

Abstract
Targeting angiogenesis is proving to be a successful approach in the management of ovarian cancer. The vascular endothelial growth factor inhibitor, bevacizumab, is the first angiogenesis inhibitor to have shown a significant progression-free survival advantage in the Phase III setting. There is now evidence supporting the use of bevacizumab in combination with chemotherapy for first-line and relapsed (platinum-sensitive and resistant) ovarian cancer. In this review, we summarize the positive Phase III trial (OCEANS [Ovarian Cancer Study Comparing Efficacy and Safety of Chemotherapy and Anti-Angiogenic Therapy in Platinum-Sensitive Recurrent Disease]) that led to European Medicines Agency approval of bevacizumab in platinum-sensitive first relapse and discuss the best use of the drug in this disease.
Keywords: antiangiogenic, recurrent, ovarian
Introduction
Ovarian cancer is diagnosed in approximately 225,000 women per year and there are over 140,000 deaths worldwide per year from this disease.1 The majority of women continue to present at advanced stages and the overall 5-year survival rate is approximately 40%.2 Although epithelial ovarian cancer has been traditionally treated as one disease entity, it is now established as a heterogeneous disease. There are five main histopathological types (high-grade serous, clear cell, endometrioid, mucinous, and low-grade serous) that are characterized by distinct molecular aberrations and clinical behavior (eg, response to treatment, survival).3 Recognition of the biological differences has led to the development of clinical trials for specific subtypes that focus on targeted therapies.4 The initial treatment of advanced ovarian cancer consists of maximal cytoreductive surgery and platinum-based chemotherapy.5 Over the years, there have been studies addressing other chemotherapy combinations, duration of treatment, and the addition of a third agent;6,7 however, up until recently, there was little doubt that carboplatin in combination with paclitaxel (3-weekly) remained the standard of care for first-line therapy in advanced ovarian cancer. The addition of the antiangiogenic agent bevacizumab (Avastin®; Genentech, South San Francisco, CA, USA) to standard therapy was shown to significantly improve survival in two Phase III trials and is arguably the standard of care for selected patients.8,9 Bevacizumab in combination with carboplatin and paclitaxel as first-line therapy is approved by the European Medicines Agency (EMA). Other regimens that have shown promise in the first-line setting are the use of intraperitoneal chemotherapy10 and dose-dense administration of paclitaxel (weekly) with carboplatin.11 These approaches are under further evaluation in ongoing clinical trials, which will help to clarify their role in the management of ovarian cancer.
The treatment of recurrent ovarian cancer is guided by the time to progression from the last platinum-based treatment.5 The prognosis is poor for women in which the platinum-free interval is less than 6 months (platinum-resistant) or disease progression occurs during platinum-based treatment (platinum-refractory), with a median overall survival (OS) typically less than 12 months. Options include weekly paclitaxel, pegylated liposomal doxorubicin (PLD), topotecan, and gemcitabine.12,13 Patients with a platinum-free interval of more than 6 months (platinum-sensitive disease) are likely to benefit from further platinum. A number of platinum-containing regimens have been demonstrated to be effective in this setting and include carboplatin with paclitaxel,14 carboplatin with gemcitabine,15 and a combination of carboplatin with PLD.16 Surgery for relapsed ovarian cancer is considered for selected patients and ongoing clinical trials are addressing this role (eg, Gynecologic Oncology Group (GOG) 213 study [Clinicaltrials.gov identifier: NCT00565851], Arbeitsgemeinschaft Gynaekologische Onkologie (AGO)-OVAR desktop III [Clinical trials.gov identifier: NCT01166737]).
Despite improvements in surgical and chemotherapeutic approaches, the majority of women with relapsed ovarian cancer eventually die from the disease and there is a desperate need to improve treatments. There are many targeted agents under investigation in relapsed ovarian cancer. Of these, the antiangiogenic approach is the first to have shown meaningful anticancer activity. In this article, we summarize the role of bevacizumab in platinum-sensitive ovarian cancer and discuss its place in clinical practice.
Overview of the mechanisms and pharmacology of bevacizumab
Angiogenesis refers to the formation of new blood vessels, which is an important step for tumor growth beyond 1 mm in size and the metastatic process. It is regulated by several pro-and antiangiogenic factors, and of these, vascular endothelial growth factor (VEGF) plays a major role. The VEGF family comprises several ligands, VEGFA, and placental growth factor 1 and 2, which bind to VEGF receptors.17,18 Of these, VEGFA (referred to as VEGF) is the most well-studied. VEGFR2 (VEGF receptor 2) is expressed on endothelial cells and is believed to be the primary receptor for VEGF-mediated effects on angiogenesis, as well as vascular permeability. In addition, VEGFR2 expression on the surface of tumor cells has been reported, suggesting paracrine and autocrine pathways.19
Bevacizumab is a humanized monoclonal antibody that binds to VEGFA. In preclinical xenograft models, bevacizumab demonstrated tumor growth inhibition20,21 and inhibition of metastases formation.21,22 Furthermore, synergistic antitumor activity may occur when combined with chemotherapy or radiotherapy. This may be mediated by “normalization” of tumor vasculature, facilitating delivery of therapeutic agents to cancer cells and increasing oxygenation.23,24 Bevacizumab is licensed for the treatment of advanced colorectal, breast, lung, renal, and ovarian carcinomas. Bevacizumab is administered intravenously. The infusion duration is initially over 90 minutes and this can be reduced to 30–60 minutes for subsequent cycles if tolerated.25 The metabolism and elimination of bevacizumab is similar to endogenous immunoglobulin G and are likely to involve the reticuloendothelial system rather than renal or hepatic routes.26 The half-life is approximately 18–20 days and depends on factors such as sex and serum albumin.25 Preclinical studies suggest that bevacizumab may improve the antitumor activity of paclitaxel by increasing the delivery and efficacy of the drug.7
Bevacizumab in ovarian cancer: clinical evidence in combination with platinum-based chemotherapy
A number of studies have shown VEGF overexpression in ovarian carcinoma and suggested high levels of VEGF as a prognostic factor associated with advanced International Federation of Gynecology and Obstetrics (FIGO) stage and early recurrence.28–31 In preclinical models, anti-VEGF therapy effectively inhibited tumor progression and the formation of malignant effusions, enhancing the activity of cytotoxic agents.32
In 2011, two pivotal first-line studies, GOG-02188 and International Collaboration on Ovarian Neoplasms (ICON) 7,9 reported that the addition of bevacizumab to the combination of carboplatin and paclitaxel, followed by maintenance therapy significantly improved progression-free survival (PFS) (GOG-0218, HR: 0.72, P<0.001; ICON7, HR: 0.81, P<0.004). This led to the approval of bevacizumab in the first-line treatment of ovarian cancer by the EMA. Furthermore, the final OS results in ICON7 demonstrated an OS advantage of 4.8 months (restricted mean 34.5 months versus [vs] 39.3 months; HR: 0.78, 95% confidence interval [CI]: 0.63–0.97, P<0.03) in the bevacizumab arm for the subgroup of patients with a poor prognosis (high-risk group defined as FIGO stage IV disease or FIGO stage III disease and more than 1.0 cm of residual disease after debulking surgery).33
A number of Phase II trials explored the efficacy and safety of bevacizumab in relapsed ovarian cancer (Table 1), and reported response rates between 15% and 56.4% and PFS from 4.4 to 8 months.34–39 These encouraging results in populations that included heavily pretreated women with platinum-resistant and platinum-sensitive disease warranted further investigation in the Phase III setting. The OCEANS (Ovarian Cancer Study Comparing Efficacy and Safety of Chemotherapy and Anti-Angiogenic Therapy in Platinum-Sensitive Recurrent Disease) trial was the first randomized Phase III trial to demonstrate the utility of an antiangiogenic agent in relapsed ovarian cancer (Figure 1).40 In this double-blind, placebo-controlled study, 484 patients with first platinum-sensitive relapse (recurrence >6 months after front-line platinum-based therapy) were randomized to receive bevacizumab or placebo in combination with chemotherapy (carboplatin with gemcitabine) followed by maintenance therapy until progression. No prior chemotherapy for recurrent disease was allowed. Randomization was 1:1 and stratification factors were time from last platinum treatment to recurrence (6–12 months vs >12 months) and whether cytoreductive surgery for recurrence was performed. Patients were randomized to receive carboplatin AUC (area under the curve) 4 on day 1 in combination with gemcitabine 1,000 mg/m2 on day 1 and 8 plus bevacizumab 15 mg/kg or placebo on day 1, every 21 days. Following six cycles of chemotherapy (up to ten cycles permitted if response continues) in combination with bevacizumab or placebo, patients continued bevacizumab/placebo alone (maintenance) until disease progression or unacceptable toxicity.
Table 1.
Evidence of bevacizumab in treatment of recurrent EOC
| Design | Population | ORR, PFS (months) | |
|---|---|---|---|
| GOG170D (Burger et al34) 62 pts |
Bev 15 mg/kg every 21 days | ≤2 lines of previous treatment 58% Pl resistant 26% Pl sensitive with Pl-free interval <12 months |
ORR 21% PFS 4.7 |
| Garcia et al35 70 pts |
Bev 10 mg/kg every 14 days + cyclophosphamide 50 mg daily | Upfront Pl-based treatment +≤2 previous line for recurrence1 40% Pl resistant 60% Pl sensitive2 |
ORR 24% PFS 7.2 |
| Cannistra et al36 44 pts |
Bev 15 mg/mq every 21 days | Three previous lines of chemotherapy Pl resistant |
ORR 15.9% PFS 4.4 |
| Nimeiri et al37 13 pts |
Bev 15 mg/mq every 21 days + erlotinib 150 mg daily | Upfront Pl-based treatment +≤2 previous line for recurrence 31% Pl refractory 15% Pl resistant 54% Pl sensitive |
ORR 15% – |
| Tillmanns et al38 48 pts |
Bev 10 mg/kg every 14 days + Ab-paclitaxel on days 1, 8, and 15 every 28 days | Pl resistant | ORR 50% PFS 8.0 |
| Wenham et al39 41 pts |
Bev 15 mg/kg every 21 days + Docetaxel 40 mg/mq on days 1 and 8 every 21 days |
Equal to or less than three lines of previous treatment3 46% Pl resistant 54% Pl sensitive with Pl-free interval <12 months |
ORR 56.4% PFS 5.2 |
Abbreviations: Bev, bevacizumab; EOC, epithelial ovarian cancer; ORR, overall response rate; Pl, platinum; PFS, progression-free survival; pts, patients.
Figure 1.
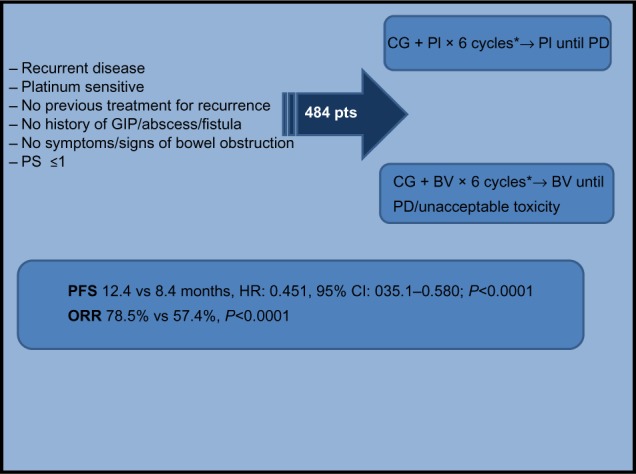
OCEANS study.
Note: *Up to ten cycles in case of ongoing response.
Abbreviations: BV, bevacizumab 15 mg/m2; CI, confidence interval; CG, carboplatin AUC 4 (area under the curve), gemcitabine 1,000 mg/m2; GIP, gastrointestinal perforation; HR, hazard ratio; ORR, overall response rate; PD, progression disease; PFS, progression-free survival; Pl, placebo; PS, Eastern Cooperative Oncology Group Performance Status; pts, patients; vs, versus; OCEANS, Ovarian Cancer Study Comparing Efficacy and Safety of Chemotherapy and Anti-aging Therapy in Platinum-Sensitive Recurrent Disease.
The study met the primary endpoint demonstrating that the addition of bevacizumab to carboplatin/gemcitabine significantly increases PFS compared with placebo (12.4 months vs 8.4 months, HR: 0.484, 95% CI: 0.388–0.605, P<0.0001). The PFS benefit was maintained regardless of age, performance status, time to recurrence, and cytoreductive status. Importantly, there was a significant improvement in overall response rate (79.5% vs 57.4%, P<0.0001) for bevacizumab-treated patients. However, no improvement in OS was reported. A possible explanation is that a substantial proportion (>30%) of patients in the placebo arm went on to receive bevacizumab for subsequent relapse outside the context of the study.
This trial led to EMA approval for bevacizumab in combination with carboplatin gemcitabine in patients with first recurrence of platinum-sensitive epithelial ovarian cancer or fallopian tube or primary peritoneal cancer who have not received prior therapy with bevacizumab or other VEGF pathway-directed agents.41
Safety and tolerability
Prior to the ovarian cancer studies, the safety profile of bevacizumab was based on over 4,500 patients predominantly treated in combination with chemotherapy in clinical trials of breast, colorectal, lung, and renal carcinoma; the toxicities in ovarian cancer patients are consistent with those reported in other malignancies. The majority of the toxicities are shared with other VEGF-directed agents, and includes hypertension, proteinuria, bleeding, and thromboembolism. Hypertension is a frequent toxicity but can usually be managed adequately using standard antihypertensive medications (eg, angiotensin-converting-enzyme inhibitors, calcium channel blockers).42–44 Several mechanisms have been hypothesized by which VEGF inhibition may cause hypertension, including reduced synthesis of the vasodilator nitric oxide, leading to increased vascular resistance.45 Rarer, serious adverse events include severe nephrotic syndrome, reversible posterior leukoencephalopathy syndrome, gastrointestinal (GI) perforation, fistula formation, and hemorrhage. No new safety concerns were identified in the OCEANS study.40 It should be noted that the dose of bevacizumab in the OCEANS study was 15 mg/kg every 3 weeks, which is the same as the first-line GOG-218 study but twice the dose used in the first-line ICON7 trial (7.5 mg/kg). The overall incidence of serious adverse events (≥ grade 3) reported in the trial was higher in the bevacizumab arm compared with placebo (24.9% vs 34.8%). As expected, the rates of grade 3 or higher hypertension (0.4% vs 17.4%), proteinuria (0.9% vs 8.5%), and venous thromboembolism (2.6% vs 4.0%) were higher in the bevacizumab arm. There was no difference in the incidence of febrile neutropenia and no cases of GI perforation during treatment or within 30 days of discontinuing bevacizumab. The toxicity profile is encouraging given the concerns raised following the rates of GI perforation reported in earlier Phase II studies of bevacizumab in recurrent ovarian cancer. In a Phase II study of single-agent bevacizumab in platinum-resistant ovarian cancer, 11.4% of patients developed GI perforation.36 It is noteworthy that the incidence was higher in patients that had received three prior chemotherapy lines compared to two (23.8% vs 0%). In another study that included platinum-sensitive and -resistant patients whom had received a maximum of two prior lines of treatment, there were no reported cases of GI perforation.34 Rectosigmoid disease involvement and the presence of bowel obstruction are potential risk factors for bevacizumab-related bowel perforation. Given the results from the OCEANS trial and first-line studies, (perforation rates in the ICON-7 and GOG218 trials were 1% and 2.6%, respectively),8,9 it appears that GI perforation/fistula are more likely to occur in heavily treated patients rather than in the initial treatment or at first relapse.
Patient-focused perspectives
Despite the large number of clinical trials of bevacizumab in multiple malignancies, there are relatively few data regarding the impact of bevacizumab on quality of life (QoL). Unfortunately, patient-reported outcomes (PROs) were not recorded in the OCEANS study;40 hence, it is difficult to assess the overall benefit taking into consideration QoL and improved PFS in the absence of an OS advantage in platinum-sensitive ovarian cancer. However, QoL information is available for bevacizumab in the initial treatment of ovarian cancer. In the ICON-7 study, PROs were obtained using the European Organisation for Research and Treatment of Cancer quality-of-life questionnaire – ovarian cancer module (EORTC QLQ-OV28), and the EORTC QLQ-C30. This information was collected at baseline (before randomization), every 21 days throughout the chemotherapy phase, every 6 weeks up to 12 months in the maintenance phase, and subsequently, every 3 months for up to 24 months. Bevacizumab continuation treatment was associated with a small but statistically significant decrease in QoL compared with standard treatment.46 In the GOG 218 trial, PROs were also recorded using the trial outcome index of the Functional Assessment of Cancer Therapy – Ovary (FACT-O-TOI) prior to cycles 1, 4, 7, 13, and 21, and 6 months after completing protocol-directed therapy. The QoL scores were lower in the bevacizumab-containing arms during the period it was administered with chemotherapy (compared to chemotherapy alone). However, no significant differences were noted over the bevacizumab maintenance period.47 The number of hospital attendances for maintenance bevacizumab administration, toxicities, and treatment related to the management of toxicities are all factors that need to be taken into consideration when counseling patients regarding the benefits of this drug in recurrent ovarian cancer. At a time when the cost-effectiveness of bevacizumab in recurrent ovarian cancer in the absence of an OS benefit is debated, PROs are very important in the clinical decision-making process. Furthermore, when considering cost-effectiveness, it is important to recognize that the dose of bevacizumab used in the OCEANS study was double the dose used in the first-line ICON7 study (7.5 mg/kg, 3-weekly). There are no reported studies in the relapsed setting of bevacizumab at 7.5 mg/kg (3-weekly), and therefore it is not possible to confirm whether a similar advantage in PFS would be seen at the lower dose. However, given the benefit in terms of PFS and OS seen in high-risk patients in the ICON7 trial where bevacizumab was administered at 7.5 mg/kg (3-weekly), there is merit in exploring bevacizumab at this dose in relapsed disease.
Place in therapy
There is now strong evidence from Phase III trials to support the use of bevacizumab as part of management of first-line, first platinum-sensitive relapse and platinum-resistant settings. The AURELIA study, a Phase III trial of bevacizumab in combination with chemotherapy (PLD, topotecan, or weekly paclitaxel) until progression, demonstrated a statistically significant improvement in PFS (3.4 months vs 6.7 months; HR: 0.48, P<0.001) in platinum-resistant ovarian cancer.48 Despite the lack of advantage in OS, the findings from both OCEANS and AURELIA strongly support a role for bevacizumab in recurrent disease. Bevacizumab is currently licensed and has EMA approval in ovarian cancer for both first-line treatment and for first-line platinum-sensitive relapse (if the patient has had no prior anti-VEGF therapy). To date, the evidence for bevacizumab in platinum-sensitive ovarian cancer is in combination with carboplatin and gemcitabine, and this option is considered standard of care in many cancer centers. However, the optimal clinical situation (ie, upfront, platinum-sensitive, or platinum-resistant setting) for which patients derive the most benefit from bevacizumab remains unknown. Platinum-resistant ovarian cancer is the most challenging situation to treat, and therefore, there is an argument to reserve bevacizumab for this situation. However, despite the significant and clinically meaningful benefit for bevacizumab with chemotherapy in platinum-resistant disease, bevacizumab is currently not licensed for this indication. Therefore, in current clinical practice, for the majority of oncologists, the question is whether to offer patients bevacizumab as first-line therapy or at first platinum-sensitive recurrence. A reasonable proposal is that for newly diagnosed patients with no residual disease following surgery (low-risk of early relapse), bevacizumab should be reserved for first recurrence. However, for newly diagnosed patients with high-risk disease (stage III residual disease >1 cm, stage IV), bevacizumab should be utilized as first-line therapy (with carboplatin/paclitaxel, followed by maintenance bevacizumab) as this is the scenario where a significant OS advantage is seen. In addition, it is currently unclear whether patients derive benefit by continuing bevacizumab at the time of progression whilst instituting a new line of systemic therapy.
The main limitations of bevacizumab are resistance to treatment, toxicities, and cost. It is therefore essential to identify methods that select those patients that will derive most benefit with least chance of life-threatening toxicities. There are currently no validated biomarkers predicting clinical efficacy following bevacizumab in ovarian cancer, although studies investigating gene expression arrays, plasma VEGF levels, and imaging techniques such as multiparametric magnetic resonance (MR) and positron emission tomography (PET) imaging are underway.
Resistance to anti-VEGF strategies is complex and mechanisms include the upregulation of alternative proangiogenic signaling pathways (fibroblast growth factor [FGF], platelet-derived growth factor [PDGFR], c-Met). Several tyrosine kinase inhibitors (TKIs) under investigation in ovarian cancer target VEGF receptors as well as other proangiogenic molecules, eg, FGF: nintedanib, brivanib, dovitinib; PDGFR: cediranib, pazopanib; and c-Met: cabozantinib.
In addition to bevacizumab, there is now evidence for a role of VEGFR inhibitors in platinum-sensitive ovarian cancer. The ICON6 study evaluated the oral VEGFR inhibitor, cediranib, in platinum-sensitive relapsed ovarian cancer. Preliminary results were recently presented and showed an OS benefit with an antiangiogenic agent in relapsed ovarian cancer for the first time.49 In this Phase III trial, women who had relapsed more than 6 months following first-line platinum-based chemotherapy were randomized to either (three cohorts): platinum-based chemotherapy with placebo maintenance, concurrent cediranib (20 mg/day) during chemotherapy followed by placebo for up to 18 months, or concurrent cediranib followed by maintenance cediranib. A statistically significant improvement in OS of 2.7 months was seen in the concurrent/maintenance cediranib arm (17.6 to 20.3 months, HR: 0.70; P=0.0419). The benefit appears to be derived from the maintenance phase. The development of cediranib has temporarily ceased, and therefore the future of cediranib in ovarian cancer is unclear. In addition to bevacizumab, the VEGFR TKIs, pazopanib and nintedanib have shown significant activity in first-line Phase III trials. The ICON6 study results are encouraging and suggest a role for TKIs targeting the VEGF pathway in addition to a place for bevacizumab in recurrent ovarian cancer.
In addition to drugs targeting angiogenesis, poly ADP (adenosine diphosphate) ribose polymerase (PARP) inhibitors (eg, olaparib) which exploit DNA repair pathways, have also shown significant activity in platinum-sensitive ovarian cancer. A randomized, double-blind, placebo-controlled, Phase II study evaluated maintenance olaparib in patients with second or subsequent relapsed, platinum-sensitive, high-grade serous ovarian cancer who had achieved a response following their most recent platinum-based regimen.50 PFS was significantly prolonged with olaparib compared to the placebo arm (median 8.4 months vs 4.8 months; HR: 0.35, P<0.001) and the benefit was greatest in BRCA mutant patients (4.3 vs 11.2 months; HR: 0.18, P<0.00001). Phase III studies of PARP inhibitors in platinum-sensitive ovarian cancer are underway. The place for bevacizumab in platinum-sensitive ovarian cancer in light of the PARP inhibitor data is not clear. It is likely that patients with high-grade serous ovarian cancer will receive both VEGF-directed therapy and a PARP inhibitor at some point. Moreover, there is evidence to support combining inhibitors of the VEGF pathway with PARP inhibitors4 and this is an area under exploration.
Finally, as the management of ovarian cancer evolves to become more like a chronic disease, the long-term toxicities and QoL associated with antiangiogenic agents are increasingly important and approaches are required to facilitate the successful delivery of maintenance treatment in order for patients to derive the maximum benefit.
Conclusion
The addition of bevacizumab to the gemcitabine/carboplatin combination and continued until progression significantly improves PFS (median 12.4 vs 8.4 months; HR: 0.48) in the treatment of first platinum-sensitive relapsed ovarian cancer. This has led to EMA approval for this indication. In addition to bevacizumab, other agents targeting this pathway have also shown significant clinical activity in platinum-sensitive ovarian cancer and future trials should address the best strategy to use all these approaches in various settings (first-line, relapse [platinum-sensitive and resistant]) for the optimal benefit of our patients.
Acknowledgments
The Gynaecology Unit acknowledges support from the Royal Marsden NHS Foundation Trust and the Institute of Cancer Research National Institute of Health Research (NIHR) Biomedical Research Centre.
Footnotes
Disclosure
SB has received honoraria from Roche. CDP has no conflicts of interest.
References
- 1.Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61(2):69–90. doi: 10.3322/caac.20107. [DOI] [PubMed] [Google Scholar]
- 2.Sant M, Allemani C, Santaquilani M, Knijn A, Marchesi F, Capocaccia R, EUROCARE Working Group EUROCARE-4. Survival of cancer patients diagnosed in1995–1999. Results and commentary. Eur J Cancer. 2009;45(6):931–991. doi: 10.1016/j.ejca.2008.11.018. [DOI] [PubMed] [Google Scholar]
- 3.Gurung A, Hung T, Morin J, Gilks CB. Molecular abnormalities in ovarian carcinoma: clinical, morphological and therapeutic correlates. Histopathology. 2013;62(1):59–70. doi: 10.1111/his.12033. [DOI] [PubMed] [Google Scholar]
- 4.Banerjee S, Kaye SB. New strategies in the treatment of ovarian cancer: current clinical perspectives and future potential. Clin Cancer Res. 2013;19(5):961–968. doi: 10.1158/1078-0432.CCR-12-2243. [DOI] [PubMed] [Google Scholar]
- 5.Colombo N, Peiretti M, Parma G, et al. ESMO Guidelines Working Group Newly diagnosed and relapsed epithelial ovarian carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2010;21(Suppl 5):v23–v30. doi: 10.1093/annonc/mdq244. [DOI] [PubMed] [Google Scholar]
- 6.Bookman MA, Brady MF, McGuire WP, et al. Evaluation of new platinum-based treatment regimens in advanced-stage ovarian cancer: a Phase III Trial of the Gynecologic Cancer Intergroup. J Clin Oncol. 2009;27(9):1419–1425. doi: 10.1200/JCO.2008.19.1684. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Lambert HE, Rustin GJ, Gregory WM, Nelstrop AE. A randomized trial of five versus eight courses of cisplatin or carboplatin in advanced epithelial ovarian carcinoma. A North Thames Ovary Group Study. Ann Oncol. 1997;8(4):327–333. doi: 10.1023/a:1008256431090. [DOI] [PubMed] [Google Scholar]
- 8.Burger RA, Brady MF, Bookman MA, et al. Gynecologic Oncology Group Incorporation of bevacizumab in the primary treatment of ovarian cancer. N Engl J Med. 2011;365(26):2473–2483. doi: 10.1056/NEJMoa1104390. [DOI] [PubMed] [Google Scholar]
- 9.Perren TJ, Swart AM, Pfisterer J, et al. ICON7 Investigators A phase 3 trial of bevacizumab in ovarian cancer. N Engl J Med. 2011;365(26):2484–2496. doi: 10.1056/NEJMoa1103799. [DOI] [PubMed] [Google Scholar]
- 10.Armstrong DK, Bundy B, Wenzel L, et al. Gynecologic Oncology Group Intraperitoneal cisplatin and paclitaxel in ovarian cancer. N Engl J Med. 2006;354(1):34–43. doi: 10.1056/NEJMoa052985. [DOI] [PubMed] [Google Scholar]
- 11.Katsumata N, Yasuda M, Takahashi F, et al. Japanese Gynecologic Oncology Group Dose-dense paclitaxel once a week in combination with carboplatin every 3 weeks for advanced ovarian cancer: a phase 3, open-label, randomised controlled trial. Lancet. 2009;374(9698):1331–1338. doi: 10.1016/S0140-6736(09)61157-0. [DOI] [PubMed] [Google Scholar]
- 12.Gynecologic Oncology Group. Markman M, Blessing J, Rubin SC, Connor J, Hanjani P, Waggoner S. Phase II trial of weekly paclitaxel (80 mg/m2) in platinum and paclitaxel-resistant ovarian and primary peritoneal cancers: a Gynecologic Oncology Group study. Gynecol Oncol. 2006;101(3):436–440. doi: 10.1016/j.ygyno.2005.10.036. [DOI] [PubMed] [Google Scholar]
- 13.Gordon AN, Fleagle JT, Guthrie D, Parkin DE, Gore ME, Lacave AJ. Recurrent epithelial ovarian carcinoma: a randomized phase III study of pegylated liposomal doxorubicin versus topotecan. J Clin Oncol. 2001;19(14):3312–3322. doi: 10.1200/JCO.2001.19.14.3312. [DOI] [PubMed] [Google Scholar]
- 14.Parmar MK, Ledermann JA, Colombo N, et al. ICON and AGO Collaborators Paclitaxel plus platinum-based chemotherapy versus conventional platinum-based chemotherapy in women with relapsed ovarian cancer: the ICON4/AGO-OVAR-2.2 trial. Lancet. 2003;361(9375):2099–2106. doi: 10.1016/s0140-6736(03)13718-x. [DOI] [PubMed] [Google Scholar]
- 15.Pfisterer J, Plante M, Vergote I, et al. AGO-OVAR. NCIC CTG. EORTC GCG Gemcitabine plus carboplatin compared with carboplatin in patients with platinum-sensitive recurrent ovarian cancer: an intergroup trial of the AGO-OVAR, the NCIC CTG, and the EORTC GCG. J Clin Oncol. 2006;24(29):4699–4707. doi: 10.1200/JCO.2006.06.0913. [DOI] [PubMed] [Google Scholar]
- 16.Pujade-Lauraine E, Wagner U, Aavall-Lundqvist E, et al. Pegylated liposomal doxorubicin and carboplatin compared with paclitaxel and carboplatin for patients with platinum-sensitive ovarian cancer in late relapse. J Clin Oncol. 2010;28(20):3323–3329. doi: 10.1200/JCO.2009.25.7519. [DOI] [PubMed] [Google Scholar]
- 17.Gerber HP, Ferrara N. Pharmacology and pharmacodynamics of bevacizumab as monotherapy or in combination with cytotoxic therapy in preclinical studies. Cancer Res. 2005;65(3):671–680. [PubMed] [Google Scholar]
- 18.Saif MW. Anti-VEGF agents in metastatic colorectal cancer (mCRC): are they all alike? Cancer Manag Res. 2013;5:103–115. doi: 10.2147/CMAR.S45193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Spannuth WA, Sood AK, Coleman RL. Angiogenesis as a strategic target for ovarian cancer therapy. Nat Clin Pract Oncol. 2008;5(4):194–204. doi: 10.1038/ncponc1051. [DOI] [PubMed] [Google Scholar]
- 20.Presta LG, Chen H, O’Connor SJ, et al. Humanization of an anti-vascular endothelial growth factor monoclonal antibody for the therapy of solid tumors and other disorders. Cancer Res. 1997;57(20):4593–4599. [PubMed] [Google Scholar]
- 21.Kim KJ, Li B, Winer J, et al. Inhibition of vascular endothelial growth factor-induced angiogenesis suppresses tumour growth in vivo. Nature. 1993;362(6423):841–844. doi: 10.1038/362841a0. [DOI] [PubMed] [Google Scholar]
- 22.Melnyk O, Zimmerman M, Kim KJ, Shuman M. Neutralizing anti-vascular endothelial growth factor antibody inhibits further growth of established prostate cancer and metastases in a pre-clinical model. J Urol. 1999;161(3):960–963. [PubMed] [Google Scholar]
- 23.Warren RS, Yuan H, Matli MR, Gillett NA, Ferrara N. Regulation by vascular endothelial growth factor of human colon cancer tumorigenesis in a mouse model of experimental liver metastasis. J Clin Invest. 1995;95(4):1789–1797. doi: 10.1172/JCI117857. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Jain RK. Normalizing tumor vasculature with anti-angiogenic therapy: a new paradigm for combination therapy. Nat Med. 2001;7(9):987–989. doi: 10.1038/nm0901-987. [DOI] [PubMed] [Google Scholar]
- 25.FDA Approval for Bevacizumab [webpage on the Internet] Application number STN-125085/0. Clinical pharmacology/toxicology review. [Accessed April 8, 2014]. Available at: http://www.cancer.gov/cancertopics/druginfo/fda-bevacizumab.
- 26.Lin YS, Nguyen C, Mendoza JL, et al. Preclinical pharmacokinetics, interspecies scaling, and tissue distribution of a humanized monoclonal antibody against vascular endothelial growth factor. J Pharmacol Exp Ther. 1999;288(1):371–378. [PubMed] [Google Scholar]
- 27.Yanagisawa M, Yorozu K, Kurasawa M, et al. Bevacizumab improves the delivery and efficacy of paclitaxel. Anticancer Drugs. 2010;21(7):687–694. doi: 10.1097/CAD.0b013e32833b7598. [DOI] [PubMed] [Google Scholar]
- 28.Cooper BC, Ritchie JM, Broghammer CL, et al. Preoperative serum vascular endothelial growth factor levels: significance in ovarian cancer. Clin Cancer Res. 2002;8(10):3193–3197. [PubMed] [Google Scholar]
- 29.Hefler LA, Zeillinger R, Grimm C, et al. Preoperative serum vascular endothelial growth factor as a prognostic parameter in ovarian cancer. Gynecol Oncol. 2006;103(2):512–517. doi: 10.1016/j.ygyno.2006.03.058. [DOI] [PubMed] [Google Scholar]
- 30.Yamamoto S, Konishi I, Mandai M, et al. Expression of vascular endothelial growth factor (VEGF) in epithelial ovarian neoplasms: correlation with clinicopathology and patient survival, and analysis of serum VEGF levels. Br J Cancer. 1997;76(9):1221–1227. doi: 10.1038/bjc.1997.537. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Alvarez AA, Krigman HR, Whitaker RS, Dodge RK, Rodriguez GC. The prognostic significance of angiogenesis in epithelial ovarian carcinoma. Clin Cancer Res. 1999;5(3):587–591. [PubMed] [Google Scholar]
- 32.Yoneda J, Kuniyasu H, Crispens MA, Price JE, Bucana CD, Fidler IJ. Expression of angiogenesis-related genes and progression of human ovarian carcinomas in nude mice. J Natl Cancer Inst. 1998;90(6):447–454. doi: 10.1093/jnci/90.6.447. [DOI] [PubMed] [Google Scholar]
- 33.Oza AM, Perren TJ, Swart AM, et al. ICON7: Final overall survival results in the GCIG phase III randomized trial of bevacizumab in women with newly diagnosed ovarian cancer; European Cancer Congress 2013; September 27–October 1, 2013; Amsterdam, The Netherlands. Abstract 6. [Google Scholar]
- 34.Burger RA, Sill MW, Monk BJ, Greer BE, Sorosky JI. Phase II trial of bevacizumab in persistent or recurrent epithelial ovarian cancer or primary peritoneal cancer: a Gynecologic Oncology Group study. J Clin Oncol. 2007;25(33):5165–5171. doi: 10.1200/JCO.2007.11.5345. [DOI] [PubMed] [Google Scholar]
- 35.Garcia AA, Hirte H, Fleming G, et al. Phase II clinical trial of bevacizumab and low-dose metronomic oral cyclophosphamide in recurrent ovarian cancer: a trial of the California, Chicago, and Princess Margaret Hospital phase II consortia. J Clin Oncol. 2008;26(1):76–82. doi: 10.1200/JCO.2007.12.1939. [DOI] [PubMed] [Google Scholar]
- 36.Cannistra SA, Matulonis UA, Penson RT, et al. Phase II study of bevacizumab in patients with platinum-resistant ovarian cancer or peritoneal serous cancer. J Clin Oncol. 2007;25(33):5180–5186. doi: 10.1200/JCO.2007.12.0782. [DOI] [PubMed] [Google Scholar]
- 37.Nimeiri HS, Oza AM, Morgan RJ, et al. Chicago Phase II Consortium. PMH Phase II Consortium. California Phase II Consortium Efficacy and safety of bevacizumab plus erlotinib for patients with recurrent ovarian, primary peritoneal, and fallopian tube cancer: a trial of the Chicago, PMH, and California Phase II Consortia. Gynecol Oncol. 2008;110(1):49–55. doi: 10.1016/j.ygyno.2008.02.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Tillmanns TD, Lowe MP, Walker MS, Stepanski EJ, Schwartzberg LS. Phase II clinical trial of bevacizumab with albumin-bound paclitaxel in patients with recurrent, platinum-resistant primary epithelial ovarian or primary peritoneal carcinoma. Gynecol Oncol. 2013;128(2):221–228. doi: 10.1016/j.ygyno.2012.08.039. [DOI] [PubMed] [Google Scholar]
- 39.Wenham RM, Lapolla J, Lin HY, et al. A phase II trial of docetaxel and bevacizumab in recurrent ovarian cancer within 12 months of prior platinum-based chemotherapy. Gynecol Oncol. 2013;130(1):19–24. doi: 10.1016/j.ygyno.2013.04.049. [DOI] [PubMed] [Google Scholar]
- 40.Aghajanian C, Blank SV, Goff BA, et al. OCEANS: a randomized, double-blind, placebo-controlled phase III trial of chemotherapy with or without bevacizumab in patients with platinum-sensitive recurrent epithelial ovarian, primary peritoneal, or fallopian tube cancer. J Clin Oncol. 2012;30(17):2039–2045. doi: 10.1200/JCO.2012.42.0505. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.European Medicines Agency . Avastin: bevacizumab. London, UK: European Medicines Agency; [Accessed April 8, 2014]. Available at: http://www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/human/medicines/000582/human_med_000663.jsp&mid=WC0b01ac058001d124. [Google Scholar]
- 42.Miles D. Management of toxicity in patients receiving therapy with bevacizumab. EJC Supplements. 2008;6(6):29–39. [Google Scholar]
- 43.Bennouna J, Von Pawel J, Zatloukal P, et al. Oral management of hypertension (HTN) in patients with advanced or recurrent non-squamous non-small cell lung cancer (NSCLC) receiving first-line cisplatin and gemcitabine with bevacizumab or placebo – results from randomised phase III trial BO17704. Eur J Cancer Suppl. 2007;5(4):359. [Google Scholar]
- 44.Kozloff M, Hainsworth J, Badarinath S, et al. Management of hypertension in patients with metastatic colorectal cancer treated with bevacizumab plus chemotherapy. Eur J Cancer Suppl. 2007;5(4):250. [Google Scholar]
- 45.Dincer M, Altundag K. Angiotensin-converting enzyme inhibitors for bevacizumab-induced hypertension. Ann Pharmacother. 2006;40(12):2278–2279. doi: 10.1345/aph.1H244. [DOI] [PubMed] [Google Scholar]
- 46.Stark D, Nankivell M, Pujade-Lauraine E, et al. Standard chemotherapy with or without bevacizumab in advanced ovarian cancer: quality-of-life outcomes from the International Collaboration on Ovarian Neoplasms (ICON7) phase 3 randomised trial. Lancet Oncol. 2013;14(3):236–243. doi: 10.1016/S1470-2045(12)70567-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Monk BJ, Huang HQ, Burger RA, et al. Patient reported outcomes of a randomized, placebo-controlled trial of bevacizumab in the front-line treatment of ovarian cancer: a Gynecologic Oncology Group Study. Gynecol Oncol. 2013;128(3):573–578. doi: 10.1016/j.ygyno.2012.11.038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Poveda A, Selle F, Hilpert F, et al. Weekly paclitaxel (PAC), pegylated liposomal doxorubicin (PLD) or topotecan (TOP) ± bevacizumab (BEV) in platinum (PT)-resistant recurrent ovarian cancer (OC): analysis by chemotherapy (CT) cohort in the GCIG AURELIA randomised phase III trial; European Society for Medical Oncology Congress 2012; September 28–October 2, 2012; Vienna, Austria. Abstract LBA26. [Google Scholar]
- 49.Ledermann JA, Perren TJ, Raja FA, et al. Randomised double-blind phase III trial of cediranib (AZD 2171) in relapsed platinum sensitive ovarian cancer: Results of the ICON6 trial; European Society for Medical Oncology Congress 2013; September 27–October 1, 2013; Amsterdam, The Netherlands. Abstract 10. [Google Scholar]
- 50.Ledermann J, Harter P, Gourley C, et al. Olaparib maintenance therapy in platinum-sensitive relapsed ovarian cancer. N Engl J Med. 2012;366(15):1382–1392. doi: 10.1056/NEJMoa1105535. [DOI] [PubMed] [Google Scholar]