

Abstract
Background:
There are several studies about the positive relation between physical inactivity or low cardio respiratory fitness with development of metabolic syndrome (MS). In contrast, physical activity had favourable effects on all components of MS but the quantity and the frequency of physical activity necessary to produce this beneficial effect has not been defined as yet. The aim of this survey was to study the association of regular physical activity, measured by patient's estimation of walking time per day, with MS.
Materials and Methods:
This cross-sectional study was conducted as a part of Isfahan Healthy Heart Program (IHHP). Persons who had no component of MS were considered as reference group. Demographic data were collected by questionnaire. Relation between walking time and MS was evaluated by using logistic regression adjusted by age, sex, socioeconomic status (SES), life style and food item.
Results:
The study populations consisted of 4151 persons. Lower physical activity was associated with higher prevalence of MS (P < 0.001). There was a negative relation between the usual daily walking time and MS. Adjusted odds ratio for age groups, sex, SES, life style and food items (fat and oil, sweet and sweet drink, rice and bread, fried food) revealed that MS decreases with increasing walking time (P < 0.05) [OR = 0.70 (0.52-0.94)].
Conclusion:
Total daily walking time is negatively associated with MS and increasing daily walking time is an effective way for preventing MS.
Keywords: Dietary behaviour, physical activity, walking
INTRODUCTION
Metabolic syndrome (MS) is a clustering of cardiovascular risk factors represented by high blood pressure, overweight/obesity, hypertriglyceridemia, low high-density lipoprotein-cholesterol (HDL-C), and glucose intolerance.1
The diagnosis of MS in adults, and recently in children and adolescents, is established when three or more of the five individual elements exist together in the same subject.[1,2]
MS comprises a major risk for chronic diseases and in association with rising childhood obesity, and a sedentary lifestyle, is rapidly increasing in prevalence.3 It is reported that up to 47.2% of the Iranian population had sedentary lifestyle.4 It is estimated that 21.9% of Iranian adults living in central Iran have MS.5
Coronary heart disease is the leading cause of death in industrialised countries and is rapidly becoming a primary cause of death worldwide.6 In adults, MS is associated with a significantly elevated risk of coronary heart disease.7
Physical activity helps to promote a healthful body composition, maintain muscle mass and thus preserve the resting metabolic rate.8,9
Physical activity and fitness are associated with a lower incidence of morbidity and mortality from a number of chronic diseases, including cardiovascular diseases (CVDs), diabetes and obesity.10,11
There is a substantial body of evidence associating physical inactivity or low cardio respiratory fitness with the development of MS in adults.12,13 In contrast, physical activity has favourable effects on all components of the MS and on the resulting cardiovascular risk.14
Walking is the most common physical activity among adults,6,15 and an accessible form of moderate physical activity particularly relevant for the obese, which are less likely to perform vigorous physical activity.
The quantity and the frequency of physical activity necessary to produce beneficial effects has not been defined as yet, but brisk walking is considered particularly appropriate, as it can be practiced by a large number of individuals, without any additional cost, and has a low rate of injury.16 In one study on hypertensive patients, walking and running produce similar reductions in mortality.17
In this study, walking with intensity, which is usual in daily activity, was evaluated in relation to MS in a sample of Iranian population. The programme began in 2000-2001 and its third phase was done in 2007.18,19 It is a quasi-experimental trial that includes a reference area and several levels of evaluation including process, impact and outcome evaluations. IHHP involves individual, community and environmental changes to support health behaviour modification.20,21
MATERIALS AND METHODS
This was a cross-sectional study of the Isfahan Healthy Heart Program (IHHP).
IHHP is a comprehensive integrated community based programme for CVD prevention and control among adults via reducing CVD risk factors and improvement of cardiovascular healthy behaviours.
The IHHP evaluation included four annual independent sample surveys in four specific sub-groups (adults, adolescents, health professionals and individuals at high risk for non-communicable disease) in both intervention and reference areas. In each community, a random sample of adults was selected yearly by multi-stage cluster sampling.
MS was defined as subjects who had three or more of the following criteria as defined by the National Cholesterol Education Program:1 (1) Central obesity as the waist circumference (WC) >102 cm in men and >88 cm in women; (2) Fasting plasma triglycerides ≥150 mg/dl; (3) low HDL-C with fasting HDL-C <40 mg/dl in men and <50 mg/dl in women; (4) hypertension with systolic blood pressure ≥130 mmHg and/or diastolic blood pressure 85 mmHg and/or anti-hypertensive agents and (5) hyperglycaemia with fasting plasma glucose ≥100 mg/dl and/or hypoglycaemic medications.
A total of 2196 persons who had no components of MS were considered as the reference group.
The data were collected using validated questionnaires.6,15,16,18,19,20 Physical activity was assessed by Baecke questionnaire. Walking time was estimated by participants. Walking time is composed of two components, leisure walking time and transfer walking time; in this study, the sum of these two components was considered as walking time. The weight measured by a Seca scale, and WC was measured at the part of the trunk located midway between the lower costal margin (bottom of the lower rib) and the iliac crest (top of the pelvic bone). Body mass index (BMI) was calculated as weight/height2 (kg/m2). Blood pressure was measured twice on the right arm, in sitting position and after 15 minutes rest. The mean of two recordings was recorded. The first and fifth Korokov's sounds were considered as systolic and diastolic blood pressure, respectively. To measure blood sugar and lipid profile (cholesterol, triglyceride, HDL and low-density lipoprotein (LDL)), approximately 10 ml of blood sample was taken from participants after an overnight fast.
Statistical analysis
The demographic and baseline data of two groups were compared by chi-square and t-test. Walking time was divided in to the 4 quartiles. The prevalence for each component of MS was calculated by chi-square and analysis of variance (ANOVA) tests were used to compare the means. The relations between walking-duration quartiles and MS were analysed by logistic regression test. To test for linear trend and determine P-value for trend across quartile of walking, we assigned the median walking time to individual's variable as continuous variable in logistic regression for >=3 component vs. 0 component. The results are adjusted by age, sex, socioeconomic status (SES), life style and food items (fat and oil, sweet and sweet drink, rice and bread, fried food). The effect of BMI is also adjusted in the last model.
RESULTS
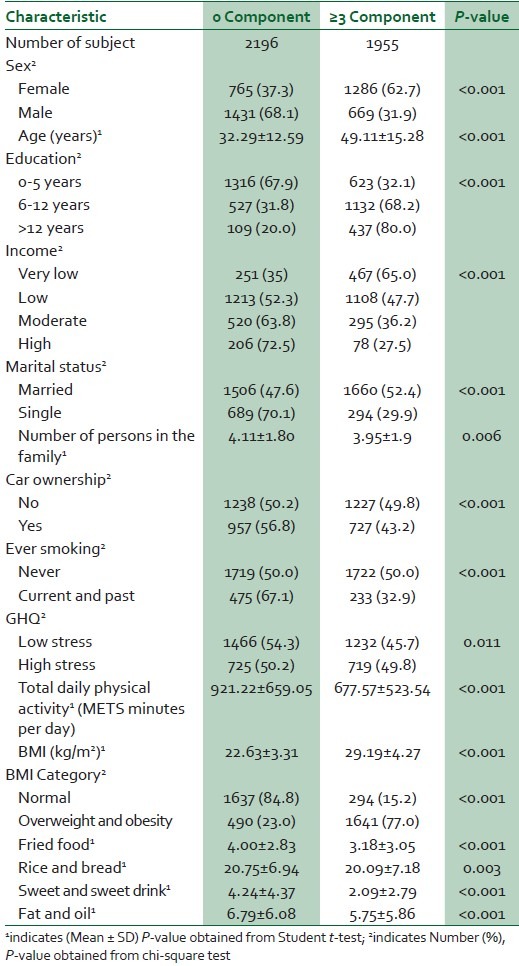
The study population was 4151 persons with a mean age of 40.21 ± 16.26 years (49.4% female and 50.6% male). The basic characteristics of participants are shown in [Table 1]. MS is more prevalent in women than in men (62.7% vs. 31.9%) (P < 0.001). It is also more prevalent in people who are in lower economic status (65% vs. 27.5%) (P < 0.001). MS prevalence is higher in persons with higher stress score and in people who had lower daily physical activity (P < 0.001).
Table 1.
Basic characteristics of the study population
In [Table 2], mean and prevalence of MS components, among quartile of walking time are shown. WC, fasting blood glucose, LDL and total cholesterol all are negatively associated with increasing walking time (P < 0.001). The results of logistic regression test for relation between MS and walking duration are shown in [Table 3].
Table 2.
Mean and prevalence of the components of metabolic syndrome in study participants among quartile of walking time
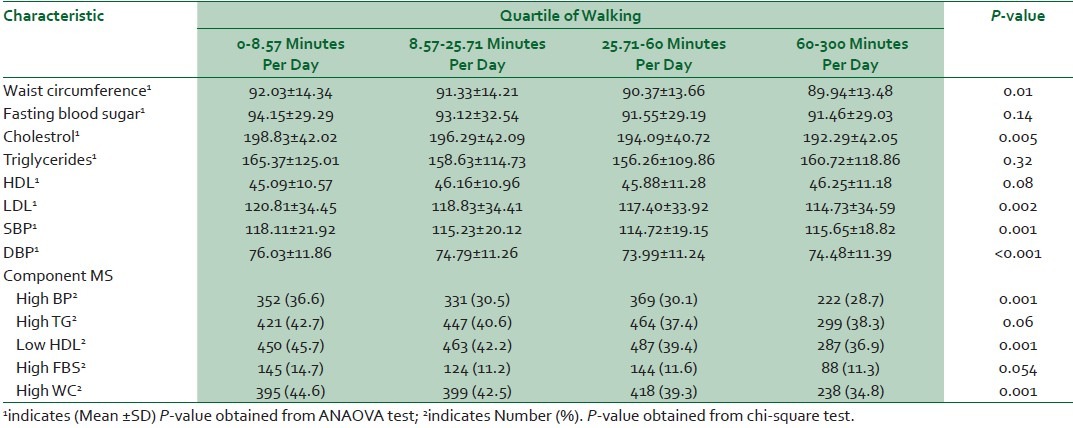
Table 3.
Crude and adjusted odds ratios (95% CI) for metabolic syndrome vs. no elevated component of MS among quartiles of walking time
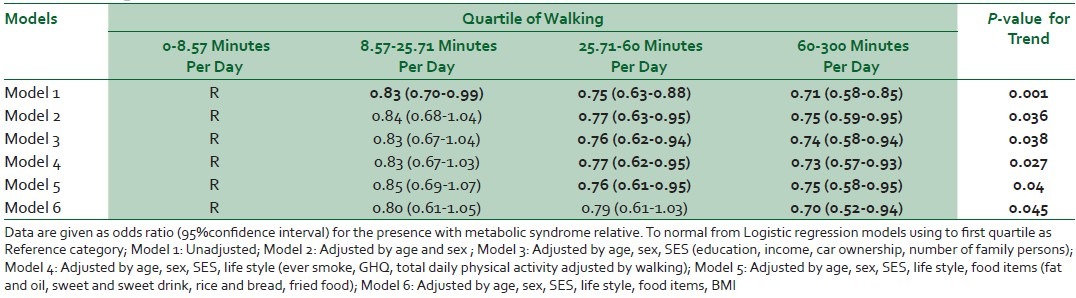
In all models, the odds ratio of MS decreases with increasing walking time (P < 0.05).
In Model 1, ‘logistic regression without adjustment’ the odds ratio for existing MS in persons with usual walking time between 60 and 300 minutes/day is 0.71, which means that this level of daily walking time decreases the probability of occurrence of MS by about 29%. In model 6, ‘adjusting for age, sex, SES, life style, food items and BMI’ the odd ratio changes only 1%, this means that these factors had a trivial effect on the relation between daily walking time and MS.
DISCUSSION
Regular physical activity is an important protective factor against several diseases, such as obesity, hypertension, type II diabetes3,18 and MS.19 In a cross-sectional school-based study on 417 adolescents (243 girls) aged 15-18 years from the Azorean Islands, Portugal, daily step counts and physical activity levels were negatively associated with having one or more metabolic risk factors.22 In another study on 456 adolescents in Brazil, the inactive adolescents and the adolescents with low cardio respiratory fitness had higher prevalence of MS; there was no difference with respect to gender.23
In the Woolf study on 207 adult women (20-70 years), significant inverse correlations were found between activity (steps per day) and BMI, insulin level, CRP concentration, leptin level, WC and body fat, glucose levels, CRP concentration, WC and body fat.24
In our study, lower physical activity was associated with higher prevalence of MS (P < 0.001).
In the Woolf study, with increasing age (from 30 to70 years) in women, the incidence of MS components increases. The relation between physical activity and MS components is also more prominent in younger women.24
Kim et al., from Japan, reported that the risk for MS among physically inactive men was significantly higher than that for physically active men after adjustment for age, sedentary time, low intensity activity, smoking, calorie intake and BMI. In contrast, the risk for MS in women was not significantly different between physically active and physically inactive women after adjustment for age, sedentary time, low intensity activity, smoking, calorie intake, BMI and menopausal status.25 In our study, the age and sex had a small effect (>4%) on risk of having MS for patients with low physical activity.
Regarding the mentioned studies, the age and sex in different region of world may have different impact on relation between physical activity and MS. This may be related to daily level of physical activity, daily calorie intake, daily stresses and other measures of life style. In our study, it was a negative association between MS and self-reported walking time in adults aged 19-55 years, regarding high prevalence of sedentary life in the Iranian population (47.2%),4 replacing daily activity with activity that increase the usual daily walking time would decrease the incidence of MS in this population.
The main limitation of our study was estimation of walking time by participants, hence this variable depends on patient cooperation. Also this study was cross-sectional and these kinds of studies are weak for evaluation of relations between variables.
CONCLUSION
In individual adults aged 19-55 years, daily estimated walking time is negatively associated with MS. This indicates that a mild physical activity such as regular daily walking is an effective way of preventing metabolic syndrome in the adult population.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III): Executive summary of the third report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, ad Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) JAMA. 2001;285:2486–97. doi: 10.1001/jama.285.19.2486. [DOI] [PubMed] [Google Scholar]
- 2.Ford ES, Li C. Defining the metabolic syndrome in children and adolescents: Will the real definition please stand up? J Pedriatr. 2008;152:160–4. doi: 10.1016/j.jpeds.2007.07.056. [DOI] [PubMed] [Google Scholar]
- 3.Kohen-Avramoglu R, Theriault A, Adeli K. Emergence of the metabolic syndrome in childhood: An epidemiological overview and mechanistic link to dyslipidemia. Clin Biochem. 2003;36:413–20. doi: 10.1016/s0009-9120(03)00038-9. [DOI] [PubMed] [Google Scholar]
- 4.Shirani S, Heidari K, Sabzghabaee AM, Mirmoghtadaee P, Hoseini L, Aalifar H, et al. The modifiable noncommunicable risk factors among an Iranian population. Southeast Asian J Trop Med Public Health. 2012;43:1227–32. [PubMed] [Google Scholar]
- 5.Gharipour M, Kelishadi R, Baghaie AM, Boshtam M, Rabeie K. Prevalence of metabolic syndrome in an Iranian adult population. ARYA J. 2005;1:188–92. [Google Scholar]
- 6.Hu FB, Willett WC. Optimal diets for prevention of coronary heart disease. JAMA. 2002;288:2569–78. doi: 10.1001/jama.288.20.2569. [DOI] [PubMed] [Google Scholar]
- 7.Hitsumoto T, Makahashi M, Iizuka T, Shirai K. Relationship between metabolic syndrome and early stage coronary atherosclerosis. J Atheroscler Thromb. 2007;14:294–302. doi: 10.5551/jat.e506. [DOI] [PubMed] [Google Scholar]
- 8.Hu FB, Li TY, Colditz GA, Willett WC, Manson JE. Television watching and other sedentary behaviors in relation to risk of obesity and type 2 diabetes mellitus in women. JAMA. 2003;289:1785–91. doi: 10.1001/jama.289.14.1785. [DOI] [PubMed] [Google Scholar]
- 9.Van Pelt RE, Jones PP, Davy KP, Desouza CA, Tanaka H, Davy BM, et al. Regular exercise and the age-related decline in resting metabolic rate in women. J Clin Endocrinol Metab. 1997;82:3208–12. doi: 10.1210/jcem.82.10.4268. [DOI] [PubMed] [Google Scholar]
- 10.Blair SN, Horton E, Leon AS, Lee IM, Drinkwater BL, Dishman RK, et al. Physical activity, nutrition, and chronic disease. Med Sci Sports Exerc. 1996;28:335–49. doi: 10.1097/00005768-199603000-00009. [DOI] [PubMed] [Google Scholar]
- 11.Warburton DE, Nicol CW, Bredin SS. Health benefits of physical activity: The evidence. CMAJ. 2006;174:801–9. doi: 10.1503/cmaj.051351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Erikson J, Taimela S, Koivisto VA. Exercise and the metabolic syndrome. Diabetologia. 1997;40:125–35. doi: 10.1007/s001250050653. [DOI] [PubMed] [Google Scholar]
- 13.Kullo IJ, Hensrud DD, Allison TG. Relation of low cardiorespiratory fitness to the metabolic syndrome in middle-aged men. Am J Cardiol. 2002;90:795–7. doi: 10.1016/s0002-9149(02)02617-6. [DOI] [PubMed] [Google Scholar]
- 14.Montesi L, Moscatiello S, Malavolti M, Marzocchi R, Marchesini G. Physical activity for the prevention and treatment of metabolic disorders. Intern Emerg Med. 2013 doi: 10.1007/s11739-013-0953-7. [DOI] [PubMed] [Google Scholar]
- 15.Siegel PZ, Brackbill RM, Heath GW. The epidemiology of walking for exercise: Implications for promoting activity among sedentary groups. Am J Public Health. 1995;85:706–10. doi: 10.2105/ajph.85.5.706. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Eyler AA, Brownson RC, Bacak SJ, Housemann RA. The epidemiology of walking for physical activity in the United States. Med Sci Sports Exerc. 2003;35:1529–36. doi: 10.1249/01.MSS.0000084622.39122.0C. [DOI] [PubMed] [Google Scholar]
- 17.Williams PT. Walking and running produce similar reductions in cause-specific disease mortality in hypertensives. Hypertension. 2013;62:485–91. doi: 10.1161/HYPERTENSIONAHA.113.01608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Sarraf-Zadegan N, Sadri G, Malek AH, Baghaei M, Mohammadi FN, Shahrokhi S, et al. Isfahan Healthy Heart Programme: A comprehensive integrated community-based programme for cardiovascular disease prevention and control. Design, methods and initial experience. Acta Cardiol. 2003;58:309–20. doi: 10.2143/AC.58.4.2005288. [DOI] [PubMed] [Google Scholar]
- 19.Kelishadi R, Sarrafzadegan N, Sadri GH. Short-term results of a community-based program on promoting healthy lifestyle for prevention and control of chronic diseases in a developing country setting: Isfahan Healthy Heart Program. Asia Pac J Public Health. 2011;23:518–33. doi: 10.1177/1010539509348241. [DOI] [PubMed] [Google Scholar]
- 20.Rabiei K, Kelishadi R, Sarrafzadegan N, Abedi HA, Alavi M, Heidari K, et al. Process evaluation of a community-based program for prevention and control of non-communicable disease in a developing country: The Isfahan Healthy Heart Program, Iran. BMC Public Health. 2009;9:57. doi: 10.1186/1471-2458-9-57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Sarrafzadegan N, Kelishadi R, Esmaillzadeh A, Mohammadifard N, Rabiei K, Roohafza H, et al. Do lifestyle interventions work in developing countries. Findings from the Isfahan Healthy Heart Program in the Islamic Republic of Iran? Bull World Health Organ. 2009;87:39–50. doi: 10.2471/BLT.07.049841. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Moreira C, Santos R, de Farias Júnior JC, Vale S, Santos PC, Soares-Miranda L, et al. Metabolic risk factors, physical activity and physical fitness in azorean adolescents: A cross-sectional study. BMC Public Health. 2011;11:214. doi: 10.1186/1471-2458-11-214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Stabelini Neto A, Sasaki JE, Mascarenhas LP, Boguszewski MC, Bozza R, Ulbrich AZ, et al. Physical activity, cardiorespiratory fitness, and metabolic syndrome in adolescents: A cross-sectional study. BMC Public Health. 2011;11:674. doi: 10.1186/1471-2458-11-674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Woolf K, Reese CE, Mason MP, Beaird LC, Tudor-Locke C, Vaughan LA. Physical activity is associated with risk factors for chronic disease across adult women's life cycle. J Am Diet Assoc. 2008;108:948–59. doi: 10.1016/j.jada.2008.03.015. [DOI] [PubMed] [Google Scholar]
- 25.Kim J, Tanabe K, Yokoyama N, Zempo H, Kuno S. Association between physical activity and metabolic syndrome in middle-aged Japanese: A cross-sectional study. BMC Public Health. 2011;11:624. doi: 10.1186/1471-2458-11-624. [DOI] [PMC free article] [PubMed] [Google Scholar]