

Abstract
Fibrolamellar hepatocellular carcinoma (FLHCC) is a rare malignant liver neoplasm, commonly observed in adolescents and young adults of both genders. The disease is more common in Caucasians and in patients without a prior history of liver disease. The best treatment option is a surgical resection associated with liver hilum lymph node dissection. However, there is no established systemic drug treatment for patients with locally advanced or metastatic disease. We report on a patient with advanced FLHCC, initially considered unresectable due to invasion of the right and the middle hepatic veins and circumferential involvement of the left hepatic vein. Following the treatment with gemcitabine-oxaliplatin systemic chemotherapy, the patient exhibited a significant tumor reduction. As a result, a complete resection was performed with an extended right hepatectomy associated with a partial resection of the inferior vena cava, a wedge resection in segment 2, and lymphadenectomy of the hepatic hilum. The case was unusual due to the significant tumor downstaging with gemcitabine-oxaliplatin, potentially enabling curative resection. More studies are needed to confirm the efficacy of the systemic drug treatment for FLHCC.
Keywords: Chemotherapy, Gemcitabine, Oxaliplatin, Hepatectomy, Hepatic veins, Fibrolamellar hepatocellular carcinoma
Core tip: Fibrolamellar hepatocellular carcinoma (FLHCC) is a rare malignant liver neoplasm. The best treatment option is a surgical resection with liver hilum lymph node dissection. Currently there is no established systemic drug treatment for patients with locally advanced or metastatic disease. In this report, a patient with advanced FLHCC, initially considered unresectable due to vascular invasion, exhibited a significant tumor reduction following systemic chemotherapy with gemcitabine-oxaliplatin, allowing resection. This was an unusual case where gemcitabine-oxaliplatin treatment led to a significant tumor downstaging enabling curative resection. Additional studies are needed to confirm the efficacy of the systemic drug treatment for FLHCC.
INTRODUCTION
Fibrolamellar hepatocellular carcinoma (FLHCC) is an uncommon primary liver neoplasm, representing 0.6%-8.6% of all hepatocellular carcinomas (HCC)[1]. It was first described in 1956 by Edmonson as a rare distinctive form of HCC[2]. In general, it is a vascular tumor with prominent fibrosis. Microscopically, FLHCC appears as a well-differentiated tumor comprised of large polygonal cells with large nuclei and nucleoli, as well as an abundant eosinophilic cytoplasm, arranged in lamellar bands of collagen fibers[3]. FLHCC most often affects adolescents and young adults of both genders, often Caucasian, and without a prior history of liver disease[1,4]. Liver function tests are typically normal or only mildly elevated. Commonly used HCC markers, such as alpha-fetoprotein, are of little help in diagnosing and monitoring disease progression in the majority of patients, as only a small proportion of patients (7%-11%) show elevation in alpha-fetoprotein levels[5,6].
FLHCC is believed to more commonly metastasize to regional lymph nodes. The cornerstone for FLHCC treatment is a surgical resection associated with lymph node dissection[3,4]. Patients with advanced FLHCC represent a population in need of novel and effective treatments. Due to the lack of data on effective systemic drug treatments as well as the FLHCC patients’ paucity, it is difficult to conduct clinical trials[1]. The authors report an unusual case of a young patient, initially with an unresectable FLHCC, treated with gemcitabine-oxaliplatin (GEMOX), resulting in an excellent response and complete resection of the tumor.
CASE REPORT
A previously healthy 35-year-old Caucasian female complaining of abdominal pain, 3 kg weight loss, weakness, back pain, and a palpable mass in the right upper quadrant, was referred for evaluation. Physical examination disclosed a palpable hard mass 20 cm below the right costal margin. There were no signs of liver disease or other relevant findings. A computed tomography scan (Figure 1) showed a suggestive FLHCC mass (17 cm × 15 cm) affecting the right liver lobe. In addition, the mass affected segment 4b by obstructing the right portal branch, invading both the right and middle hepatic veins, circumferentially wrapping the left hepatic vein, and compressing the inferior vena cava. A lesion (ø 6.5 cm) in segment 2 displayed the same characteristics, as well as lymphadenopathy at the liver hilum up to 2.7 cm in size. Laboratory tests revealed elevated levels of alkaline phosphatase, gamma-glutamyl transpeptidase, and alpha-fetoprotein (44.395 ng/mL). Both hepatitis B and C serologies were negative. Colonoscopy and endoscopy results were normal. Percutaneous biopsy of the tumor confirmed FLHCC. The lesion was considered unresectable because of the extensive vascular involvement, especially of the hepatic veins; therefore, the patient was referred to an oncologist for a systemic drug treatment. Transplantation was eliminated due to the presence of the hilar lymph nodes (extra hepatic disease).
Figure 1.
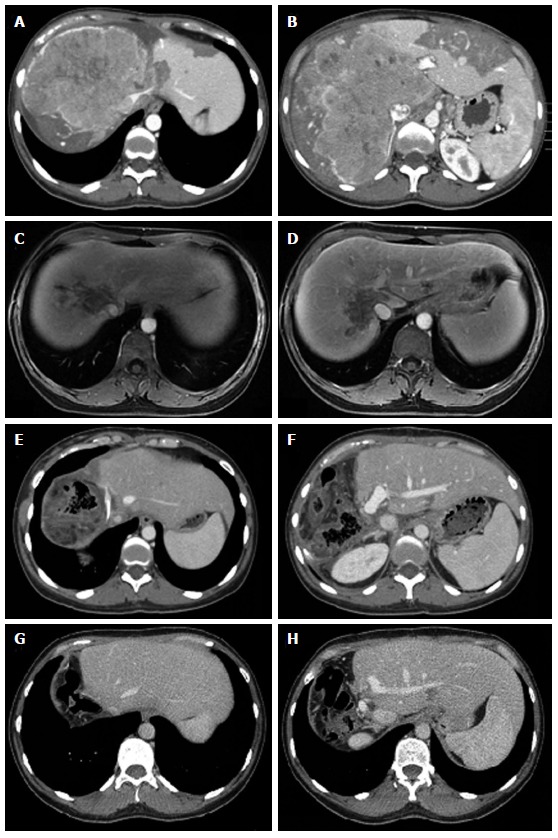
Abdominal computed tomography and magnetic resonance imaging of a 35-year-old Caucasian female, with no previous history of liver disease, showing a large mass in the upper right quadrant. A, B: Abdominal computed tomography (CT) before chemotherapy showing a large mass invading (17 cm × 15 cm) the right and the middle hepatic veins, and surrounding the left hepatic vein; C, D: Abdominal magnetic resonance imaging after gemcitabine-oxaliplatin chemotherapy showing significant reduction of the tumor size; E, F: Abdominal CT two weeks after surgery with hypertrophy of the left lateral segment of liver (liver remnant), and free and patent left branch of the portal vein and left hepatic vein; G, H: Late follow-up after 14 mo.
The patient received 100 mg of oxaliplatin and 1400 mg of gemcitabine (20 mg/kg) every two weeks during an 11-mo treatment period, with good tolerance. The staging intervals, scheduled every four months, included either a computed tomography scan or magnetic resonance imaging. After one year of treatment, magnetic resonance imaging showed significant tumor size reduction (the larger lesion size was 8.5 cm and the smaller 2.2 cm), decrease in contact with the left hepatic vein and inferior vena cava, disappearance of the lymphadenopathy, and hypertrophy of the left lateral segment of the liver (38% of total liver volume) (Figure 1). In addition, there was a significant decrease in alpha-fetoprotein levels to 45 ng/mL.
The patient was submitted to an extended right hepatectomy with partial resection of the inferior vena cava associated with a wedge resection in segment 2 and lymphadenectomy of the hepatic hilum. The procedure lasted 450 min with the patient receiving two units of packed red blood cells and staying in the intensive care unit for two days. The patient developed a postoperative biliary fistula, which was treated conservatively, with spontaneous closure after 28 d. Our patient was discharged on the 17th postoperative day in a good clinical condition.
Histology examination confirmed FLHCC with microscopically free margins (R0 resection). The hepatic hilum lymph nodes were free of the disease. At discharge, the level of alpha-fetoprotein was within normal limits (4.7 ng/mL). The patient had no signs of the disease recurrence at the 14-mo follow-up.
DISCUSSION
The best treatment option for FLHCC is a resection with adequate lymph node dissection[3,5]. However, a resection is not always possible due to locally advanced disease. The best therapy for these patients has not been well established[1]. Several chemotherapy agents have been used for FLHCC treatment, including fluoropyrimidines, doxorubicin, cisplatin, oxaliplatin, gemcitabine, and irinotecan, as well as interferon, bevacizumab, and sorafenib in either combination regimens or separately[1,5]. Locoregional therapies, such as transarterial chemoembolization, radiofrequency ablation, external beam radiation, percutaneous ethanol injection, and hepatic arterial infusion of cisplatin, had disappointing results[1,5]. A study from the Fibrolamellar Carcinoma Consortium, which contained 99 patients diagnosed with FLHCC, showed that from the 73 patients who underwent surgery, 13% (10/73) received preoperative chemotherapy, external beam radiation, and/or transarterial chemoembolization. Twenty one percent (20/99) were considered to have unresectable disease and 13 of them were treated with various combinations of systemic drug therapy with or without locoregional therapies. Chemotherapy agents used in the study included fluoropyrimidines, doxorubicin, cisplatin, oxaliplatin, gemcitabine, and irinotecan. However, a multivariate analysis showed a lack of surgery to be an independently poor overall survival predictor[1]. Kaseb et al[7] studied 94 FLHCC patients and found tumor resection to be a factor positively associated with longer overall survival; 5-fluorouracil-interferon combination was the most frequently used systemic therapy.
HCC markers, such as alpha-fetoprotein, are of little help in diagnosing and monitoring disease progression in the majority of patients. This is mostly due to a small proportion of patients (7%-11%) showing elevated alpha-fetoprotein levels[5,6]. Our patient probably belongs to this peculiar group since her initial levels of alpha-fetoprotein were high, and were lowered to normal levels following surgery.
Sorafenib is currently the standard treatment for advanced HCC[8,9]. However, no systemic drug therapy had convincingly improved survival among patients with advanced HCC. There have been attempts to evaluate the efficacy of new drugs or combination treatments in clinical trials. Some of the examples of these trials include: (1) doxorubicin alone and/or with gemcitabine; (2) combination of cisplatin, doxorubicin, 5-fluorouracil, and alpha-interferon; and (3) combination of irinotecan, taxanes, gemcitabine, topotecan, and thymidilate synthase inhibitors[10]. The GEMOX regimen appeared to be the most promising, based on a lack of renal and hepatic toxicity in cirrhotic patients, promising efficacy in the phase II trials for advanced HCC, and with possible extended benefit for Child B cirrhosis[10-13]. Louafi et al[12], studying 32 patients treated for advanced HCC, had two patients that underwent HCC curative resection after partial response to GEMOX. In a retrospective multicenter study, Zaanan et al[10] observed tumor responses in 204 patients with advanced HCC treated with GEMOX. In 10 patients, tumor response either permitted secondary surgical resection of residual tumors or orthotopic liver transplantation. Radiofrequency ablation was performed in one patient, transcatheter arterial chemoembolization in three patients, cyberknife treatment in one patient, and radioembolization in two patients. There was also a case report on a patient with metastatic HCC without liver disease with a complete response after 12 cycles of GEMOX[14].
There has been only one reported case of FLHCC with a complete response after GEMOX treatment. In this case, a young woman had a histologically proven metastatic lymph node relapse after resection of the primary tumor. GEMOX regimen lead to a complete response without relapse five years after chemotherapy discontinuation[15].
HCC patients have poor tolerance to systemic chemotherapy, mostly due to cirrhotic liver[15]. In most cases FLHCC patients do not have a prior history of liver disease[4]. This may explain the better tolerance to chemotherapy, hence leading to a better response, as is the case in our patient. In the present case, the chemotherapy regimen with GEMOX promoted FLHCC downstaging, potentially allowing for a curative treatment. However, more studies are needed to confirm GEMOX efficacy.
COMMENTS
Case characteristics
A previously healthy 35-year-old Caucasian female complained of abdominal pain, 3 kg weight loss, weakness, back pain, and a palpable mass in the right upper quadrant.
Clinical diagnosis
A palpable hard mass was found to be located 20 cm below the right costal margin with no signs of liver disease.
Differential diagnosis
Hepatocellular carcinoma, cholangiocarcinoma, liver metastasis.
Laboratory diagnosis
The patient had elevated levels of alkaline phosphatase, gamma-glutamyl transpeptidase, and alpha-fetoprotein, and negative serologies for both hepatitis B and C.
Imaging diagnosis
A computed tomography scan showed a suggestive fibrolamellar hepatocellular carcinoma (FLHCC) mass (17 cm × 15 cm) affecting the right liver lobe and segment 4b, obstructing the right portal branch, invading the right and middle hepatic veins, circumferentially wrapping the left hepatic vein, and compressing the inferior vena cava; the second lesion (6.5 cm) in segment 2 had the same characteristics and lymphadenopathy at the liver hilum (up to 2.7 cm), with colonoscopy and endoscopy results being normal.
Pathological diagnosis
FLHCC was confirmed by percutaneous biopsy of the tumor.
Treatment
The patient received 1400 mg of gemcitabine (20 mg/kg) and 100 mg of oxaliplatin (GEMOX) every 2 wk over 11 mo, with a significant tumor reduction, allowing for resection.
Related reports
The best treatment option for FLHCC is resection with adequate lymph node dissection. However, resection is not always possible due to local disease advancement. There has not been well-established disease therapy for these patients.
Term explanation
FLHCC is an uncommon primary liver neoplasm. In general, it is a vascular tumor with prominent fibrosis. Microscopically, FLHCC appears as a well-differentiated tumor comprised of large polygonal cells with large nuclei and nucleoli, as well as an abundant eosinophilic cytoplasm, arranged in lamellar bands of collagen fibers.
Experiences and lessons
In the present case, the chemotherapy regimen with GEMOX promoted FLHCC downstaging, potentially allowing for curative treatment and suggesting GEMOX as a possible chemotherapy treatment for patients with advanced FLHCC; however, more studies are needed to confirm GEMOX efficacy.
Peer review
This is an interesting case of a young female with an initially considered unresectable FLHCC. Significant tumor downstaging with GEMOX allowed surgical resection.
Footnotes
P- Reviewers: Boeck S, Ghinolfi D S- Editor: Song XX L- Editor: A E- Editor: Wu HL
References
- 1.Ang CS, Kelley RK, Choti MA, Cosgrove DP, Chou JF, Klimstra D, Torbenson MS, Ferrell L, Pawlik TM, Fong Y, et al. Clinicopathologic characteristics and survival outcomes of patients with fibrolamellar carcinoma: data from the fibrolamellar carcinoma consortium. Gastrointest Cancer Res. 2013;6:3–9. [PMC free article] [PubMed] [Google Scholar]
- 2.Edmondson HA. Differential diagnosis of tumors and tumor-like lesions of liver in infancy and childhood. AMA J Dis Child. 1956;91:168–186. doi: 10.1001/archpedi.1956.02060020170015. [DOI] [PubMed] [Google Scholar]
- 3.Mavros MN, Mayo SC, Hyder O, Pawlik TM. A systematic review: treatment and prognosis of patients with fibrolamellar hepatocellular carcinoma. J Am Coll Surg. 2012;215:820–830. doi: 10.1016/j.jamcollsurg.2012.08.001. [DOI] [PubMed] [Google Scholar]
- 4.Mayo SC, Mavros MN, Nathan H, Cosgrove D, Herman JM, Kamel I, Anders RA, Pawlik TM. Treatment and prognosis of patients with fibrolamellar hepatocellular carcinoma: a national perspective. J Am Coll Surg. 2014;218:196–205. doi: 10.1016/j.jamcollsurg.2013.10.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Liu S, Chan KW, Wang B, Qiao L. Fibrolamellar hepatocellular carcinoma. Am J Gastroenterol. 2009;104:2617–2624; quiz 2625. doi: 10.1038/ajg.2009.440. [DOI] [PubMed] [Google Scholar]
- 6.Stipa F, Yoon SS, Liau KH, Fong Y, Jarnagin WR, D’Angelica M, Abou-Alfa G, Blumgart LH, DeMatteo RP. Outcome of patients with fibrolamellar hepatocellular carcinoma. Cancer. 2006;106:1331–1338. doi: 10.1002/cncr.21703. [DOI] [PubMed] [Google Scholar]
- 7.Kaseb AO, Shama M, Sahin IH, Nooka A, Hassabo HM, Vauthey JN, Aloia T, Abbruzzese JL, Subbiah IM, Janku F, et al. Prognostic indicators and treatment outcome in 94 cases of fibrolamellar hepatocellular carcinoma. Oncology. 2013;85:197–203. doi: 10.1159/000354698. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Cheng AL, Kang YK, Chen Z, Tsao CJ, Qin S, Kim JS, Luo R, Feng J, Ye S, Yang TS, et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: a phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009;10:25–34. doi: 10.1016/S1470-2045(08)70285-7. [DOI] [PubMed] [Google Scholar]
- 9.Trevisani F, Frigerio M, Santi V, Grignaschi A, Bernardi M. Hepatocellular carcinoma in non-cirrhotic liver: a reappraisal. Dig Liver Dis. 2010;42:341–347. doi: 10.1016/j.dld.2009.09.002. [DOI] [PubMed] [Google Scholar]
- 10.Zaanan A, Williet N, Hebbar M, Dabakuyo TS, Fartoux L, Mansourbakht T, Dubreuil O, Rosmorduc O, Cattan S, Bonnetain F, et al. Gemcitabine plus oxaliplatin in advanced hepatocellular carcinoma: a large multicenter AGEO study. J Hepatol. 2013;58:81–88. doi: 10.1016/j.jhep.2012.09.006. [DOI] [PubMed] [Google Scholar]
- 11.Taïeb J, Bonyhay L, Golli L, Ducreux M, Boleslawski E, Tigaud JM, de Baere T, Mansourbakht T, Delgado MA, Hannoun L, et al. Gemcitabine plus oxaliplatin for patients with advanced hepatocellular carcinoma using two different schedules. Cancer. 2003;98:2664–2670. doi: 10.1002/cncr.11869. [DOI] [PubMed] [Google Scholar]
- 12.Louafi S, Boige V, Ducreux M, Bonyhay L, Mansourbakht T, de Baere T, Asnacios A, Hannoun L, Poynard T, Taïeb J. Gemcitabine plus oxaliplatin (GEMOX) in patients with advanced hepatocellular carcinoma (HCC): results of a phase II study. Cancer. 2007;109:1384–1390. doi: 10.1002/cncr.22532. [DOI] [PubMed] [Google Scholar]
- 13.Dhooge M, Coriat R, Mir O, Perkins G, Brezault C, Boudou-Rouquette P, Goldwasser F, Chaussade S. Feasibility of gemcitabine plus oxaliplatin in advanced hepatocellular carcinoma patients with Child-Pugh B cirrhosis. Oncology. 2013;84:32–38. doi: 10.1159/000342763. [DOI] [PubMed] [Google Scholar]
- 14.Boschetti G, Walter T, Hervieu V, Cassier P, Lombard-Bohas C, Adham M, Scoazec JY, Dumortier J. Complete response of hepatocellular carcinoma with systemic combination chemotherapy: not to get out the chemotherapy? Eur J Gastroenterol Hepatol. 2010;22:1015–1018. doi: 10.1097/MEG.0b013e328336565a. [DOI] [PubMed] [Google Scholar]
- 15.Gras P, Truant S, Boige V, Ladrat L, Rougier P, Pruvot FR, Hebbar M. Prolonged Complete Response after GEMOX Chemotherapy in a Patient with Advanced Fibrolamellar Hepatocellular Carcinoma. Case Rep Oncol. 2012;5:169–172. doi: 10.1159/000338242. [DOI] [PMC free article] [PubMed] [Google Scholar]