

Abstract
Background:
Coronary artery disease (CAD) mostly occurs in persons older than 45 years of age. In India, CAD manifests almost a decade earlier than in Western countries. This study was done to study the risk factors and angiographic profile in young patients presenting with acute myocardial infarction (AMI).
Patients and Methods:
One hundred and twenty four consecutive patients presenting with AMI at less than 40 years of age were studied for risk factors. Coronary angiography was done in all.
Results:
Out of 124 patients, 123 were male. Mean age was 35.94 ± yrs. One hundred and eighteen had ST elevation myocardial infarction (MI) (95.16%) and six had non ST elevation MI (5.84%). Anterior wall MI was present in 88 patients (70.97%), inferior wall MI in 31 patients (25%) and lateral wall MI in five patients (4.03%). Seventy three patients (58.8%) were smoker, 55 were hypertensive (44.35%), 10 were diabetic (8.06%). Family history of CAD was present in 22 (17.7%) patients. Low High-density lipoprotein (HDL) was seen in 53 patients (42.7%), and high triglycerides in 60 patients (48.38%). Significant CAD was found in 88 (70.96%) patients, 13 (10.48%) had normal coronaries. Single vessel disease was seen in 57 patients, two-vessel disease in 15 patients and three-vessel disease in eight patients. Total 125 lesions were seen and left anterior descending (LAD) was the commonest vessel involved, with 78 lesions (62.4%).
Conclusion:
AMI in young almost exclusively occurs in male, and ST elevation MI is the main presentation. Anterior wall MI is most common, with LAD being involved in around 2/3 patients. Smoking, hypertension, low HDL and high triglycerides are the major risk factors.
Keywords: Coronary artery disease, myocardial infarction, risk factors
INTRODUCTION
Coronary heart disease (CHD) is the leading cause of death in the West. Acute myocardial infarction (AMI) among young is relatively uncommon. Still, it is an important problem for the patient and the treating physician, as these patients have different risk factors, clinical presentation and prognosis than the older patients. There are few studies of risk factor profile and pattern of coronary artery involvement in AMI in young, so the purpose of the study.
MATERIALS AND METHODS
One hundred and twenty four consecutive patients of less than 40 years and above 18 yrs presenting with AMI were studied for the conventional risk factors.
AMI was defined as typical rise and fall of cardiac markers of myocardial necrosis with at least one of the following:
Ischaemic symptoms
Electrocardiogram (ECG) changes indicative of ischaemia (ST elevation or depression)
Development of Pathological Q waves in ECG
Echocardiographic evidence of new regional wall motion abnormality.
Diabetes was defined as having a history of diabetes diagnosed and/or treated with medication and/or diet or fasting blood glucose 126 mg/dl or greater. Hypertension was defined as having a history of hypertension diagnosed and/or treated with medication, diet, and/or exercise, blood pressure greater than 140 mmHg systolic or 90 mmHg diastolic on at least two occasions. Hyperlipidaemia was defined as history of Dyslipidaemia diagnosed and/or treated by a physician or total cholesterol greater than 200 mg/dl, low-density lipoprotein greater than or equal to 130 mg/dl, or high-density lipoprotein <40 mg/dl. High homocystine (HC) was defined HC more than 15 mg/dl and high Lipoprotein a (Lpa) as Lpa more than 30 mg/dl. Current smoker was defined as a person smoking cigarettes within 1 month of index admission. A positive family history for Coronary artery disease (CAD) was defined as evidence of CAD in a parent, sibling, or children before 55 years of age. Overweight was defined as body mass index (BMI) greater than 25 kg/ m2. Obesity was defined as BMI greater than 30 kg/ m2. Waist circumference more than 102 cm was considered as high.
All patients were subjected to coronary angiography during the index admission or on follow up. Significant stenosis was defined as more than 50% stenosis in any of the coronary arteries, insignificant disease as less than 50% stenosis or plaques in any of the coronary arteries.
RESULTS
Out of total 124 patients studied, 118 had ST elevation MI. Thirty eight of these received thrombolytic therapy. Youngest patient was 22 years of age. Most of the patients had anterior wall MI. Three patients presented in cardiogenic shock. There were two deaths, one due to cardiogenic shock and the other had sudden cardiac death.
Table 1 shows the clinical profile and risk factors of the patients.
Table 1.
Clinical profile and risk factors
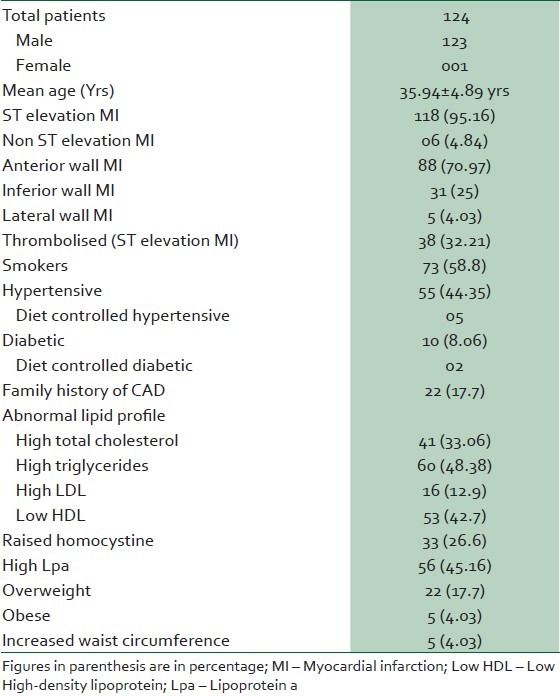
It can be seen that smoking, hypertension, low HDL and raised triglycerides (TG) and Lpa were the major risk factors.
Table 2 shows the coronary angiographic findings in the patients.
Table 2.
Angiographic findings
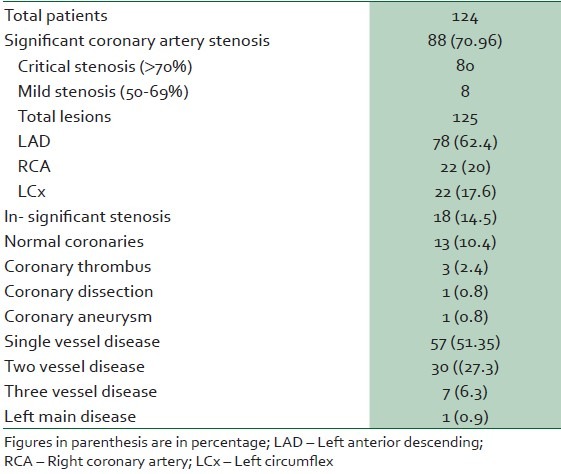
Significant coronary stenosis was found in 88 patients (70.96%). One patient had dissection in proximal left anterior descending (LAD). One patient had aneurysms in left main and right coronary artery probably as a late result of Kawasaki disease. Three patients had coronary thrombosis with no stenosis. We could not find any cause for prothrombotic state in these patients. Thirteen patients had normal coronaries. There was no history of cocaine abuse in these patients.
DISCUSSION
MI is a disease of older population and is uncommon in young, though it occurs at younger age in India compared to Western population. In Global Registry of Acute Coronary Events (GRACE) study, the prevalence of young acute coronary syndrome (ACS) was 6.3%,1 in Thigh ACS Registry, it was 5.8%2 and in Spain Registry, it was 7%.3
MI in young can be divided in to two groups, those with angiographically normal coronary arteries and those with coronary artery disease (CAD). Some young MI patients have normal coronary arteries. The MI in them can be caused by arteritis, thrombosis, embolisation or spasm. As is the case with venous thrombosis, coronary thrombosis can be seen in hypercoagulabe states, such as protein C and protein S deficiency, antiphospholipid syndrome or nephrotic syndrome.4,5,6,7 Coronary artery spasm can cause MI in patients with cocaine abuse8 and also in association with alcohol binges.9 In the second group of young MI (those with CAD), it is mostly a result of atherosclerotic process, which starts in early childhood. Milanig et al., in a necropsy study of 760 young patients, dying of various causes found that 20% of men and 8% of women in the age group between 30-34 yrs had evidence of Coronary heart disease (CHD).10
Etiology of athermanous CHD is limited to conventional risk factors, as in adults, with some differences. Zimmerman et al., found prevalence of smoking in 92% of young CAD patients.11 Mukherjee et al., found prevalence of smoking to be higher in those less than 40 yrs of age, compared to those above 60 yrs (58.7 Vs 43%),12 in patients who underwent Percutaneous transluminal coronary angioplasty (PTCA). We found smoking to be the most common risk factor, present in around 60% of young MI patients. Family history of CAD was found in 18% of our patients. This is much less than in a study done in London by Chen et al., who, found family H/O CAD in 39% of patients.13 Lipid abnormalities, especially raised TG and low HDL were found in around 50% of our patients. Xie et al., also found diabetes mellitus, hypertension and hyperlipidaemia as important risk factors in young women with acute MI.14 They found that each of these risk factors had around 50% prevalence.
Spontaneous coronary dissection is one of the rare causes of MI, especially in young women, in peripartum period. Coronary artery aneurysm may also be a cause of MI in young. These may be congenital or acquired, secondary to Kawasaki's disease in childhood.15
Fibromuscular dysplasia (FMD) is another very rare cause of MI in young, especially in women. It is an idiopathic, nonatherosclerotic and noninflammatory vasculopathy affecting small-to medium-sized arteries. The renal arteries (60-80%) and cervicocranial arteries (20-30%) are most commonly involved. Regardless of the type of FMD, the disease can cause dissection, rupture, or occlusion leading to a wide range of clinical presentations and even death. Fibromuscular dysplasia of the coronary arteries has only rarely been described, since the first report of two probable cases in 1965.16 Pate et al., described seven cases of coronary angiographic characteristics of seven women with acute coronary syndromes and unusual coronary anatomy who also had renal artery FMD.17 In each case, the proximal vessel appeared normal but in the middle or distal segment there was a well-demarcated abrupt transition to diffuse obliterative disease.
Angiographic findings are different in young MI patients compared to older MI patients. Increased prevalence of normal coronary arteries (up to 18%) and minor coronary abnormalities were found in Coronary Artery Surgery Study (CASS). Single vessel disease was found in 38% of subjects. We found SVD in around 57% patients. Xie et al., found SVD in 71.8% in a study of AMI in young Asian women.14
Younger patients with MI have a better prognosis. We had in-hospital mortality of just 1.6%. Xie et al., found no in-hospital mortality in young women with MI.
CONCLUSION
MI in less than 40 yrs of age is almost exclusively seen in male. Smoking, hypertension, high TG, low HDL and raised Lpa are major risk factors. Around 10% patients have normal coronary arteries. Anterior wall MI is more common and most of the patients have single vessel disease. In hospital, mortality is low.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Avezum A, Makdisse M, Spencer F, Gore JM, Fox KA, Montalescot G, et al. Impact of age on management and outcome of acute coronary syndrome: Observations from the Global Registry of Acute Coronary Events (GRACE) Am Heart J. 2005;149:67–73. doi: 10.1016/j.ahj.2004.06.003. [DOI] [PubMed] [Google Scholar]
- 2.Tungsubutra W, Tresukosol D, Buddhari W, Boonsom W, Sanguanwang S, Srichaiveth B, et al. Acute coronary syndrome in young adults: The Thai ACS Registry. J Med Assoc Thai. 2007;90:81–90. [PubMed] [Google Scholar]
- 3.Morillas P, Bertomeu V, Pabón P, Ancillo P, Bermejo J, Fernández C, et al. Characteristics and outcome of acute myocardial infarction in young patients. The PRIAMHO II study. Cardiology. 2007;107:217–25. doi: 10.1159/000095421. [DOI] [PubMed] [Google Scholar]
- 4.Padler FA, Comad AR. Myocardial infarction with normal coronary artery: A case report and review of literature. Am J Med Sci. 1997;314:342–5. doi: 10.1097/00000441-199711000-00013. [DOI] [PubMed] [Google Scholar]
- 5.Penny WJ, Colvin BT, Brooks N. Myocardial infarction with normal coronary arteries and factor XII deficiency. Br Heart J. 1985;53:230–4. doi: 10.1136/hrt.53.2.230. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hamsten A, Norberg R, Björkholm M, de Faire U, Holm G. Antibodies to cardiolipin in young survivors of myocardial infarction: An association with recurrent cardiovascular events. Lancet. 1986;1:113–6. doi: 10.1016/s0140-6736(86)92258-0. [DOI] [PubMed] [Google Scholar]
- 7.Fujimura O, Gulamhusein S. Acute myocardial infarction: Thrombotic complications of nephrotic syndrome. Can J Cardiol. 1987;3:267–9. [PubMed] [Google Scholar]
- 8.Ross GS, Bell J. Myocardial infarction associated with inappropriate use of cocaine for treating epistaxis. Am J Emerg Med. 1992;10:219–22. doi: 10.1016/0735-6757(92)90213-H. [DOI] [PubMed] [Google Scholar]
- 9.Moreyra AE, Kostis JB, Passannante AJ, Kuo PT. Acute myocardial infarction in patients with normal coronary arteries after acute ethanol intoxication. Clin Cardiol. 1982;5:425–30. doi: 10.1002/clc.4960050707. [DOI] [PubMed] [Google Scholar]
- 10.Milonig G, Malcolm GT, Wick G. Early inflammatory and immunological lesions in juvenile atherosclerosis from the pathological determinants of atherosclerosis in youth (PDAY) study. Atherosclerosis. 2002;160:444–8. doi: 10.1016/s0021-9150(01)00596-2. [DOI] [PubMed] [Google Scholar]
- 11.Zimmerman FH, Cameron A, Fisher LD, Ng G. Myocardial infarction in young adults: Angiographic characteristics, risk factors and prognosis, coronary artery surgery study register (CASS) J Am Coll Cardiol. 1995;26:654–61. doi: 10.1016/0735-1097(95)00254-2. [DOI] [PubMed] [Google Scholar]
- 12.Mukherjee D, Hsu A, Moliterno DJ, Lincoff AM, Goormastic M, Topol EJ. Risk factors for premature coronary artery disease and determinants of adverse outcomes after revascularization in patients less than 40 years old. Am J Cardiol. 2003;92:1465–7. doi: 10.1016/j.amjcard.2003.08.062. [DOI] [PubMed] [Google Scholar]
- 13.Chen L, Chester M, Kaski JC. Clinical factors and angiographic features associated with premature coronary artery disease. Chest. 1995;108:364–9. doi: 10.1378/chest.108.2.364. [DOI] [PubMed] [Google Scholar]
- 14.Xie CB, Chan MY, Teo SG, Low AF, Tan HC, Lee CH. Acute myocardial infarction in young Asian women: A comparative study on Chinese, Malay and Indian ethnic groups. Singapore Med J. 2011;52:835–9. [PubMed] [Google Scholar]
- 15.Lee BW, Tay JS, Yip WC, Yap HK, Chan KY, Low PS. Kawasaki syndrome in Chinese children. Ann Trop Pediatric. 1989;9:147–51. doi: 10.1080/02724936.1989.11748618. [DOI] [PubMed] [Google Scholar]
- 16.Hill LD, Antonius JI. Arterial dysplasia: An important surgical lesion. Arch Surg. 1965;90:585–95. doi: 10.1001/archsurg.1965.01320100129020. [DOI] [PubMed] [Google Scholar]
- 17.Pate GE, Lowe R, Buller CE. Fibromuscular dysplasia of the coronary and renal arteries? Catheter Cardiovasc Interv. 2005;64:138–45. doi: 10.1002/ccd.20246. [DOI] [PubMed] [Google Scholar]