Literature
Transpedicular fixation is associated with risks of hardware failure, such as screw/rod breakage and/or loosening at the screw-rod interface and difficulties in the system assembly, which remain a significant clinical problem. Removal or revision of the spinal hardware is often required.
Methods
Two hundred patients (88 women, 112 men) were divided into 2 major groups, with 100 patients in group I (implant failure group G1) and 100 patients in group II (successful fusion, control group G2). We subdivided the study groups into two subgroups: subgroup a (single-level instrumented group) and subgroup b (multilevel instrumented group). The implant status was assessed based on intraoperative and follow-up radiographs.
Results
Implant failure in general was present in 36% in G1a, and in 64% in G1b, and types of implant failure included screw fracture (34%), rod fracture (24%), rod loosening (22%), screw loosening (16%), and failure of both rod and screw (4%). Most of the failures (90%) occurred within 6 months after surgery, with no reported cases 1 year postoperatively.
Conclusions
We tried to address the problem and study the causes of failure, and proposed solutions for its prevention.
Keywords: Lumbar, fixation; Screw, failure; Fusion; Fracture fixations, prosthesis; Loosening
Introduction
Failures of implanted pedicle screws are not unavoidable complications or sequelae of ongoing degeneration, in a properly performed fusion. Failure to provide adequate stabilization can necessitate additional surgical procedures to achieve spinal fusion [1]. An understanding of fundamental biomechanical principles of the spine and fixation strategies is essential to avoid unnecessary subsequent failures [1,2].
1. Study objective
In this comparative case series, we tried to highlight the topic of metal (hardware, or implant) failure in transpedicular lumbar fixation as a challenging surgical issue. The purpose of the study was to review the outcome of 100 patients who had pedicle screw fixation of the thoracolumbar, lumbar, and lumbosacral regions with implant failure and compare the outcome to the outcome of 100 control-patients without failure, in order to study the causes of failure and ways to avoid it as much as possible. We tried to identify and highlight some questions and their possible answers in this study, including: Is the posterior transpedicular-screw-fixation system a suitable system for fixing a particular case? Is this system the only needed one to fix a particular case? What is the difference between instrumented fixation and bony fusion? Lastly, how can we minimize the incidence of different forms of implant failure?
Materials and Methods
1. Study idea and description
This study is a practical clinical (pragmatic) study that measures treatment effectiveness and aims to inform choices between treatments. Thus, the present study is a multicenter, pragmatic, controlled, case study series conducted and designed to evaluate the clinical problem of implant failure after thoracolumbar, lumbar, and lumbosacral fixation with transpedicular screws. The evaluation of the imaging studies was blinded.
2. Patient screening
The majority of participants in the study were identified from existing patients of the departments of neurosurgery and orthopedics in two different universities namely, Cairo and Ain Shams universities, in addition to other departments of neurosurgery and orthopedics in the hospitals of the Ministry of Health in Egypt. Pedicle-screw procedures done by many orthopedic and neurological surgeons on a big scale from January 2000 to June 2010 were screened. The screening consisted of demographic data, medical and surgical history with coexisting diseases, physical examination, radiographic and laboratory evaluation, and indications for surgery. The type of surgery, number of levels fused, and the type of hardware and grafts used intraoperatively were reviewed. The preoperative diagnosis, possible postoperative complications, and the presence of an osseous union were reviewed. Finally, outcomes were analyzed.
We studied two matched groups of patients. One hundred patients (56 men, 44 women; age, 32-79 years) of postoperative hardware frank failure were studied (implant failure, study group G1). A control group of patients with similar characteristics and of similar number, but without implant failure, was also studied (successful fusion, control group G2). The study groups were subdivided into two subgroups: subgroup a, single-level posteriorly instrumented group; and subgroup b, multilevel posteriorly instrumented group, i.e., patients with more than two contiguous vertebral involvements (at two or more levels).
3. Patient selection criteria
To be included in group 1 of the study, there should be an obvious frank failure of instrumentation with cutting out of devices attached to the lamina, breakage of screw, or loosening of rod, etc. All the selected cases had, at least, one form or another of hardware problems.
4. Radiological follow-up evaluation and outcome assessment
The mean duration of follow-up was 2 years (range, 1-3 years). Implant status was assessed on the basis of intraoperative, immediate postoperative and follow-up radiographs. We compared the outcome data to the baseline within both groups and with each other at various time intervals. We evaluated the efficacy of the surgical procedure, together with the instrumentation implantation, by comparing preoperative and postoperative clinical data and radiological findings.
5. Implant failure radiological analysis
The postoperative plain radiological studies include the standard anteroposterior and lateral radiographs. Oblique views in certain cases were performed and multisection plain tomography was performed in some cases. In a few cases, there was a need for a computed tomography scan. The radiographs were interpreted for 1) manifestations of failure of fixation; 2) the effect of implant failure; 3) the point of instrumentation failure; 4) screw axis, screw length and diameter, rod length and diameter, and rod contouring; and 5) failed cases were interpreted in comparison to the successful cases in order to enhance the radiological differences that may be considered as markers of failure.
6. Radiological fusion analysis
All patients underwent follow-up for a minimum of 1 year. Successful fusion was determined by evaluating the radiographs for the presence of bridging bone between the fused segments and the trabeculae through the fusion mass. However, it is often very difficult to tell if a patient's spine has fused, and it can be even harder to determine if further fusion surgery is necessary. In general, it takes at least three months to get a solid fusion, and it can take up to a year in some cases.
Results
We analyzed the clinical and radiological outcomes in 200 random patient samples (88 women, 112 men) of both successful and failed transpedicular screw fixation of the thoracolumbar, lumbar, and lumbosacral regions, after a minimum of one year. We divided the sample into two matched groups of patients. The failure or study group (G1) included 100 patients (56 men, 44 women; age, 32-79 years) of postoperative hardware problems (failed implants). A control group (G2) included a similar patient number and characteristics, but without implant failure. We further subdivided each group into two subgroups: subgroup a, single-level group and subgroup b, multilevel group, i.e., patients with more than two contiguous posteriorly instrumented (at two or more) levels. Each group of patients had 100 implants that were evaluated and studied. Fig. 1 shows plain X-ray radiographs of the lumbosacral spine (LSS) of different cases showing different mechanisms and forms of screw breakage.
Fig. 1.

Plain X-ray radiographs of the lumbosacral spine of different cases showing different mechanisms and forms of screw breakage.
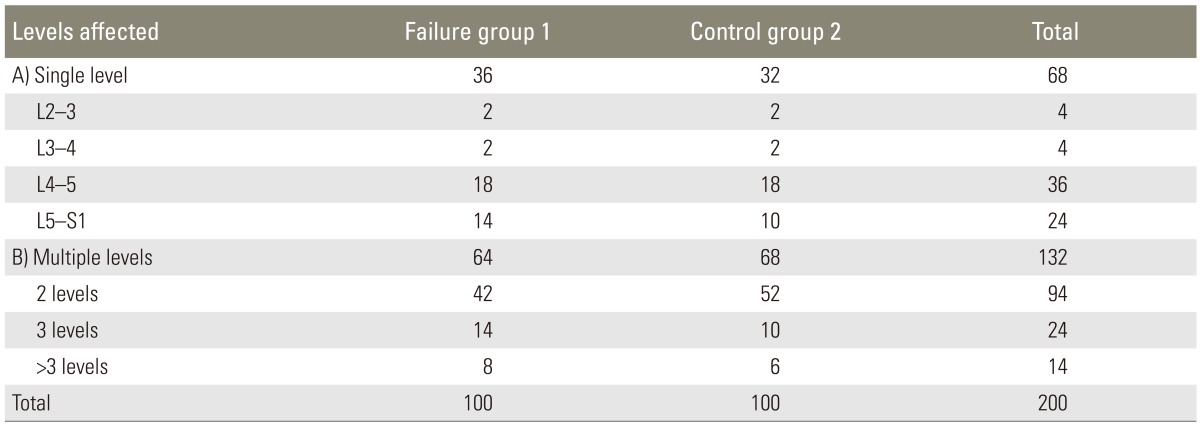
There were 68 single-level and 132 multilevel fusions in both groups (Table 1). In group 1a, single-level fusions were 36 cases (L2-3 in 2 case, L3-4 in 2, L4-5 in 18, and L5-S1 in 14 cases), and in group 1b, multi-level fusions were in 64 cases (double level in 42 cases, 3 levels in 14 cases, and more than 3 levels in 8 cases). A group of almost similar cases were included in the control group. The mean extent of fusion was 1.5 motion segments (range one to four motion segments).
Table 1.
Levels affected and fixed in both groups and subgroups
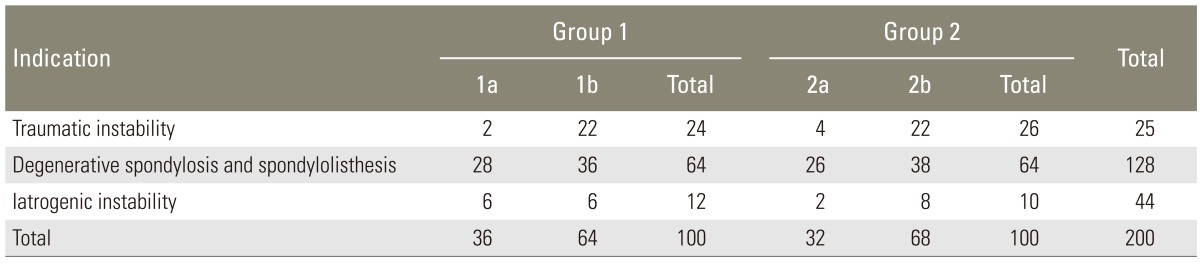
Indications for fixation were traumatic instability (50 patients), degenerative spondylosis or spondylolisthesis (128 patients), and iatrogenic instability (22 patients) (Table 2). In both failure and control groups, degenerative instability accounted for the majority of the treated cases, followed by traumatic instability, and lastly, iatrogenic instability accounted for the least number of cases. Single level fusions were less than multilevel ones in all indications; however, the difference between single and multilevel fusions in degenerative instability was the smallest one.
Table 2.
Indications for fixation
There were 110 individual complications in 100 patients of the failure group (G1) and 6 patients in the other 100 controls. The complications seen were screw misplacement, coupling failure of the device, wound infection, loosening and/or breakage of screws, loosening and/or breakage of rods. Most of the studied screws, in both groups, were inserted within the pedicle and the vertebral body. In 12 cases (6 in G1, 6 in G2), one screw (per case) perforated the bony vertebral cortex. All the selected G1 cases had one form or another of hardware problems. Implant failure in general was present in 36 cases (36%) in G1a, and in 64 cases (64%) in G1b, including screw fracture (34 cases, 34%), rod fracture (24 cases, 24%), rod loosening (22 cases, 22%), screw loosening (16 cases, 16%), and failure of both rod and screw (4 cases, 4%) (Table 3). We found that most of the failures (90%) occurred within 6 months after surgery, with a small number (10%) occurring in the following 6 months (usually coinciding with some form of trauma), with no reported cases after 1 year postoperatively.
Table 3.
Radiological patterns of implant failure in relation to number of fixed levels and laterality
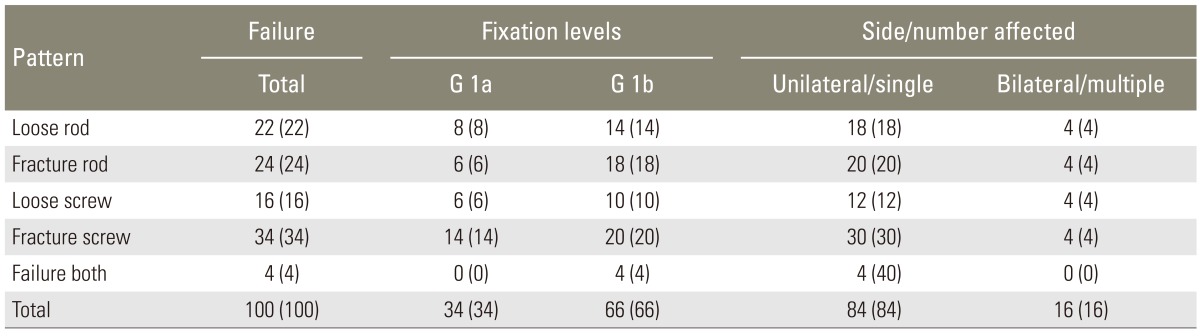
Values are presented as number (%). Percentages are in relation to the total number per group.
Unilateral/single=regarding form and number of failed components.
Bilateral/multiple=regarding forms and numbers of failed components.
In general, screw complications (50%) were slightly more than rod complications (46%), with the least frequent being coupling failure of both elements (4%). The 4 cases of coupling failure were fracture of both screw and rod in one case and loosening of both in the other case. All forms of implant failure were more common in patients with multilevel fusions (Table 3). The commonest form of failure was fracture screw, accounting for 34% of the total forms of failure, followed by rod fracture (24%), rod loosening (22%), and then the least frequent form, namely loose screw, which accounted for 16%. Most of the screws that broke were of an early design. All the 100 patients had an exploration; 30 of them already had solid fusions, and 70 had pseudarthrosis. Eight patients (8%) had at least one further reoperation for one or more re-failures.
Regarding the screw axis, the screws placed through the pedicle parallel to the endplate were 40% in G1 and 70% in G2; non-parallel screws were more common in the implant failure group (60%) than the control group (30%). Regarding rod length, the long rod placed in multilevel fixation was found more often in the failure group (66%) than in the control group (52%). The failed short rod group (34%) had longer ends in almost half of these cases. Regarding rod contouring, it was done in 88% of cases of the control group in comparison to only 54% of the failure group (Table 4).
Table 4.
Other radiological observations
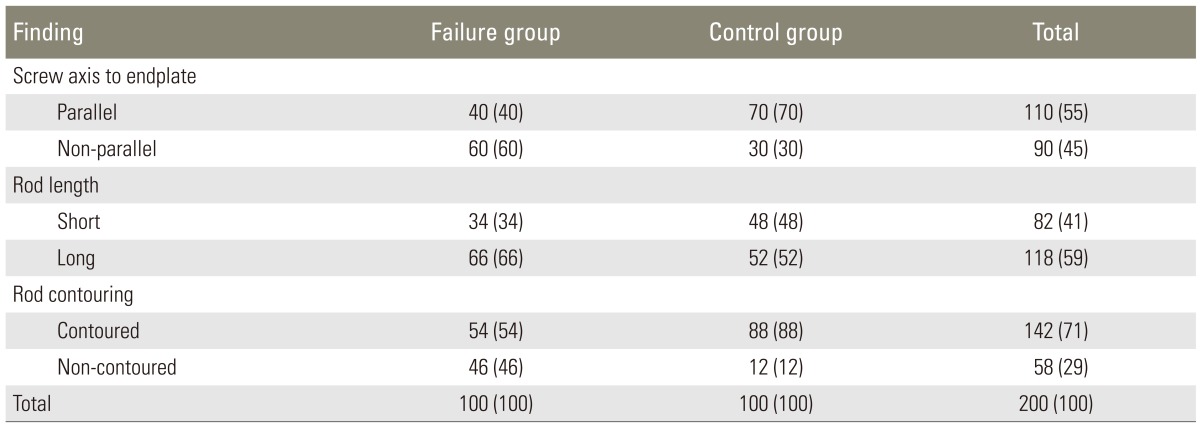
Values are presented as number (%). Percentages are in relation to the total number per group.
The point of screw fracture (points of maximum stress) was at the fulcrum in 20 cases out of 36 cases of screw fracture (34 cases of single fracture and 2 cases of coupling fracture) (Table 5).
Table 5.
Radiological analyses of the site and number of points of failure per implant
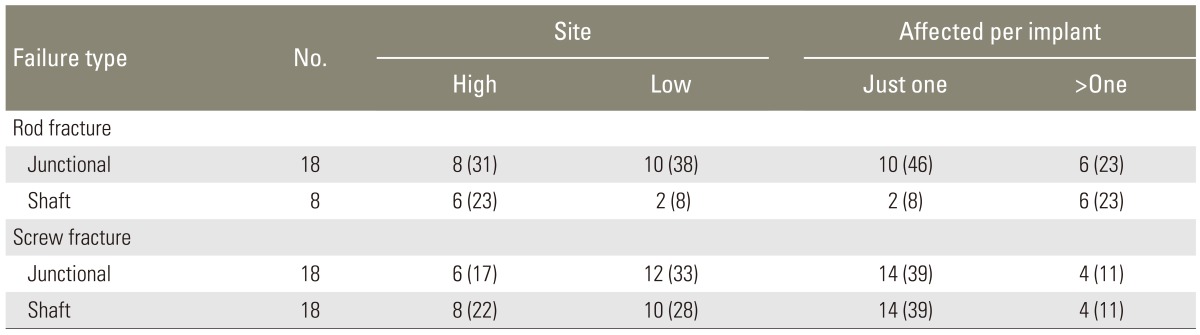
Values are presented as number (%). Percentages are in relation to the number of each failure type (approximate).
The failure type=single failure type+number of coupling failures.
Our data showed that screw fracture was the most common failure in cases of traumatic instability with anterior column defects, (12% out of 24% of all failure forms in the trauma group). We reported no screw-thread fracture. The loose screw was the least frequent form of implant failure, accounting for 16% of all failures; we reported most of them (10% out of the 16%) in degenerative instability, and the rest (6% out of the 16%) in iatrogenic instability. We reported no cases of screw loosening in traumatic instability. Most of our studied screws were titanium. Frank loosening was the sole criterion for inclusion in this form of failure in our cases (Table 6). Fig. 2 shows plain X-ray radiographs of the lumbosacral spine of different cases showing different mechanisms and forms of rod breakage. Notice the points of rod failure are always near the screw-plate/rod junction (point of maximum stress). Fig. 3 shows X-ray radiographs of the LSS spine showing screw loosening: one can notice that screws are non-parallel to the endplates and there is gradual increase in the step denoting progressive instability with time. Fig. 4 shows plain X-ray radiographs of the LSS spine showing screw loosening: There is bilateral loosening of more than one screw. The rods are long and the screws show loss of parallism to the vertebral endplates.
Table 6.
Radiological analyses of the patterns of failure in relation to the cause of instability
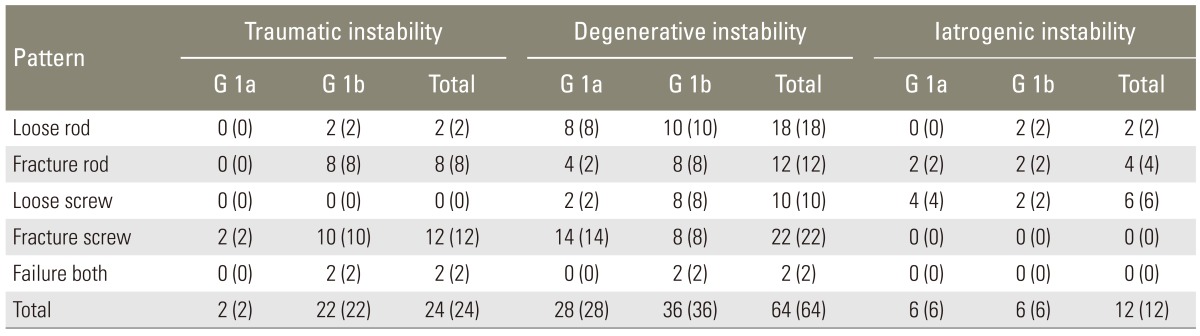
Values are presented as number (%). Percentages are in relation to the total number per group.
Fig. 2.

Plain X-ray radiographs of thelumbosacral spine of different cases showing different mechanisms and forms of rod breakage. Notice the points of rod failure are always near the screw-plate/rod junction (point of maximum stress).
Fig. 3.

(A-C) Plain X-ray radiographs of the lumbosacral spine spine showing screw loosening: one can notice that screws are non-parallel to the endplates and there is gradual increase in the step denoting progressive instability with time.
Fig. 4.

Plain X-ray radiographs of the lumbosacral spine showing screw loosening: There is bilateral loosening of more than one screw. The rods are long and the screws show loss of parallelism to the vertebral endplates.
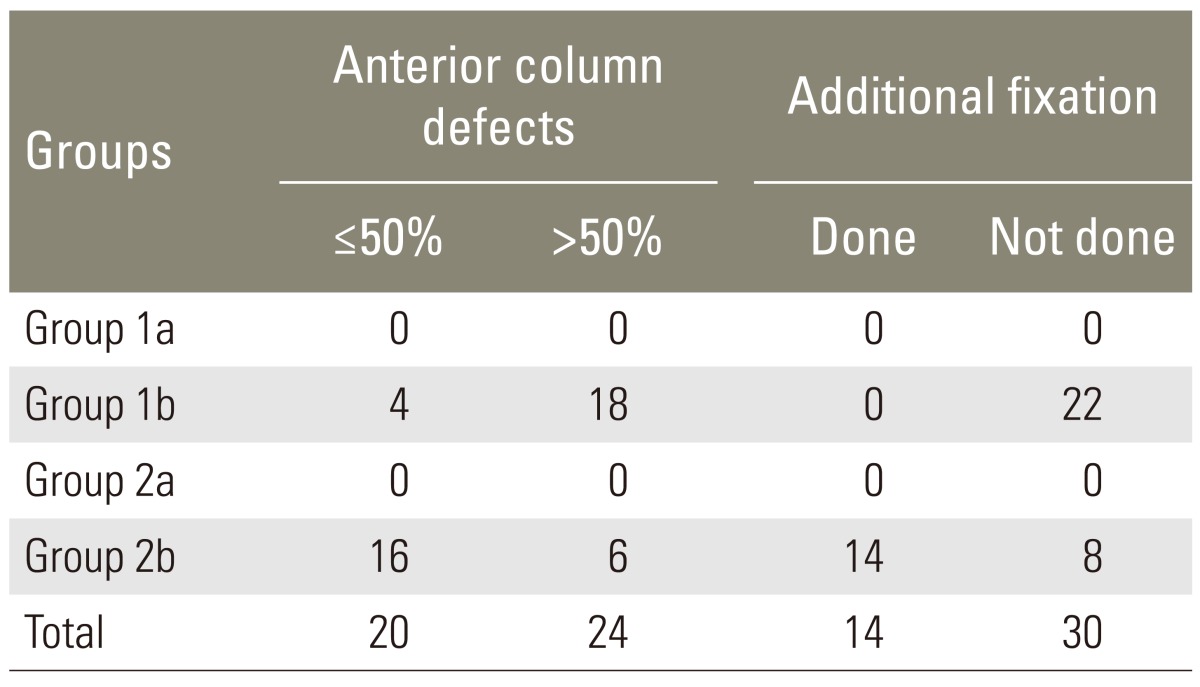
In traumatic cases, no anterior column defects were encountered in single level fixation cases in both failure and control groups. Defects of more than 50% collapse of the anterior vertebral body height were more frequent in the failure group trauma cases (9 cases out of 12). In contrast, defects of less than 50% collapse of the anterior vertebral body height were more frequent in the control group cases (16 cases out of 26). Additional fixation techniques were not done in any of the failure cases. However, the addition of more fixation points was done in 14 trauma cases of the control group (Table 6).
Fig. 5 shows plain X-ray radiographs of the lumbosacral spine of different cases showing rod loosening (all are long rods transfixing multiple levels).
Fig. 5.

(A-D) Plain X-ray radiographs of the lumbosacral spine of different cases showing rod loosening (all are long rods transfixing multiple levels).
Regarding bony union, pedicle-screw-based posterolateral fusion, using the autograft obtained from laminectomy augmented by bone strips from the iliac crest was the routine procedure in 90% of cases of the control group, with 10% of cases having anterior interbody fusion, with or without cages, as an alternative. On the other hand, posterolateral fusion alone, using only the autograft obtained from laminectomy, allografts and/or synthetic bone, was the rule in the majority (80%) of cases of the failed implant group, with 20% of the cases having no bony fusion whatsoever. None of the patients had anterior surgery.
Fig. 6 shows plain tomogram evaluation of bony fusion in the failure group: a) showing a bony bar bridging the left transverse process of L3 & L4, with incomplete merge with the later; b) showing evidence of incomplete bony fusion between the left transverse processes of D12 and L1, with a bony bar projecting downwards from the right L1 transverse process with no definite fusion with that of L2. Fig. 7 shows plain radiography and coronal reformatted computed tomography images showing different forms of adding bony fusion in the control group: a) intertransverse fusion, b) anterior interbody bony fusion (ALIF with bone graft), c) anterior interbody cage fusion (ALIF with cages).
Fig. 6.

Plain tomogram evaluation of bony fusion in the failure group (A) showing a bony bar bridging the left transverse process of L3 & L4, with incomplete merge with the later, (B) showing evidence of incomplete bony fusion between the left transverse processes of D12 and L1, with a bony bar projecting downwards from the right L1 transverse process with no definite fusion with that of L2.
Fig. 7.

Plain radiography and coronal reformatted computed tomography images showing different forms of bony fusion in the control group: (A) intertransverse fusion, (B) anterior interbody bony fusion (ALIF with bone graft), (C) anterior interbody cage fusion (ALIF with cages).
Another important finding in this study was that the addition of supplemental fixation sites was a criterion of many cases of the control group, but only 4 cases of the failure group, and in both groups, the cases were traumatic instability with more than 50% anterior column defects. The addition of supplemental fixation sites in the control group constituted one or more component of attachment of the two screws in an individual vertebra with use of a metal crosslink, and the addition of two more screws at the pathology level or extra level, especially in junctional zones, or anterior interbody fusion with cages.
Discussion
Spinal surgery can be more of an art than a science. Planning surgery is one thing, and performing surgery is another! The objective of lumbar spine fixation surgery is to stop motion at a painful spine segment, minimizing the pain and allowing the patients to increase their function [3,4,5]. Several implant devices are used for this purpose. During the past decade, the use of pedicle screws in spinal stabilization has gradually and dramatically increased [6,7]. Pedicle screws now are the standard routine procedure in spinal fixation surgery for many types of spinal problems [8]. With its frequent use, and despite its advantages over other fixation techniques, transpedicular screw fixation is associated with risks of hardware failure and pedicle fracture during screw insertion [9,10]. Incidences of hardware failures have been reduced over the last two decades. However, these forms of implant failure remain a significant clinical problem, particularly in patients with poor vertebral bone quality.
1. Addressing the problem of transpedicular implant failure
It is important to remember that the main purpose of the procedure is to achieve a solid arthrodesis and without this, any form of internal fixation may eventually fail [8,10,11]. If a solid fusion is not obtained, but the hardware is intact and there is still good stability to the spine, the patient may still have good pain relief with the surgery. This finding made some authors to believe that achieving spinal stability alone is more important than obtaining a solid fusion. However, an implant can fatigue and break; and it can fail before the bones fuse [9,10,11,12]. This is usually an indicator of continued gross spinal instability and a second traumatic surgical operation is required. It is therefore a race between the spine fusing and the metal failing. In our series, like other reported series, we found that most of the failures (90%) occurred within 6 months after surgery, with a small number (10%) occurring in the following 6 months (usually coinciding with some form of trauma), with no reported cases after 1 year postoperatively. This early occurrence of hardware failure, before bony union, and the lack of failures after one year postoperatively strongly support the idea that instrumented fixation cannot be a permanent form of fixation, and bony fusion should be the important target of intervention. Once the bony fusion has matured, the hardware itself could even be safely removed [13,14]. Thus, improving bone-bone union is the corner stone of improving the outcome and preventing implant failure. In general, the iliac crest has been the best source of high-quality graft. Bone chips from the laminae and spinous processes can be added.
Another important finding is that, with improved fixation techniques, surgeons have attempted to limit their use of extra autogenous bone graft to avoid making a separate incision over the iliac crest. Allograft and synthetic bone have been used with pedicle-screw-based constructs, with greater or lesser success depending on the pathology and the host-related variables [15,16]. Their success rate is too poor for it to be used routinely, and this technique adds to the causes of implant failure. The reason why one continues to harvest bone from the crest is its strong potential to lead to a solid fusion. A review of the results in our patients demonstrated that the union rate with pedicle-screw-based posterolateral fusion alone, using only the autograft obtained from laminectomy, allografts and/or synthetic bone, was inferior to that using bone chips from the laminae and spinous processes, augmented by strips from iliac crest bone. Moreover, we found that the use of interbody fusion techniques as an alternative strongly adds to successful results. Here, we would like to mention that many studies supported the idea that lumbar interbody fusion techniques have several theoretical and proven advantages over posterior lateral on-lay grafting techniques. In posterior lateral fusion, the barriers to successful arthrodesis are much greater. The graft is not under compression, vascularity is not as good, and the graft-host interface is less reliable [14,15,16,17,18].
Fixation failure typically occurs when the implant, implant-bone interface, or component-component junction fails. Some of the common reasons for failure after spinal fusions include poor bone healing, poor alignment of the fusion, or suboptimal strategy, causing subsequent stress on the implant, leading to pain and eventually implant failure [19,20].
The literature reported another important point to mention, which is, the higher the number of fused segments, the higher the likelihood of implant failure; implant failure were more uncommon in one level fusion [13,21,22]. This was also the case in our study, in which all forms of implant failure were more common in patients with multilevel fusions (Table 3). Thus, the percentage of failures increases as the distance between the screws increases.
2. Addressing the general causes of implant failure
As reported, the success of spinal fusion surgery was dependent on patient populations, surgeons involved, and the research design methods. Failure of the implant after spinal fusions might be the result of doing it for the wrong patient, with the wrong diagnosis, by the wrong surgeon [1,2,3,4]. We add to these causes: using the wrong implant, and/or doing the wrong technique. The wrong patient is the patient chosen for fixation with pathology that will not benefit from the procedure, or is contraindicated for fixation. We want to stress the fact that very few people with degenerative low back pain require a fusion. This is, in our view, the first and most important preventive measure to decrease the incidence of implant failure, namely, stoppage of unnecessary fusions. The wrong diagnosis includes misdiagnosis, inadequate preoperative studies, or poor choice of the surgical approach. The wrong surgeon is the one who does not master these complex techniques. Literature studies showed a ten-fold variation in outcomes between surgeons.
Regarding the wrong implant, several unique implant features are needed to stop or resist failure problems. The implant components should be made of a special alloy with high mechanical strength and fatigue resistance while maintaining flexibility. Many different types have been developed to attach a pedicle screw to a plate or a rod; some are quite rigid and some, less rigid. Different types of pedicle screws currently on the market result in different outcomes. Many reports found the complication rate to be highly dependent on the manufacturer and type of instrumentation used [23]. Thus, each type of device must be evaluated individually for safety and effectiveness.
Discussing the wrong technique, it may be a wrong surgical detail or just a wrong belief! Without solid fusion, there is a risk of the instrumentation loosening or even breaking. Conversely, if instrumentation is loose or malpositioned from the start, then there is definite reduction in the chances of successful fusion. Some surgeons stopped the use of bone grafts depending solely on the instrumented fixation. The basic difference between fixation and fusion in their decision-making became hazy. Moreover, one of the most common causes of implant failure is poor surgical planning. Sticking to the basic surgical techniques with case-dependent planning of the procedure, aiming to decrease these forms of failure is, in our viewpoint, the solution.
3. Forms and modes of hardware failure and their solutions
In the literature, the rate of screw misplacement ranged from 0%-2% up to 25%-95% in patients with scoliosis in different series, and to nearly 4.2% in those with degenerative diseases [1,5]. However, in this series, 6% had screw misplacement, equally distributed in both failure and control groups, questioning its significance. Apart from screw misplacement, we reported three forms of lumbar transpedicular hardware failure, namely axial component (screw) failure, longitudinal component (rod/plate) failure, and coupling failure of both hardware components.
We reported two modes of screw failure: screw breakage and screw loosening. In our series, forms of screw failure represented 50% of all failures; 12% of them were reported in cases of traumatic instability, 32% in degenerative instability, and 6% in iatrogenic instability. The reported incidence of most of the literature series reported the incidence to all the operated cases, in contrast to our series, in which the incidence was to the failure cases only.
4. Screw breakage
The screw breakage, in the reported series, was the most significant form of hardware failure. Many reports have focused on the complication of pedicle screw breakage. In the literature, the frequency of screw breakage ranged from 2.6%-4.9% to 9%-36% to as high as 60% [5,6,9,10]. Our findings run parallel to these previous reports. The commonest form of failure in our study was fracture screw, accounting for 34% of the total forms of failure. However, comparing these different figures may be misleading because the percentage in our series was in comparison to the failure forms only, in contrast to other series in which the percentage was part of the whole study population in relation to a certain type of instability and its general surgical outcome. Nevertheless, all agree that screw fracture is the commonest form of hardware failure. The reported high screw breakage rates in the literature were seen in highly comminuted spinal fractures, internally fixed with posterior short-segment pedicle-screw-based instruments. This was also the case in our series, where screw fracture was the most common failure in cases of traumatic instability with anterior column defects (12% out of 24% of all failure forms in the trauma group) (Table 7). We reported no screw-thread fracture, and the literature has never reported it, to our knowledge. The percentage of screw breakage increases as the distance between the screws increases and it may occur more than six months after surgery. In these cases, pedicle screw breakage has nothing to do with bony fusion or pseudarthrosis; trauma is the offender in many cases.
Table 7.
Anterior column defects in cases of traumatic instability
Screws are most prone to fail at points of maximum stress. The fulcrum was found to be the point where screw fracture is most likely to occur. This is related to the inner diameter of a screw, to the differences in integrity of the materials through which the screw passes and resistance of the loads applied. The importance of the 'Load Sharing' classification, especially in cases of traumatic instability, has been documented. The resulting load-sharing score can assist in predicting fixation failure. The higher the load sharing score, the higher is the fixation failure rate [14,23]. Although initial screw-breakage rates were high, we can reduce it even to zero when the influence of comminution of the vertebral body is appreciated (Fig. 8) [13,24]. Our study findings strongly enforce this idea. The high failure rate in traumatic instability coincided with the high incidence of anterior column defects in those cases. It is simply attractive to consider reconstitution of the vertebral body in junctional highly stressed zones as is often considered. We suggest that anterior vertebrectomy, grafting, reconstruction, and instrumentation are essential in patients with severely comminuted injury to avoid the high screw-breakage rates.
Fig. 8.

The load-sharing effect of different forces on deformity progression in spondylolisthesis (A); anterior column compression defects (B).
In our series, the most common location of mechanical failure clinically was at the lower screws. This was also the case in some reported series. Considerable loading of the caudal screw-bone junction often leads to failure. Appreciating the dynamic angular relationships of the spinal junctional zones is crucial. This high failure rate at the junctional regions is related, in part, to the angle of the screw in relation to the axis that is perpendicular to the floor (Fig. 9). The distal fixation sites may be further exposed to failure within an increasing anterior column deficit. Distal attachment sites of the sacrum are mechanically weak in comparison to pedicle fixation within the proximal lumbar spine. Moreover, long multi-segmental fixation tends to load the more caudal screws far more than the rostral screws. Long implants are associated with a high failure rate. When clinically appropriate, the use of a shorter length implant, with its shorter moment arm, may decrease the risk of caudal construct failure.
Fig. 9.

Plain radiography of the lumbosacral spine showing the screw failure point (the point of maximum stresses secondary to the bending forces applied to the screw). One can note that the point is near the screw-plate/rod junction.
Regarding the screw axis, the screws were placed through the pedicle parallel to the endplate; non-parallel screws are associated with a high risk of implant failure. Regarding rod length, the long rod placed in multilevel fixation is more liable to be broken at the point of maximal stress. In addition, long constructs are associated with disparities in the angles. Regarding rod contouring, it is required in multilevel fixation and long constructs.
5. Screw pullout, loosening
Screw pullout, loosening and screw-connector disengagement have been reported both in in vitro testing and in patients. Many reports have focused on the frequency of screw loosening. An extensive literature review showed a frequency of screw loosening that varied from 0.6% to 11%. These studies with low rates of loosening of the screws do not comment on radiological methods or the criteria for screw loosening. In other studies with strict radiological criteria for screw loosening, the loosening rates ranged from 21% to 27% [25,26]. In contrast, our data showed that the loose screw was the least common form of implant failure, accounting for 16% of all failures; we reported most of them (10% out of the 16%) in degenerative instability, and the rest (6% out of the 16%) in iatrogenic instability. We reported no cases of screw loosening in traumatic instability. Frank loosening was the sole criterion for inclusion in our cases of this form of failure. The major factors involved and reported in the literature are the quality of the bone, the screw size and design, the screw insertion method, and the bone quality at the insertion site [27]. In all those studies, stainless steel screws were used with very few exceptions. Most of our studied screws were titanium. In most studies, including this series, screws of different designs and from different vendors were used. Therefore, it seems unlikely that the varying results could be explained by differences in materials and screw designs. We can explain the varying incidences of screw loosening in these studies by the differences in study design, with different definitions of screw loosening employed, and great variation in the follow-up of the patients. It seems likely that several of the literature studies underestimated the frequency of loosening.
The mechanism of screw loosening has been controversial. The main failure mode reported by some researchers is pullout, while unscrewing is not a failure mode seen clinically. Other authors describe it as a toggling phenomenon (nonfixed end of the screw degrade the integrity of the bone, by means of a "windshield whipping" motion) under caudocephalad loads [24,25,26,28]. According to Christensen et al. [23], the rotational stability of the screw is essential and is dependent on the size of the screw and the quality of the bone in the interface. The diameter of the screw is limited by the size of the pedicle, and could not be further increased [23]. Thus, the most effective way to improve the pullout strength of pedicle screws is to improve the bone quality. Another important way is improving the screw-bone grip [20,25,28]. The stabilizing influence of using converging screws, if possible, also was emphasized. Pullout resistance is proportional not only to the volume of bone between screw threads but also to the triangular area defined by the screw (Fig. 10). In the present study, we found that screw length did not contribute significantly to pullout resistance, however, triangulated screws significantly increase resistance.
Fig. 10.

Plain radiography of the lumbosacral spine and diagrammatic representation showing the effect of triangulation: adds more stability, increasing the chance of good grip (G2) and decreasing the chance of loosening (G1).
We are now satisfied that the surgeon should attempt to distribute loads such that no single portion of the implant or spine bears an excessive portion of the load. This can be accomplished by providing additional implant-bone interfaces, and by normalizing the geometry. The addition of supplemental fixation sites definitely adds to the stability of the construct, which is proportional to the number of high-quality fixation points. The fundamental improvement in pullout strength obtained by cross-linking has been documented [26]. We found that a rigid cross bar implant, with or without two more screws (at the pathology level or extra level) acts as a bridging implant that resists spinal deformation. The anterior interbody fusion shares the load with the rest of the construct absorbing up to 80% of the axial load (Fig. 8). From this finding, many spine surgeons routinely began to use circumferential fusion for all cases of degenerative spinal disease.
In our practice, bicortical purchase is routinely used at the first sacral level but never at any other level. Investigators demonstrated that patients with poor bone-mineral density were very poor candidates for pedicle-screw-based internal fixation. Others have strongly suggested the routine use of bone-mineral-density testing before surgery, although mild osteoporosis did not seem to affect screw purchase or clinical outcome adversely [27].
6. Longitudinal component failure
Regarding longitudinal component (rod/plate) failure, rod breakage has been reported only rarely [4,10,29,30]. This study reported rod breakage as the second most common form of failure, representing 24% of all forms of failure. Rod breakage was most common in traumatic instability with anterior column defects (8% out of 24%). Despite that, the incidence of rod breakage is more in degenerative instability (12% out of 24%); it is less common than traumatic cases because the number of affected cases were 8 out of 48 in traumatic cases, in contrast to 12 out of 128 degenerative cases. The same applied to cases of iatrogenic instability, which represented 4% out of the 24% total percentage of rod breakage, while the number of affected cases was 4 out of 24 cases. Thus, in relation to the number of cases per single pathology, traumatic instability comes first, followed by iatrogenic and lastly degenerative instability, in the percentage of rod breakage. The high percentage in traumatic instability may be explained by the high percentage of uncorrected anterior column defects in these cases, which add stress loads on the system components. Most of the fractured rods were in the multilevel fixation subgroup (18 out of 24 cases). On the other hand, rod loosening represented 22% of all forms of failure in this study, and were most commonly reported in cases of degenerative instability.
In the literature, the rod diameter was the most important factor in affecting the maximum stress values, as one expects. The maximum stress values decreased as the diameters increased. Similar to screws, plates/rods break at the point at which maximum stress is applied. Therefore, we can minimize the incidence of rod/plate breakage by increasing the rod diameter [29].
Fig. 8 shows the load-sharing effect of different forces on deformity progression in spondylolisthesis (Fig. 8A); anterior column compression defects (Fig. 8B).
Fig. 9 shows plain radiography of the LSS showing the screw failure point (the point of maximum stresses secondary to the bending forces applied to the screw). One can note that the point is near the screw-plate/rod junction.
Fig. 11 shows plain radiography showing the fundamental improvement after the addition of more fixation points in the form of a rigid cross bar (Fig. 11A, C) and/or extra-screws (Fig. 11A-C).
Fig. 11.

Plain radiography showing the fundamental improvement after the addition of more fixation points in the form of a rigid cross bar (A, C) and/or extra-screws (A-C).
Fig. 10 shows plain radiography of the LSS and diagrammatic representation showing the effect of triangulation: adds more stability, increasing the chance of good grip (G2) and decreasing the chance of loosening (G1).
Lastly, we want to stress that, unfortunately, even in the best hands, a fusion may not form as intended and a suboptimal or poor result may develop. Thus, the optimal treatment for complex spinal conditions remains a challenge. Use of the patient's own bone, instrumentation and good surgical technique can improve the chances of developing a solid spinal fusion and decrease the chances of implant failure. Many details are not clear to us yet. There is still need for an optimum instrumentation system that can restore the biomechanics of the fused vertebral segments, as well as relieve pain, and enhance resolution of the neurological deficit, increasing the resistance to the stress loads and minimizing failures.
Conclusions
We recommend 1) Limiting the use of lumbar instrumentation in unstable situations; 2) Treatment must be individualized with evaluation of both the benefits and the risks of all available therapeutic options for every single case; 3) Surgery should include decompression, spinal realignment with maintenance of lumbar lordosis as much as possible, rigid posterior instrumentation, and a period of bed rest and/or bracing to allow bony union and fusion maturation; 4) The proper use of pedicle screws requires knowledge of the patient's pedicle anatomy, the use of image intensification during the application, the use of primarily autograft material, and the availability of a full inventory of implants; 5) The choice of pedicle screw implant system requires adequate screw size, rigid rod attachment to the screws, adequate rod size to resist bending moments, adequate pedicle and sacral anatomy to take normally positioned screws, and adequate bone density, accurate placement with minimal posterior cortical destruction, screw placement to the anterior vertebral body and bicortical screw placement at S1; 6) With anterior column height loss, fully constrained rigid systems are required. An implant should not terminate at or near a junctional zone. The combination of stable pedicle screws and cross bridging bars creates stable points of fixation for correction; 7) When instrumentation placement is planned, the surgeon should be aware that distal attachment sites of the sacrum are mechanically weak in comparison to pedicle fixation within the proximal lumbar spine.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Masferrer R, Gomez CH, Karahalios DG, Sonntag VK. Efficacy of pedicle screw fixation in the treatment of spinal instability and failed back surgery: a 5-year review. J Neurosurg. 1998;89:371–377. doi: 10.3171/jns.1998.89.3.0371. [DOI] [PubMed] [Google Scholar]
- 2.Arnold PM, Strang RD, Roussel D. Efficacy of variable-angle screws in transpedicular fixation. Neurosurg Focus. 1999;7:e1. doi: 10.3171/foc.1999.7.6.4. [DOI] [PubMed] [Google Scholar]
- 3.Bennett GJ, Serhan HA, Sorini PM, Willis BH. An experimental study of lumbar destabilization. Restabilization and bone density. Spine (Phila Pa 1976) 1997;22:1448–1453. doi: 10.1097/00007632-199707010-00005. [DOI] [PubMed] [Google Scholar]
- 4.Esses SI, Sachs BL, Dreyzin V. Complications associated with the technique of pedicle screw fixation. A selected survey of ABS members. Spine (Phila Pa 1976) 1993;18:2231–2238. doi: 10.1097/00007632-199311000-00015. [DOI] [PubMed] [Google Scholar]
- 5.Schnee CL, Freese A, Ansell LV. Outcome analysis for adults with spondylolisthesis treated with posterolateral fusion and transpedicular screw fixation. J Neurosurg. 1997;86:56–63. doi: 10.3171/jns.1997.86.1.0056. [DOI] [PubMed] [Google Scholar]
- 6.Gaines RW., Jr The use of pedicle-screw internal fixation for the operative treatment of spinal disorders. J Bone Joint Surg Am. 2000;82:1458–1476. doi: 10.2106/00004623-200010000-00013. [DOI] [PubMed] [Google Scholar]
- 7.Aebi M, Thalgott JS, Webb JK. Modular stabilization system: the universal spine system. In: Aebi M, Thalgott JS, Webb JK, editors. AO ASIF principles in spine surgery. Berlin: Springer-Verlag; 1998. pp. 123–196. [Google Scholar]
- 8.Cunningham BW, Kotani Y, McNulty PS, Cappuccino A, McAfee PC. The effect of spinal destabilization and instrumentation on lumbar intradiscal pressure: an in vitro biomechanical analysis. Spine (Phila Pa 1976) 1997;22:2655–2663. doi: 10.1097/00007632-199711150-00014. [DOI] [PubMed] [Google Scholar]
- 9.Duncan JD, MacDonald JD. Extraction of broken pedicle screws: technical note. Neurosurgery. 1998;42:1399–1400. doi: 10.1097/00006123-199806000-00138. [DOI] [PubMed] [Google Scholar]
- 10.Faraj AA, Webb JK. Early complications of spinal pedicle screw. Eur Spine J. 1997;6:324–326. doi: 10.1007/BF01142678. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Abumi K, Kaneda K. Pedicle screw fixation for nontraumatic lesions of the cervical spine. Spine (Phila Pa 1976) 1997;22:1853–1863. doi: 10.1097/00007632-199708150-00010. [DOI] [PubMed] [Google Scholar]
- 12.Kowalski RJ, Ferrara LA, Benzel EC. Biomechanics of bone fusion. Neurosurg Focus. 2001;10:E2. doi: 10.3171/foc.2001.10.4.3. [DOI] [PubMed] [Google Scholar]
- 13.Parker JW, Lane JR, Karaikovic EE, Gaines RW. Successful short-segment instrumentation and fusion for thoracolumbar spine fractures: a consecutive 41/2-year series. Spine (Phila Pa 1976) 2000;25:1157–1170. doi: 10.1097/00007632-200005010-00018. [DOI] [PubMed] [Google Scholar]
- 14.Donovan DJ, Polly DW, Jr, Ondra SL. The removal of a transdural pedicle screw placed for thoracolumbar spine fracture. Spine (Phila Pa 1976) 1996;21:2495–2498. doi: 10.1097/00007632-199611010-00017. [DOI] [PubMed] [Google Scholar]
- 15.Gibson JN, Grant IC, Waddell G. The Cochrane review of surgery for lumbar disc prolapse and degenerative lumbar spondylosis. Spine (Phila Pa 1976) 1999;24:1820–1832. doi: 10.1097/00007632-199909010-00012. [DOI] [PubMed] [Google Scholar]
- 16.Suk SI, Lee CK, Kim WJ, Lee JH, Cho KJ, Kim HG. Adding posterior lumbar interbody fusion to pedicle screw fixation and posterolateral fusion after decompression in spondylolytic spondylolisthesis. Spine (Phila Pa 1976) 1997;22:210–219. doi: 10.1097/00007632-199701150-00016. [DOI] [PubMed] [Google Scholar]
- 17.Thomsen K, Christensen FB, Eiskjaer SP, Hansen ES, Fruensgaard S, Bunger CE. 1997 Volvo Award winner in clinical studies. The effect of pedicle screw instrumentation on functional outcome and fusion rates in posterolateral lumbar spinal fusion: a prospective, randomized clinical study. Spine (Phila Pa 1976) 1997;22:2813–2822. doi: 10.1097/00007632-199712150-00004. [DOI] [PubMed] [Google Scholar]
- 18.Ondra SL, Marzouk S. Revision strategies for lumbar pseudarthrosis. Neurosurg Focus. 2003;15:E9. doi: 10.3171/foc.2003.15.3.9. [DOI] [PubMed] [Google Scholar]
- 19.Schlenk RP, Stewart T, Benzel EC. The biomechanics of iatrogenic spinal destabilization and implant failure. Neurosurg Focus. 2003;15:E2. doi: 10.3171/foc.2003.15.3.2. [DOI] [PubMed] [Google Scholar]
- 20.Kanayama M, Cunningham BW, Weis JC, Parker LM, Kaneda K, McAfee PC. The effects of rigid spinal instrumentation and solid bony fusion on spinal kinematics. A posterolateral spinal arthrodesis model. Spine (Phila Pa 1976) 1998;23:767–773. doi: 10.1097/00007632-199804010-00004. [DOI] [PubMed] [Google Scholar]
- 21.Kothe R, Panjabi MM, Liu W. Multidirectional instability of the thoracic spine due to iatrogenic pedicle injuries during transpedicular fixation. A biomechanical investigation. Spine (Phila Pa 1976) 1997;22:1836–1842. doi: 10.1097/00007632-199708150-00008. [DOI] [PubMed] [Google Scholar]
- 22.Lynn G, Mukherjee DP, Kruse RN, Sadasivan KK, Albright JA. Mechanical stability of thoracolumbar pedicle screw fixation. The effect of crosslinks. Spine (Phila Pa 1976) 1997;22:1568–1572. doi: 10.1097/00007632-199707150-00007. [DOI] [PubMed] [Google Scholar]
- 23.Christensen FB, Dalstra M, Sejling F, Overgaard S, Bunger C. Titanium-alloy enhances bone-pedicle screw fixation: mechanical and histomorphometrical results of titanium-alloy versus stainless steel. Eur Spine J. 2000;9:97–103. doi: 10.1007/s005860050218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.McLain RF, Sparling E, Benson DR. Early failure of short-segment pedicle instrumentation for thoracolumbar fractures. A preliminary report. J Bone Joint Surg Am. 1993;75:162–167. doi: 10.2106/00004623-199302000-00002. [DOI] [PubMed] [Google Scholar]
- 25.Barber JW, Boden SD, Ganey T, Hutton WC. Biomechanical study of lumbar pedicle screws: does convergence affect axial pullout strength? J Spinal Disord. 1998;11:215–220. [PubMed] [Google Scholar]
- 26.Dick JC, Zdeblick TA, Bartel BD, Kunz DN. Mechanical evaluation of cross-link designs in rigid pedicle screw systems. Spine (Phila Pa 1976) 1997;22:370–375. doi: 10.1097/00007632-199702150-00003. [DOI] [PubMed] [Google Scholar]
- 27.Renner SM. 2001 Bioengineering Conference, ASME, BED. Vol. 50. New York: ASME; 2001. Pedicle screw pull-out strength is augmented by an injectable calcium phosphate and varies by injection. [Google Scholar]
- 28.Gaines RW, Carson WL, Satterlee CC, Groh GI. Improving quality of spinal internal fixation: evolution toward "ideal immobilization": a biomechanical study. Orthop Trans. 1987;11:86–87. [Google Scholar]
- 29.Rohlmann A, Calisse J, Bergmann G, Radvan J, Mayer HM. Clamping stiffness and its influence on load distribution between paired internal spinal fixation devices. J Spinal Disord. 1996;9:234–240. [PubMed] [Google Scholar]
- 30.Okuyama K, Abe E, Suzuki T, Tamura Y, Chiba M, Sato K. Can insertional torque predict screw loosening and related failures? An in vivo study of pedicle screw fixation augmenting posterior lumbar interbody fusion. Spine (Phila Pa 1976) 2000;25:858–864. doi: 10.1097/00007632-200004010-00015. [DOI] [PubMed] [Google Scholar]