

Abstract
Objective:
Indwelling transurethral catheter is frequently used after gynecological surgeries in order to prevent urinary retention. There is controversy about the ideal time to remove the catheter after surgery. This randomized controlled study was undertaken to determine whether the immediate removal of urinary catheter after abdominal hysterectomy affects the rate of symptomatic urinary tract infection (UTI), recatheterization, subjective pain perception and febrile morbidity.
Study Design:
This prospective randomized controlled trial included 70 women undergoing abdominal hysterectomy with or without salpingoophrectomy for benign diseases. Patients were divided into two equal groups on the basis of timing of removal of urinary catheter (Group I — Immediate removal after surgery, Group II — Removal after 24 h and evaluated for benefits versus risks of immediate catheter removal. The results were compared by the Chi-square test.
Results:
Recatheterization was required in three patients of immediate removal group and none in late removal group (P = 0.07). Higher incidence of positive urine cultures (25.9%) and febrile morbidity (10%) was found in Group II when compared to immediate removal group (8%). Pain perception was not statistically different in both groups (P = 0.567).
Conclusions:
The early removal of an indwelling catheter after surgery was not associated with an increased rate of febrile events, UTI. Pain perception was also lower in early removal group. Although need of recatheterization was higher in early removal group, but not statistically significant.
Keywords: Catheterization, febrile morbidity, indwelling bladder catheter, post abdominal hysterectomy, urinary tract infections
INTRODUCTION
Traditionally, urinary catheter has been used in gynecological surgical practice to assess urinary output, to improve surgical exposure, reduce the possibility of injury to the urinary system and to prevent postoperative urinary retention. [1] However, catheterization is mainly required to keep the bladder out of the operative site and later on until patient becomes ambulatory. Shortest duration of the catheter is now a routine and unlike cesarean infection rate is much low even if kept for 24-48 h. Although there seems to be no clinical uncertainty about the need for an empty bladder before and during surgery, controversy arises about the ideal time to remove the catheter postoperatively. [2] Few studies reported significantly less pain and urinary tract infection (UTI) in after immediate removal, whereas others showed that early removal urinary catheter after uncomplicated hysterectomy seem to decrease first ambulation time and hospital stay without posing any threats. [2,3,4,5,6,7,8]
MATERIALS AND METHODS
This prospective, randomized controlled trial was conducted in the Department of Obstetrics and Gynecology of a tertiary care referral center from July 2008 to December 2009. The aim of this study was to compare the outcomes of immediate removal of urinary catheter versus removal on the first day after abdominal hysterectomy for benign gynecological disease. Informed consent was obtained from enrolled patients and protocol was approved by the Institute's Ethical Committee. Seventy patients who underwent an uneventful abdominal hysterectomy with or without salpingoophrectomy were included in this study. Patients with anticipated complicated surgical procedure requiring strict fluid replacement postoperatively, bladder suspension or colporraphy surgery, positive or unavailable preoperative urine culture report and co-morbid illness requiring strict intake output monitoring were excluded from the study.
Randomization
Group I Immediate removal of the catheter in the operating room.
Group II Catheter removal after 24 h.
Randomization was performed by using a computer generated randomization table and allocation group was kept in sealed envelope. The operating surgeon was made aware of randomization and accordingly the patient was assigned to one of the two groups. In all cases, the envelope was opened at the end of the surgical procedure. All patients received one dose of antibiotic prophylaxis at the time of surgery and continued postoperatively as per department protocol. Standard 16F Foley's catheter with 10 cc balloon was used. A fresh catheter sample was taken for the urine microscopy and culture at the time of preoperative catheterization. Catheter was kept for the duration of surgical procedure. Later, on the basis of study assignment, catheter was removed either in the operating room immediately or 24 h postoperative. Type of anesthesia, amount of blood loss, duration of surgery was noted.
Incidence of symptomatic UTIs, re-catheterization, subjective pain assessment and febrile morbidity was compared in both groups.
Pain was assessed with a pictorial questionnaire that assed the level of pain and location of pain, that is, bladder or urethra versus surgical site. The questionnaires were site specific for the pain. All patients were given same analgesia in the postoperative period.
Febrile morbidity was defined as two consecutive oral temperatures of >100.4°F measured 6 h apart.
After urinary catheter removal, patients were asked to void spontaneously. Need of recatheterization was assessed by an inability to pass urine at the end of 12 h, or failure to void after two attempts.
The diagnosis of symptomatic UTI was based on the presence of significant bacteriuria accompanied by at least one of the following symptoms: Fever, dysuria, increased frequency of urination, urinary urgency, suprapubic pain, and burning micturition.
A clear voided midstream urine specimen was obtained on. The second postoperative day for culture and sensitivity. A second clean voided midstream urine sample for culture and sensitivity was obtained at 2 week postoperative visit. All the culture sensitivity reports were collected, recorded and patients with positive culture were treated according to the sensitivity.
Statistical analysis
Groups were compared by the Chi-square test. A P < 0.05 was considered to be statistically significant.
RESULTS
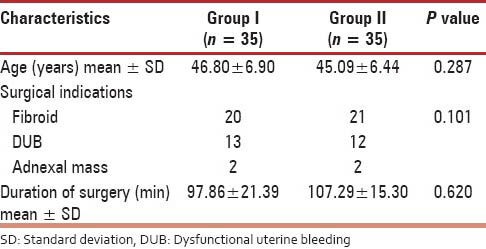
A total of 70 women were enrolled in the study and equally assigned to two groups. All women had similar clinical characteristics, that is, age, indication for hysterectomy and duration of surgery [Table 1].
Table 1.
Distribution according to clinical characteristics
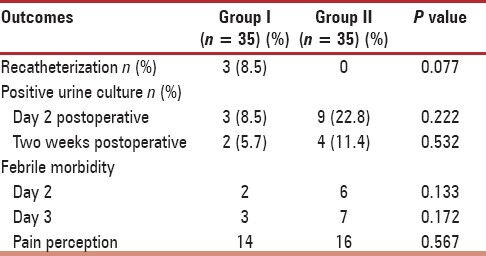
Of 35 women only 3 (8.5%) required recatheterization after immediate postoperative removal, while no one from late removal group needed to be recatheterized. Twelve women had positive culture at day 2 postoperative out of which nine were from late removal group as compared to three patients of early removal group (P = 0.222). Of 12 culture positive most common organism was Escherichia coli. None of these had repeat culture positive at 2 weeks. Out of six culture positive cases at 2 weeks postoperative day, two women were from early removal group and four women from late removal group (P = 0.532).
Pain perception was also higher in late removal group (45.7%) as compared to early group (40%). Out of eight febrile patients on day 2 postoperative six patients were from Group II while the rest were from Group I (P = 0.133) and on day 3 postoperative day seven patient from late removal group were febrile when compared to three women of early removal group [Table 2].
Table 2.
Results
Three women out of nine culture positive cases in late removal group had symptoms of UTI and fever. None was symptomatic in early removal group. One women at 2 weeks who was positive for culture had a fever and other symptoms of UTI.
DISCUSSION
Abdominal hysterectomy for dysfunctional uterine bleeding is now becoming rare as vaginal hysterectomy and total laparoscopic hysterectomy or laparoscopy-assisted vaginal hysterectomy has taken a lead role. UTIs comprise of all nosocomial infections and occur after urological instrumentation, usually urinary catheterization, in up to 75% of the patients. [2,3,4,5] The potential squeal of urinary catheterization include gram negative bacteremia, antimicrobial toxicity, chronic bacteriuria and chronic renal disease. [6] With today's heightened awareness of costs of medical care a nosocomial infection causing increased length of hospital stay would not only be a significantly morbid event, but also an economic consideration.
Hemantha Senanayka from Colombo showed that elective cesarean in 344 women without catheterization does not compromise the safety or ease of surgery. [9] It reduces the risk of infection.
A prospective randomized control trial conducted on 200 women by Onile et al. showed that immediate removal of catheter after cesarean is associated with a lower rate of UTI. [10]
Various prospective trials have been conducted in other urogenital surgeries regarding early removal of the catheter. A prospective randomized study conducted on 90 women by Sekhavat et al. [11] in anterior colporraphy showed that symptomatic UTI was significantly lower in early catheter-removal group; also patients in this group reported significantly less pain and voiding disturbances.
This study demonstrated that the immediate removal of an in-dwelling catheter is safe and not associated with adverse effects. One interesting finding was that only three women in the early catheter-removal group required recatheterization after failing to void and none of these women had positive urine culture. We are aware that a possible criticism to our findings may lie in the fact that number of patients was limited. Although our findings are strengthened by the fact the surgeon was made aware of the randomization only at the end of the operation, but, a limitation of our study may exist in the fact that the observer of outcome was not blinded to the randomization.
However, it seems unlikely that the parameters evaluated in the study (rate of recatheterization, symptomatic UTIs, fever) were biased by the observer, considering that they were determined on the basis of standardized criteria. Pain perception is a subjective measure, which could result in variations of perceived pain.
CONCLUSION
Early catheter removal after abdominal hysterectomy was associated with a lower incidence of positive urine culture. Furthermore, there was no adverse outcome like significant rate of recatheterization and higher pain perception.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Ghoreishi J. Indwelling urinary catheters in cesarean delivery. Int J Gynaecol Obstet. 2003;83:267–70. doi: 10.1016/s0020-7292(03)00144-9. [DOI] [PubMed] [Google Scholar]
- 2.Fernandez R, Griffiths R, Murie P. Comparison of late night and early removal of short-term urethral catheters. Joanna Briggs Inst Rep. 2003;1:1–16. [PubMed] [Google Scholar]
- 3.Dunn TS, Shlay J, Forshner D. Are in-dwelling catheters necessary for 24 hours after hysterectomy? Am J Obstet Gynecol. 2003;189:435–7. doi: 10.1067/s0002-9378(03)00496-4. [DOI] [PubMed] [Google Scholar]
- 4.Schiøtz HA, Tanbo TG. Postoperative voiding, bacteriuria and urinary tract infection with Foley catheterization after gynecological surgery. Acta Obstet Gynecol Scand. 2006;85:476–81. doi: 10.1080/00016340500409877. [DOI] [PubMed] [Google Scholar]
- 5.Alessandri F, Mistrangelo E. A prospective, randomized trial comparing immediate versus delayed catheter removal following hysterectomy. Obstet Gynecol Surv. 2006;61:578–9. doi: 10.1080/00016340600606976. [DOI] [PubMed] [Google Scholar]
- 6.Griffiths RD, Fernandez RS, Murie P. Removal of short-term indwelling urethral catheters: The evidence. J Wound Ostomy Continence Nurs. 2004;31:299–308. doi: 10.1097/00152192-200409000-00013. [DOI] [PubMed] [Google Scholar]
- 7.Fernandez R, Griffiths R, Murie P. Comparison of late night and early morning removal of short-term urethral catheters. Int J Evid Based Healthc. 2003;1:1–16. [PubMed] [Google Scholar]
- 8.Alessandri F, Mistrangelo E, Lijoi D, Ferrero S, Ragni N. A prospective, randomized trial comparing immediate versus delayed catheter removal following hysterectomy. Acta Obstet Gynecol Scand. 2006;85:716–20. doi: 10.1080/00016340600606976. [DOI] [PubMed] [Google Scholar]
- 9.Senanayake H. Elective cesarean section without urethral catheterization. J Obstet Gynaecol Res. 2005;31:32–7. doi: 10.1111/j.1447-0756.2005.00237.x. [DOI] [PubMed] [Google Scholar]
- 10.Onile TG, Kuti O, Orji EO, Ogunniyi SO. A prospective randomized clinical trial of urethral catheter removal following elective cesarean delivery. Int J Gynaecol Obstet. 2008;102:267–70. doi: 10.1016/j.ijgo.2008.04.020. [DOI] [PubMed] [Google Scholar]
- 11.Sekhavat L, Farajkhoda T, Davar R. The effect of early removal of indwelling urinary catheter on postoperative urinary complications in anterior colporrhaphy surgery. Aust N Z J Obstet Gynaecol. 2008;48:348–52. doi: 10.1111/j.1479-828X.2008.00842.x. [DOI] [PubMed] [Google Scholar]