

Abstract
Background:
Ludwig's angina is a rapidly spreading cellulitis that may produce upper airway obstruction often leading to death.
Aim:
The present paper reviews the management of Ludwig's angina in the third trimester of pregnancy. The inherent dangers to the mother and her unborn child are highlighted.
Materials and Methods:
The case files of pregnant patients who had emergent incision and drainage for life-threatening facial cellulitis at the maxillofacial unit of the Murtala Mohammed Specialist Hospital in Kano, Nigeria, over a 2 year period were retrieved and demographic and clinical characteristics were retrospectively obtained and analyzed descriptively using the statistical package for social sciences (SPSS version 13.0, for Windows, September 2004, Chicago, Illinois). Comparative statistics were determined using Pearson's Chi-square, Fisher's exact tests and independent t tests as appropriate. A P value of less than 0.05 was considered significant.
Results:
A total of 10 patients were seen within the study period, age ranges from 23 to 40 years, mean 29.5 (5.3) years. Majority of the women were in their third decade [60% (6/10)] while the remaining 40% (4/10) were in their fourth decade of life. Two of the patients presented within the period of less than 1 week of onset of symptoms while those who presented within the periods of 1-2 weeks and periods of over 2 weeks accounted for 50% (5/10) and 30% (3/10) respectively. All the patients presented during the third trimester of their pregnancy and odontogenic infections were responsible for 80% (8/10) of the Ludwig's angina. There were 20% mortality among the patients and this was significant for those with underlying systemic conditions (P = 0.02). The time of presentation was not significant for the survival rate of the gravid patient (P = 0.36) but was significant for survival of the fetus (P = 0.01).
Conclusion:
During a life-threatening infectious situation such as Ludwig's angina, risks of maternal and fetal morbidity include both septicemia and asphyxia. Attending clinicians must consider the risks that the condition and the possible treatments may cause the mother and her unborn child.
Keywords: Ludwig's angina, Management, Pregnancy
Introduction
Ludwig's angina is a rapidly spreading cellulitis that may produce upper airway obstruction often leading to death. The most common cause of Ludwig's angina is an odontogenic infection, from one or more grossly decayed teeth and is usually a result of native Streptococci or mixed aerobic and anaerobic organisms in the oral flora.[1]
There is very little publication about this condition in the pregnant patient. This paper reviews the outcome of management of pregnant women in their third trimester who presented to the maxillofacial unit of our institution with facial cellulitis, with clinical findings consistent with that of Ludwig's angina.
Materials and Methods
This was a retrospective study of pregnant patients who had emergent incision and drainage for life-threatening facial cellulitis at the maxillofacial unit of the Murtala Mohammed Specialist Hospital Kano Nigeria from January 2010 to December 2011. The study protocol was exempted for ethical clearance by our institutional ethics committee. The patients had stab incisions, under local anesthesia, at the submandibular area bilaterally and the submental region. This was followed by exploration with sinus forceps and institution of corrugated rubber drains. The retrospectively obtained information included the age, level of education, number of pregnancy, gestational period and use of herbal medications as well as the onset and duration of symptoms prior to presentation. The collected data were analyzed using the statistical packages for social sciences (SPSS version 13.0 for Windows, September 2004, Chicago, Illinois). Categorical variables were presented as frequencies and percentages while continuous variables as mean and standard deviation. Comparative statistics were determined using Pearson's chi square, Fisher's exact tests and independent t tests as appropriate. A P value of less than 0.05 was considered significant.
Results
A total of 10 patients were seen within the study period, age ranges from 23 to 40 years, mean 29.5 (5.3). Majority of the women were in their third decade [60% (6/10)] while the remaining 40% (4/10) were in their fourth decade of life. All patients were semi-literates with elementary being the highest level of education attained 50% (5/10) and the remaining 50% (5/10) only had Islamic education without any form of western education. Two of the patients presented within the period of less than 1 week of onset of symptoms while those who presented within the periods of 1-2 weeks and periods of over 2 weeks accounted for 50% (5/10) and 30% (3/10) respectively. All the patients presented during the third trimester of their pregnancy and odontogenic infections were responsible for 80% (8/10) of the Ludwig's angina. The cause was unknown in the remaining 20% (2/10) of cases. This was also supported by the fact that a history of pre-existing toothache was obtained in the same proportion of patients [Table 1].
Table 1.
Clinical characteristics of patients
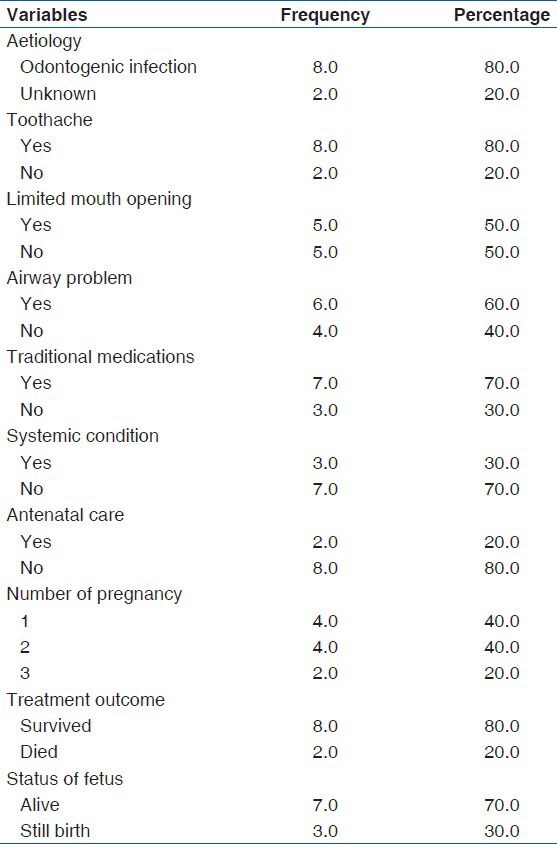
The deliveries were at full term in 80% (8/10) of cases while preterm in the remaining 20% (2/10). Majority of the deliveries [80 % (8/10)] occurred at home with the assistance of traditional birth attendants. None of the patients required induced delivery as part of the treatment plan. In all, 70% (7/10) of the fetus were delivered alive while still birth occurred in the remaining 30% (3/10). Two of the still births were preterm with the delivery occurring in the home environment, around the 28th and 29th weeks of gestation respectively. The other case of still birth occurred at full term and the delivery took place in a hospital environment. Two out of the 10 patients died giving mortality of 20% (2/10). Of the two gravid patients managed in the hospital, the mother and her baby survived in one of the cases while in the second case, both mother and child could not survive, giving 50% (5/10) survival rate. The other death occurred in a woman who presented to the hospital postpartum after she has had a still birth at home.
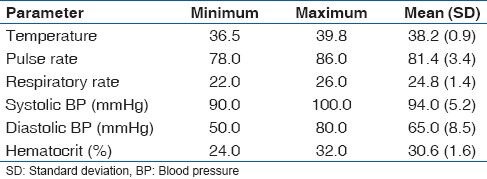
The baseline clinical parameters for the patients at presentation are shown in Table 2. The difference between the mean basal hematocrit of patients who survived, 31.3 (1.03) and those who died, 25.0 (1.14) was statistically significant (P < 0.001). The presence of underlying systemic condition also had a significant effect on the treatment outcome of the pregnant women (χ2 = 5.83, P = 0.02). The 20% (2/10) mortality recorded was seen in those with uncontrolled diabetes mellitus and incidentally two of the three observed still births occurred in these patients. Thus, patients with an underlying systemic condition had a very slim chance of survival (relative risk = 0.33; confidence interval = 0.07-1.52; P = 0.02). While the time of presentation had little, but insignificant effect on the rate of survival on the pregnant women (r = 0.45, P = 0.36), this was very critical for the survival of the fetus (r = 0.84, P = 0.01).
Table 2.
Baseline clinical parameters of patients
Discussion
Ludwig's angina is a rapidly and frequently fatal progressive gangrenous cellulitis and edema of the soft-tissues of the neck and floor of the mouth. Airway compromised has been the leading cause of death. The infection and edema are limited by the deep cervical fascia, mandible and hyoid. As a result, the tongue and floor of the mouth are elevated and posteriorly displaced with compromise of the airway, which can result in abrupt asphyxiation. Infection often results from Streptococci, Staphylococci or Bacteroides, although 50% of infections are polymicrobial. Management of a patient with Ludwig's angina requires early aggressive therapy with antibiotics, incision and drainage of any abscess and protection of the airway.[2,3] In addition, the offending tooth or teeth is usually extracted.
Odontogenic infections were responsible for the majority of Ludwig's angina cases observed in the present study. There is cumulative evidence linking periodontal diseases with preterm delivery and low neonatal birth weight.[4,5] These processes are thought to be initiated through local production of inflammatory cytokines and prostaglandins by cells of the fetal membranes when exposed to bacteria or its by-products.[6] Other documented changes in the gravid patient include mild immunosuppression,[7] lower oxygen reserve with increase fetal hypoxia during periods of hypoventilation. The hormonal changes in pregnancy may manifest orally by changes in the periodontal tissues, which becomes more sensitive and susceptible to irritation by plaques. This is further worsened by the altered eating pattern in the pregnant woman who tends to eat more of snacks and more frequently. This results in aggravation of plaque accumulation, increase in tooth decay and rapid progression of previously existing decay. Often times, because of the mild immunosuppression in pregnancy, the infections may spread to affect the placenta, uterus and possibly the fetus resulting in fetal septicemia.[8] The observed still birth in this study may probably be as a result of fetal septicemia.
The preterm deliveries recorded in the present study may largely be due to the overwhelming infections, which were predominantly of odontogenic origin. This was further complicated by the presence of underlying systemic diseases, The other possible contributory factors in our study population may include low socioeconomic status (as suggested by their educational level), stress, anemia, age at parity and unbooked deliveries, which accounted for 80% in this study. It is also possible that the unhygienic nature of the home environment coupled with the intake of local herbal medications would have contributed to the 2 observed still births out of the 8 deliveries that occurred in the home environment.
In the management of Ludwig's angina in the pregnant woman, both the physiologic changes of pregnancy and the perinatal effects of the treatment must be considered. Our management protocol include incision and drainage, empirical antibiotics usually penicillins and metronidazole. Opioids analgesics and other agents with sedative effects are avoided because of the potential risk to the fetus. All the incisions and drainage were performed under local anesthesia and none of the patients required tracheostomy or any form of artificial airway. This sharply contrast published reports,[1,9,10] from the western world where severe fascial space cellulitis such as Ludwig's angina are managed under endotracheal intubation with the attendant morbidity associated with the use of general anesthesia.
We observed two deaths among the pregnant patients. The deaths were probably due to overwhelming septicemia, occurring in a background of uncontrolled diabetes mellitus. Septicemia has been one of the leading causes of death in Ludwig's angina after airway obstruction. That 50% mortality was observed in the only two cases managed under orthodox medical care further strengthens the importance of septicemia, which may have been aggravated by a delay in presentation to the hospital, in the observed deaths. Another possible cause of death may be as a result of anemia since a significant difference was found between the mean basal hematocrit value in patients who survived and those who did not. Early presentation may have helped reduce the morbidity and mortality, especially in the unborn child.
Ludwig's angina is a life-threatening but preventable condition. Campaign for antenatal care and hospital delivery should be intensified and the pregnant woman should be educated on the importance of regular dental visits. Oral health education should be a component of routine antenatal lectures. Most dental procedures can safely be carried out during the second trimester of pregnancy and procedures such as dental fillings and scaling and polishing and even simple dental extractions can be carried out at this stage. During a life-threatening infectious situation such as Ludwig's angina, risks of maternal and fetal morbidity include both septicemia and asphyxia. Attending clinicians must consider the risks that the condition and the possible treatments may cause the mother and her unborn child.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Parhiscar A, Har-El G. Deep neck abscess: A retrospective review of 210 cases. Ann Otol Rhinol Laryngol. 2001;110:1051–4. doi: 10.1177/000348940111001111. [DOI] [PubMed] [Google Scholar]
- 2.Marple BF. Ludwig angina: A review of current airway management. Arch Otolaryngol Head Neck Surg. 1999;125:596–9. doi: 10.1001/archotol.125.5.596. [DOI] [PubMed] [Google Scholar]
- 3.Bansal A, Miskoff J, Lis RJ. Otolaryngologic critical care. Crit Care Clin. 2003;19:55–72. doi: 10.1016/s0749-0704(02)00062-3. [DOI] [PubMed] [Google Scholar]
- 4.López NJ, Smith PC, Gutierrez J. Periodontal therapy may reduce the risk of preterm low birth weight in women with periodontal disease: A randomized controlled trial. J Periodontol. 2002;73:911–24. doi: 10.1902/jop.2002.73.8.911. [DOI] [PubMed] [Google Scholar]
- 5.Jarjoura K, Devine PC, Perez-Delboy A, Herrera-Abreu M, D’Alton M, Papapanou PN. Markers of periodontal infection and preterm birth. Am J Obstet Gynecol. 2005;192:513–9. doi: 10.1016/j.ajog.2004.07.018. [DOI] [PubMed] [Google Scholar]
- 6.Romero R, Mazor M. Infection and preterm labor. Clin Obstet Gynecol. 1988;31:553–84. doi: 10.1097/00003081-198809000-00006. [DOI] [PubMed] [Google Scholar]
- 7.Lawrenz DR, Whitley BD, Helfrick JF. Considerations in the management of maxillofacial infections in the pregnant patient. J Oral Maxillofac Surg. 1996;54:474–85. doi: 10.1016/s0278-2391(96)90125-1. [DOI] [PubMed] [Google Scholar]
- 8.Abramowicz S, Abramowicz JS, Dolwick MF. Severe life threatening maxillofacial infection in pregnancy presented as Ludwig's angina. Infect Dis Obstet Gynecol 2006. 2006 doi: 10.1155/IDOG/2006/51931. 51931. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kurien M, Mathew J, Job A, Zachariah N. Ludwig's angina. Clin Otolaryngol Allied Sci. 1997;22:263–5. doi: 10.1046/j.1365-2273.1997.00014.x. [DOI] [PubMed] [Google Scholar]
- 10.Har-El G, Aroesty JH, Shaha A, Lucente FE. Changing trends in deep neck abscess. A retrospective study of 110 patients. Oral Surg Oral Med Oral Pathol. 1994;77:446–50. doi: 10.1016/0030-4220(94)90221-6. [DOI] [PubMed] [Google Scholar]