

Abstract
Aim:
Long standing mitral valve disease is usually associated with severe pulmonary hypertension. Perioperative pulmonary hypertension is a risk factor for right ventricular (RV) failure and a cause for morbidity and mortality in patients undergoing mitral valve replacement. Phosphodiesterase 5 inhibitor-sildenafil citrate is widely used to treat primary pulmonary hypertension. There is a lack of evidence of effects of oral sildenafil on secondary pulmonary hypertension due to mitral valve disease. The study aims to assess the effectiveness of preoperative oral sildenafil on severe pulmonary hypertension and incidence of RV failure in patients undergoing mitral valve replacement surgery.
Materials and Methods:
A total of 40 patients scheduled for mitral valve replacement with severe pulmonary hypertension (RV systolic pressure (RVSP) ≥60 mmHg) on preoperative transthoracic echo were randomly treated with oral sildenafil 25 mg (N = 20) or placebo (N = 20) eight hourly for 24 h before surgery. Hemodynamic variables were measured 20 min after insertion of pulmonary artery catheter (PAC) under anesthesia (T1), 20 min at weaning from cardiopulmonary bypass (CPB) (T2) and after 1,2, and 6 h (T3, T4, T5, respectively) during the postoperative period.
Results:
Systolic and mean pulmonary artery pressure (MPAP) and pulmonary vascular resistance index (PVRI) were significantly lower (P < 0.0001) in sildenafil group at all times. Ventilation time and postoperative recovery room stay were significantly lower (P < 0.001) in sildenafil group.
Conclusion:
Sildenafil produces significant pulmonary vasodilatory effect as compared with placebo in mitral valve replacement patients with severe pulmonary hypertension. It also reduces ventilation time and intensive care unit (ICU) stay time as compared with placebo. It is concluded that sildenafil is effective in reducing pulmonary hypertension when administered preoperatively in patients with severe pulmonary hypertension undergoing mitral valve replacement surgery.
KEY WORDS: Mitral valve disease, oral sildenafil, phosphodiesterase 5, phosphodiesterase 5 inhibitor, pulmonary hypertension, right ventricular failureEctua vigna Sim terurs
Introduction
Mitral valve disease with pulmonary arterial hypertension (PAH) is characterized by a progressive increase in pulmonary vascular resistance leading to right ventricular (RV) failure and mortality.[1] Prognosis of patients with severe PAH is poor, and treatment options are limited.[2,3] The goal of long-term therapy is to reduce pulmonary vasoconstriction, cause regression of vascular remodeling, and prevent thrombosis.[4]
Pulmonary vascular resistance can be lowered by enhancing cyclic adenosine monophosphate (cAMP) using β-agonist or with the phosphodiesterase type III inhibitor, milrinone.[5,6] Vascular resistance can also be lowered with nitroso vasodilators (nitroglycerine (GTN), sodium nitroprusside, and inhaled nitric oxide). Although inhaled nitric oxide is extremely efficacious, its use is complicated by the requirement for an inhaled delivery system and rebound pulmonary hypertension upon its withdrawal.[7]
Oral sildenafil phosphodiesterase type 5 (PDE5) inhibitor increases cyclic guanosine monophosphate (cGMP) levels and has been shown to be effective for primary pulmonary hypertension.[8,9] It has been shown that sildenafil can be used to manage secondary pulmonary hypertension in perioperative period in patients undergoing cardiac surgeries.[10,11]
This prospective double-blind randomized control study was planned to evaluate the efficacy of oral sildenafil preoperatively in patients with severe pulmonary hypertension undergoing mitral valve replacement surgeries.
Materials and Methods
The patients were enrolled for the study after approval from Institutional Ethics Committee after obtaining written consent. A total of 40 patients who were scheduled for mitral valve replacement surgery with severe PAH, RV systolic pressure (RVSP) ≥50mmHg, as measured by preoperative transthoracic echocardiography, were included in the study. The patients were randomly allocated to either sildenafil (in routine hospital supply) or placebo (multivitamin tablets similar in appearance to sildenafil were used in placebo group, as no other effective oral alternative is available to treat PAH) using a computerized randomization table.
Patients with associated cardiac disease (coronary artery occlusive disease, aortic valve disease, tricuspid regurgitation requiring tricuspid repair, and left ventricular systolic dysfunction ejection fraction <50%), previous cardiac operation, lung disease, liver disease, and renal disease were excluded.
Patients in group S (sildenafil, in routine hospital supply) and group C (control group) were administered oral sildenafil 25 mg (Penegra, Zydus Healthcare, India) three times a day in 24 h preoperative period and placebo in the same fashion, respectively. Nursing staff who were administering the drugs to the patients were blinded during the study. All the patients were administered tablet alprazolam 0.25 mg and tablet pantoprazole 40 mg the night before surgery.
On the day of surgery after arrival to preparation room, patients received 4-5 l of oxygen with mask. Vital parameters were monitored with ECG (electrocardiogram), NIBP (non-invasive blood pressure), and pulse oximeter. After infiltration of local anesthesia (2% lidocaine), a peripheral venous cannula (16 or 18 G) and 20 G arterial cannula in the radial artery of nondominant hand were inserted. Injection clonidine 1 μg/kg and injection midazolam 0.03 mg/kg intravenously were administered 20 min before surgery as a premedication in all patients. Anesthesia was induced with injection midazolam (0.1 mg/kg), fentanyl (7-10 μg/kg), and injection vecuronium (0.08-0.12 mg/kg) and maintained with intermittent bolus doses of fentanyl (2 μg/kg) and vecuronium (0.04 mg/kg) with sevoflurane (1-2%). After induction of anesthesia, the lungs were ventilated with tidal volume of 8 ml/kg at a rate of 12 breaths/min in 50% oxygen-air mixture. Positive end-expiratory pressure was not applied. After that, ventilatory parameters were adjusted to maintain PaO2 between 150-250 mmHg, PaCO2 between 33-38 mmHg, and pH 7.35-7.45.
After induction of anesthesia and under all aseptic and antiseptic precautions, pulmonary artery catheter (PAC) (Edwards Lifescience, Irvine, CA, USA) was inserted in the right internal jugular vein to monitor pulmonary artery pressure, pulmonary capillary wedge pressure (PCWP) and cardiac indices (CIs), SVRI (systemic vascular resistance index), and PVRI (pulmonary vascular resistance index). A temperature probe was inserted into nasopharynx for monitoring of body temperature.
CPB (cardio pulmonary bypass) was performed with Stockert pump (Germany), using membrane oxygenator with standard institutional protocol. During weaning from CPB, GTN and dobutamine (5-10 μg/kg/min) was administered in all patients after achieving body temperature greater than 36°C and normalizing acid-base and electrolyte balance. After 10 min of weaning from CPB, inotropes were titrated according to MAP (mean arterial pressure) and SPAP (systolic pulmonary artery pressure). The number of patients requiring inotropes was recorded.
Data Collection and Analysis
Hemodynamic variables were measured 20 min after insertion of PAC under anesthesia (T1), 20 min after weaning from CPB (T2), 1, 2, and 6 h after transferring the patient to postoperative recovery period (T3, T4, T5). Heart rate (HR), MAP, systolic pulmonary arterial pressure (SPAP), mean pulmonary artery pressure (MPAP), PCWP, cardiac index (CI), systolic vascular resistance index (SVRI), and PVRI were measured at each interval. The statistical analysis was performed using Statistical Package for the Social Sciences (SPSS) version 20.0. The values were expressed as mean ± standard deviation (SD). Chi-square test and unpaired “t” test were used to calculate P values. A value of P < 0.05 was considered statistically significant.
Results
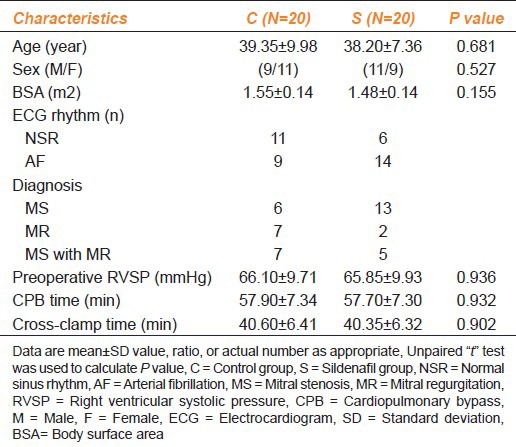
A total of 40 patients were included in the study, 20 patients in each group. Demographic characteristics were similar in both groups. Other parameters like preoperative RVSP, CPB time, and cross-clamp time were similar in both groups (P = 0.936, P = 0.932, P = 0.902, respectively) [Table 1].
Table 1.
Characteristics of patients with mitral valve disease and pulmonary hypertension treated with sildenafil versus placebo
Hemodynamic parameters, i. e. HR, MAP, and PCWP were similar in both groups after induction, after weaning from CPB, and in the postoperative period [Table 2]. SPAP and MPAP were significantly lower (P < 0.0001) during T1-T5 times in sildenafil group as compared with the control group [Table 2].
Table 2.
Hemodynamic parameters during mitral valve replacement surgery in sildenafil versus control groups
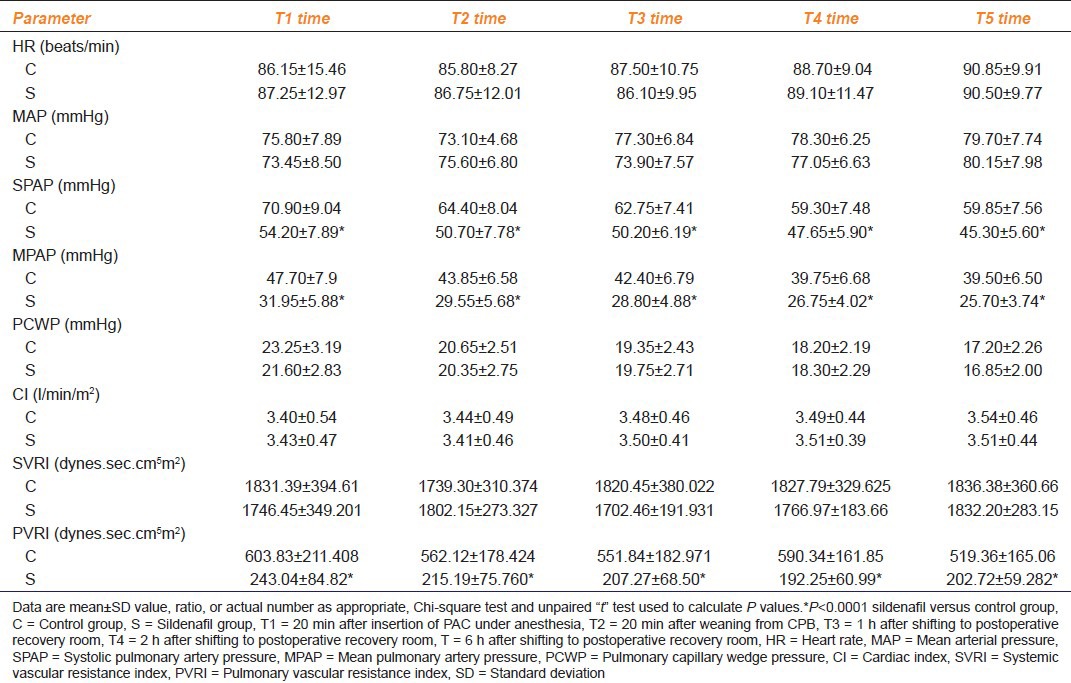
On comparison of CI and SVRI there was no statistical significance between the two groups. PVRI was significantly lower in sildenafil group after induction, after weaning from CPB, and in the postoperative period [Table 2].
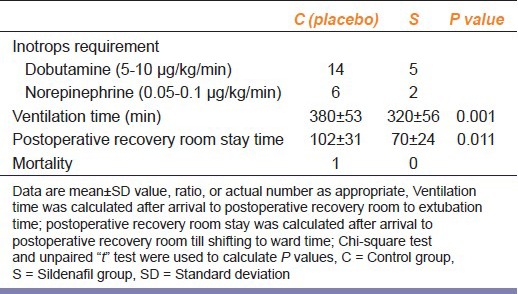
During the period of weaning from CPB, the number of patients who required dobutamine infusion was lower in S group (P < 0.01), whereas the number of patients requiring norepinephrine infusion was not significantly different between the two groups (P < 0.23; Table 3]. Postoperative parameters like ventilation time and postoperative ICU (intensive care unit) stay time was significantly lower in sildenafil group (P = 0.011) as compared with control group [Table 3]. During study, there was one mortality due to low output noted in control group on second postoperative day.
Table 3.
Perioperative parameters during mitral valve replacement surgery in sildenafil and control group of patients (N=20)
Discussion
In this prospective double-blind randomized controlled study, oral sildenafil 25 mg three times over 24 h before surgery produced significant pulmonary vasodilatation without any significant systemic effects. Sildenafil has a favorable effect like lowering pulmonary vascular resistance after induction of anesthesia that extended into postoperative period. SPAP, MPAP, and PVRI were significantly lower in sildenafil group (P < 0.0001) as compared with controlled group during the intraoperative period as well as in postoperative period.
Cardiac surgery in patients with valvular heart disease with severe PAH is often complicated with RV failure with an adverse consequence on its prognosis.[12,13] Right ventricle is susceptible to ischemic injury, as CPB exacerbates PAH,[14] This necessitates perioperative strategy to manage PAH and RV dysfunction. This goal should be achieved without compromising systemic blood pressure and coronary perfusion.[15]
The final messenger for vascular smooth muscle relaxation, cGMP, is metabolized by PDE5.[16] Among the various phosphodiesterase, PDE5 is the predominant type in the normal pulmonary vasculature that may be upregulated after CPB.[17] The inhibition of PDE5 is therefore a logical step to increase the bioavailability of cGMP and support endogenous vasodilation in patient with PAH. PDE5 is selectively inhibited by sildenafil, vardenafil, and tadalafil and less selectively by zaprinast and dipyridamole.[8]
Oral sildenafil is widely used in treatment of patients with erectile dysfunction and shows an excellent cardiovascular safety profile.[18,19] It is emerging as an effective and safe pulmonary vasodilator in primary pulmonary hypertension[20,21] as well as secondary pulmonary hypertension.[22,23] PDE5 is abundant in lung tissue; hence sildenafil selectively inhibits it and preferentially dilates pulmonary vascular beds.[16] Oral sildenafil selectively reduced pulmonary hypertension without any adverse systemic effects.[24]
In the present study, 25 mg of oral sildenafil was administered three times a day for 24 h with the last dose administered 3 h prior to surgery. Wilkens et al.,[21] demonstrated that the maximal hemodynamic effects of sildenafil on pulmonary circulation could be achieved with a dose as low as 25 mg. We used three doses over 24 h to reduce pulmonary hypertension and improve RV function prior to surgery. Sildenafil has a half-life of about 4 h; it is rapidly absorbed via the stomach and its plasma levels peaks within 30-120 min after ingestion.[8,9,10,11,12,13,14,15,16,17,18] Considering these facts, the last dose of sildenafil was administered 3 h prior to surgery.
In this study, SPAP, MPAP, and PVRI were significantly lower (P < 0.0001) after induction of anesthesia, after weaning from CPB, and in immediate postoperative period in sildenafil group as compared with control group. But MAP, PCWP and CI, and SVRI were no significantly differing between two groups. During weaning from CPB, we started GTN infusion and dobutamine infusion in all patients. Inotropes, dobutamine infusion (5-10 μg/kg/min) continued when MAP was lower than 60 mmHg and also norepinephrine infusion (0.05-0.1 μg/kg/min) was added whenever required. In sildenafil group, six (30%) patients required dobutamine infusion, of these two (33.3%) patients required norepinephrine infusion. In the control group, 14 patients required dobutamine infusion and of these five patients required norepinephrine infusion. Sildenafil group had fewer requirements of inotropes than control group. Ventilation time and postoperative recovery room times were significantly lower (P = 0.001) in sildenafil group as compared with control group. Mortality occurred on the second postoperative day due to low output.
In conclusion, preoperative oral sildenafil reduces pulmonary artery pressure in the perioperative period in patients with severe pulmonary hypertension secondary to mitral valve disease undergoing mitral valve replacement. Because of the predominant selective activity of sildenafil in management of pulmonary hypertension and improvement of RV function without compromising the systemic blood pressure, the use of this drug in cardiac surgical patients should be considered. Elaborate studies of oral sildenafil in secondary PAH in larger populations will help validate the results of this study.
Acknowledgments
The authors acknowledge Dr. Sunil Trivedi (Chief Research Officer), Mr. Paresh Dhamecha for statistical analysis, and Ms. Himani Pandya and Ms. Nrupa Kumthekar for assistance.
Footnotes
Source of Support: Nil
Conflict Interest: No
References
- 1.Simonneau G, Galiè N, Rubin LJ, Langleben D, Seeger W, Domenighetti G, et al. Clinical classification of pulmonary hypertension. J Am Coll Cardiol. 2004;43:5–12S. doi: 10.1016/j.jacc.2004.02.037. [DOI] [PubMed] [Google Scholar]
- 2.Hopkins WE, Ochoa LL, Richardson GW, Trulock EP. Comparison of the hemodynamics and survival of adults with severe primary pulmonary hypertension or Eisenmenger syndrome. J Heart Lung Transplant. 1996;15:100–5. [PubMed] [Google Scholar]
- 3.D’Alonzo GE, Barst RJ, Ayres SM, Bergofsky EH, Brundage BH, Detre KM, et al. Survival in patients with primary pulmonary hypertension: Results from a national prospective registry. Ann Intern Med. 1991;115:343–9. doi: 10.7326/0003-4819-115-5-343. [DOI] [PubMed] [Google Scholar]
- 4.Archer S, Rich S. Primary pulmonary hypertension: A vascular biology and translational research “Work in progress”. Circulation. 2000;102:2781–91. doi: 10.1161/01.cir.102.22.2781. [DOI] [PubMed] [Google Scholar]
- 5.Khazin V, Kaufman Y, Zabeeda D, Medalion B, Sasson L, Schachner A, et al. Milrinone and nitric oxide: Combined effect on pulmonary artery pressures after cardiopulmonary bypass in children. J Cardiothorac Vasc Anesth. 2004;18:156–9. doi: 10.1053/j.jvca.2004.01.020. [DOI] [PubMed] [Google Scholar]
- 6.Thelitz S, Oishi P, Sanchez LS, Bekker JM, Ovadia B, Johengen MJ, et al. Phosphodiesterase-3 inhibition prevents the increase in pulmonary vascular resistance following inhaled nitric oxide withdrawal in lambs. Pediatr Crit Care Med. 2004;5:234–9. doi: 10.1097/01.pcc.0000124021.25393.2d. [DOI] [PubMed] [Google Scholar]
- 7.Oishi P, Grobe A, Benavidez E, Ovadia B, Harmon C, Ross GA, et al. Inhaled nitric oxide induced NOS inhibition and rebound pulmonary hypertension: A role for superoxide and peroxynitrite in the intact lamb. Am J Physiol Lung Cell Mol Physiol. 2006;290:L359–66. doi: 10.1152/ajplung.00019.2005. [DOI] [PubMed] [Google Scholar]
- 8.Raja SG, Nayak SH. Sildenafil: Emerging cardiovascular indications. Ann Thorac Surg. 2004;78:1496–506. doi: 10.1016/j.athoracsur.2004.02.125. [DOI] [PubMed] [Google Scholar]
- 9.Prasad S, Wilkinson J, Gatzoulis MA. Sildenafil in primary pulmonary hypertension. N Engl J Med. 2000;343:1342. doi: 10.1056/NEJM200011023431814. [DOI] [PubMed] [Google Scholar]
- 10.Ghofrani HA, Olschewski H, Seeger W, Grimminger F. Sildenafil for treatment of severe pulmonary hypertension and commencing right-heart failure. Pneumologie. 2002;56:665–72. doi: 10.1055/s-2002-35557. [DOI] [PubMed] [Google Scholar]
- 11.Trachte AL, Lobato EB, Urdaneta F, Hess PJ, Klodell CT, Martin TD, et al. Oral sildenafil reduces pulmonary hypertension after cardiac surgery. Ann Thorac Surg. 2005;79:194–7. doi: 10.1016/j.athoracsur.2004.06.086. [DOI] [PubMed] [Google Scholar]
- 12.Ward C, Hancock BW. Extreme pulmonary hypertension caused by mitral valve disease: Natural history and results of surgery. Br Heart J. 1975;37:74–8. doi: 10.1136/hrt.37.1.74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Malouf JF, Enriquez-Sarano M, Pellikka PA, Oh JK, Bailey KR, Chandrasekaran K, et al. Severe pulmonary hypertension in patients with severe aortic valve stenosis: Clinical profile and prognostic implications. J Am Coll Cardiol. 2002;40:789–95. doi: 10.1016/s0735-1097(02)02002-8. [DOI] [PubMed] [Google Scholar]
- 14.Mangano DT. Biventricular function after myocardial revascularization in humans: deterioration and recovery patterns during the first 24 hours. Anesthesiology. 1985;62:571–7. doi: 10.1097/00000542-198505000-00005. [DOI] [PubMed] [Google Scholar]
- 15.Calvin JE., Jr Acute right heart failure: Pathophysiology, recognition, and pharmacological management. J Cardiothorac Vasc Anesth. 1991;5:507–13. doi: 10.1016/1053-0770(91)90130-l. [DOI] [PubMed] [Google Scholar]
- 16.Rabe KF, Tenor H, Dent G, Schudt C, Nakashima M, Magnussen H. Identification of PDE isozymes in human pulmonary artery and effect of selective PDE inhibitors. Am J Physiol. 1994;266:536–43. doi: 10.1152/ajplung.1994.266.5.L536. [DOI] [PubMed] [Google Scholar]
- 17.Giad A, Saleh D. Reduced expression of endothelial nitric oxide synthase in the lungs of patients with pulmonary hypertension. N Engl J Med. 1995;333:214–21. doi: 10.1056/NEJM199507273330403. [DOI] [PubMed] [Google Scholar]
- 18.Boolell M, Allen MJ, Ballard SA, Gepi-Attee S, Muirhead GJ, Naylor AM, et al. Sildenafil: An orally active type 5 cyclic GMP-specific phosphodiesterase inhibitor for the treatment of penile erectile dysfunction. Int J Impot Res. 1996;8:47–52. [PubMed] [Google Scholar]
- 19.Kloner RA, Zusman RM. Cardiovascular effects of sildenafil citrate and recommendations for its use. Am J Cardiol. 1999;84:11N–7. doi: 10.1016/s0002-9149(99)00114-9. [DOI] [PubMed] [Google Scholar]
- 20.Sastry BK, Narasimhan C, Reddy NK, Raju BS. Clinical efficacy of sildenafil in primary pulmonary hypertension: A randomized, placebo-controlled, double-blind, crossover study. J Am Coll Cardiol. 2004;43:1149–53. doi: 10.1016/j.jacc.2003.10.056. [DOI] [PubMed] [Google Scholar]
- 21.Wilkens H, Guth A, König J, Forestier N, Cremers B, Hennen B, et al. Effects of inhaled iloprost plus oral sildenafil in patients with primary pulmonary hypertension. Circulation. 2001;104:1218–22. doi: 10.1161/hc3601.096826. [DOI] [PubMed] [Google Scholar]
- 22.Cubillos-Garzón LA, Casas JP, Morillo CA. Sildenafil in secondary pulmonary hypertension. Int J Cardiol. 2003;89:101–2. doi: 10.1016/s0167-5273(02)00456-4. [DOI] [PubMed] [Google Scholar]
- 23.Ghofrani HA, Wiedemann R, Rose F, Schermuly RT, Olschewski H, Weissmann N, et al. Sildenafil for treatment of lung fibrosis and pulmonary hypertension: A randomized controlled trial. Lancet. 2002;360:895–900. doi: 10.1016/S0140-6736(02)11024-5. [DOI] [PubMed] [Google Scholar]
- 24.Schermuly RT, Kreisselmeier KP, Ghofrani HA, Yilmaz H, Butrous G, Ermert L, et al. Chronic sildenafil treatment inhibits monocrotaline-induced pulmonary hypertension in rats. Am J Respir Crit Care Med. 2004;169:39–45. doi: 10.1164/rccm.200302-282OC. [DOI] [PubMed] [Google Scholar]