

Abstract
Background
To determine the 1,25-dihydroxyvitamin D3 [1,25(OH)2D3] concentrations to patients with tuberculosis (TB) and whether it influenced the patient’s clinical features.
Methods
For the first part, a total of 153 healthy adults and 74 patients with pulmonary TB (PTB) were enrolled. Serum concentrations of 1,25(OH)2D3 were determined by liquid chromatography-tandem mass spectroscopy to examine the 1,25(OH)2D3 concentrations of the two groups from the peripheral blood. If there are differences between the two groups, what follow will increase the experimental group numbers to examine the relationship among the 1,25(OH)2D3 concentrations with the numbers of the lesion area, the tubercule bacilli in sputum and the CD4/CD8 ratio of T lymphocytes in the peripheral blood.
Results
In the first part, the 1,25(OH)2D3 concentrations was lower in patients with TB than in those healthy adults [365.9 (SD 235.7) vs. 464.3 (SD 335.6), P<0.05]. In the second part, we increased the sample size to 134 (male 91 cases, female 43 cases). we found that the plasma levels of 1,25(OH)2D3 are not correlated with the numbers of the lesion area and the tubercule bacilli in sputum, but the 1,25(OH)2D3 levels can interact the ratio of CD4/CD8 T lymphocytes, it shows a positive correlation with the ratio of CD4/CD8 T lymphocytes.
Conclusions
The 1,25(OH)2D3 concentrations in TB patients lower than the healthy adults, it might exist as a risk factor during the development of TB or TB might affect the levels of 1,25(OH)2D3. But the different status vitamin D concentration might not affect the numbers of the lesion area, the tubercule bacilli in sputum. It shows a positive correlation with the ratio of CD4/CD8 T lymphocytes. The study will have a significance value to clinical medicine, but further study will need to study the levels of 1,25(OH)2D3 with the TB.
Keywords: Tuberculosis (TB); 1,25-dihydroxyvitamin D3 [1,25(OH)2D3]; clinical features; CD4/CD8 T lymphocytes
Introduction
Vitamin D has a plethora of functions in the human body, of which the regulation of calcium metabolism is the most well-known. In recent years, the important role for vitamin D in the modulation of the innate immune by its role is as an immunomodulator (1-4). Although the effects of vitamin D on the innate immune response have been established in vitro and ex vivo (5,6), some data are available evaluating plasma 25(OH)D concentrations (7-12), there is a few concern and studying of its active metabolite 1,25-dihydroxyvitamin D3 [1,25(OH)2D3] in vivo. Plasma concentrations of 1,25(OH)2D3, but not 25(OH)D3, is the most active form of vitamin D and is responsible for most of its biological actions, directly up-regulates the production of human cathelicidin antimicrobial peptide (CAMP) from monocytes/macrophages infected with mycobacterium tuberculosis (TB) (13-15). 1,25(OH)2D3 status had a strong influence by seasonal variation (16). In addition, there are litter studies regarding 1,25(OH)2D3 with clinical outcomes, in this study, we have examined the 1,25(OH)2D3 concentration of the two groups from the peripheral blood and the relationship about the 1,25(OH)2D3 status among the lesion areas (the number of lesion area was divided into six areas through the lower edge of the 2,4 ribs during the chest X-rays), the tubercule bacilli in sputum. Previous in vitro and animal studies have suggested that 1,25(OH)2D3 has important immunoregulatory properties, and it has been well documented that T lymphocytes are dominant leukocytes present in TB, and the different immunophenotype of lymphocytes affect the prognosis of TB. Previous in vitro and animal studies have suggested that 1,25(OH)2D3 has important immunoregulatory properties and it has been well documented that T lymphocytes are dominant leukocytes present in TB. CD4(+) helper and CD8(+) cytotoxic T cells, two major subsets of T lymphocytes, CD4 T cells become activated and proliferate rapidly secreting cytokines that send signals and maintain active immune response. On the other hand, the CD8 T-cells destroy virally infected cells and tumor cells. The ratio of CD4/CD8 T lymphocyte cell affects the resistance in mycobacterium TB. Previous in vitro and animal studies have suggested that 1,25(OH)2D3 has important immunoregulatory properties. So, at the last, we investigated the ratio of CD4/CD8 lymphocyte cell in TB patients, to investigate whether the status of 1,25(OH)2D3 affects the ratio of CD4/CD8 T lymphocyte cell.
Patients and methods
Patients and data acquisition
The patients were recruited from the clinics of Nanjing Chest Hospital Tuberculosis Research Centre (TRC), who were clinically and radiologically diagnosed with PTB, which was confirmed by sputum smear examinations, culture for M. tuberculosis (at least two sputum specimens positive or culture for acid-fast bacilli by microscopy sputum smear positive) or clinical features. The test group and control group are come from the Eastern China. All the patients were HIV negative and none of them presented with any other infectious disease or any other organ function impaired. To this end, ethylenediamine tetraacetic acid (EDTA) anticoagulated blood was collected before administration of medicine and centrifuged immediately at 2,000 rpm for 10 min at 4 °C, after which plasma was stored at –80 °C until analysis. Serum concentrations of 1,25(OH)2D3 and the ratio of CD4/CD8 T lymphocyte cell were determined by liquid chromatography-tandem mass spectroscopy, the 24 hours smear were collected to be used for concentration smear and routine culture. The number of lesions and smear-negative TB (≥3 sputum smear investigations is negative) or smear-positive TB (≥3 sputum smear investigations is positive) were obtained from the clinical history of the patients to examine the concentrations of the two groups. The lesion areas, the sputum conversion rate of the PTB were obtained from the clinical history to examine the correlations between the 1,25(OH)2D3 concentrations and these relations. The study was approved by the Institutional Ethics Committee of Nanjing Chest Hospital Tuberculosis Research Centre. Informed consent was obtained from each subject before the start of the study.
Statistical analyses
All analyses were performed using SPSS18.0. Student’s t-test was applied to calculate the 1,25(OH)2D3 concentrations between the male and female, the sputum negative and positive, the ratio of CD4/CD8 T lymphocyte cell ≥ and ≤1.0, one way analysis of variance (ANOVA) was used to compare the 1,25(OH)2D3 concentrations among the numbers of the lesion areas of two groups. P value less than 0.05 was considered statistically significant.
Results
1,25(OH)2D3 concentrations in the two groups
A total of 74 TB and 153 healthy adults blood were obtained, in the cases group, 46 males and 28 females, in the control group, 91 males and 72 females, among the two groups, there is no significant difference of basal clinical conditions between the two groups (Table 1). 1,25(OH)2D3 concentrations were found to be significantly decreased among PTB patients compared to the healthy adults [365.9 (SD 235.7) vs. 464.3 (SD 335.6), P<0.05] (Figure 1). In the male group, the 1,25(OH)2D3 concentrations were found to be decreased among PTB patients compared to the healthy adults (P<0.05), unfortunately, in the female group, there is no significant difference between the two groups (P>0.05) (Table 2).
Table 1. Baseline characteristics of the two groups.
| Cases | Controls | |
|---|---|---|
| Male | 46 | 81 |
| Female | 28 | 72 |
| Body mass index (SD) | 19.1 (3.2) | 19.5 (3.7) |
| Total number | 74 | 153 |
Figure 1.
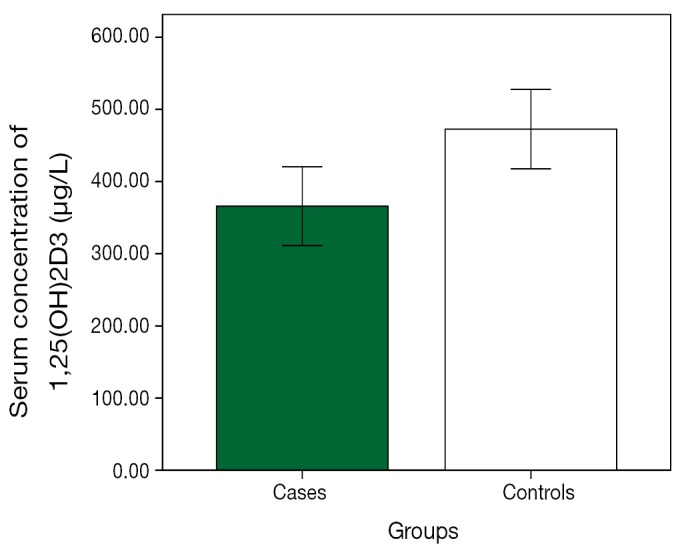
The plasma concentrations of 1,25(OH)2D3 of the two groups. Green stands for cases group, white stands for control group, the plasma concentrations of 1,25(OH)2D3 of the control group was greater compare with the test group. 1,25(OH)2D3, 1,25-dihydroxyvitamin D3.
Table 2. Ages and the plasma concentrations of 1,25(OH)2D3 of the two groups.
| Cases |
Controls |
P | ||||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| Age (years) | 31.2 | 10.4 | 33.07 | 10.6 | 0.193 | |
| 1,25(OH)2D3 (μg/L) | ||||||
| Total | 365.9 | 235.7 | 464.3 | 335.6 | 0.010 | |
| Male | 340.7 | 175.3 | 429.1 | 315.8 | 0.037 | |
| Female | 407.1 | 508.7 | 310.2 | 356.2 | 0.188 | |
1,25(OH)2D3, 1,25-dihydroxyvitamin D3.
Correlation between plasma concentrations of 1,25(OH)2D3 and the numbers of the lesion area, the smear-negative or positive and the ratio of the ratio of CD4/CD8 T lymphocyte cell
In the second part, we increase the number of TB cases to 134, males 91, females 43, the most common status 1,25(OH)2D3 is 200-600 ng/mL (Figure 2). It showed that the status of 1,25(OH)2D3 was not correlation with the different numbers of the lesion areas, the smear-negative or positive, but it shows a positive correlation with the ratio of CD4/CD8 T lymphocytes with the status of 1,25(OH)2D3 [331.0 (SD 49.7) vs. 394.8 (SD 235.7), P<0.05] (Table 3).
Figure 2.
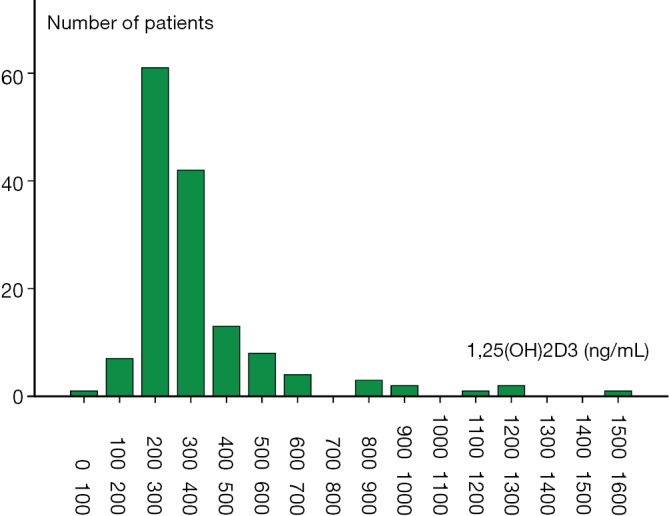
The number of patients of different levels of 1,25(OH)2D3 in the TB group. 1,25(OH)2D3, 1,25-dihydroxyvitamin D3; TB, tuberculosis.
Table 3. The basic clinical and the relationship among plasma concentrations of 1,25(OH)2D3 and the numbers of the lesion areas, the smear-negative or positive and the ratio of CD4/CD8 T lymphocyte cell.
| Group | n | Mean | SD | P |
|---|---|---|---|---|
| Total | 134 | 368.4 | 216.1 | 0.228 |
| Male | 91 | 354.8 | 184.5 | |
| Female | 43 | 400.9 | 267.3 | |
| Smear (-) or (+) | 0.105 | |||
| (+) | 56 | 301.9 | 96 | |
| (–) | 70 | 406.5 | 261.4 | |
| The ratio of CD4/CD8 | 0.008 | |||
| (I) ≤1.0 | 70 | 331 | 49.7 | |
| (II) ≥1.0 | 64 | 394.8 | 235.7 | |
| The numbers of lesion area | ||||
| (I) 1-2 | 47 | 343.9 | 193.4 | (I) and (II) P=0.107 |
| (II) 2-4 | 32 | 394.6 | 238.4 | (II) and (III) P=0.192 |
| (III) 4-6 | 55 | 387.2 | 217.5 | (I) and (III) P=0.547 |
1,25(OH)2D3, 1,25-dihydroxyvitamin D3.
Discussion
In the present study, vitamin D status was evaluated in view of its immune-regulatory role in susceptibility to microbial infection (17). Lots of researches have shown that 1,25(OH)2D3 can increase the monocytes/macrophages to killing mycobacterium TB (18,19). We have shown that the patients with TB had comparatively prevalence of concentrations decreased compared with those healthy adults (365.9 vs. 464.3, P=0.010), supported the evidence that the TB patients reflects their poor immune status compared to healthy adults (20,21). Suggest the need for vitamin D supplementation in such patients to prevent or to adjuvant the antibiotic therapy for control of TB. There has been much hope that vitamin D might fulfill at least some of these actions as a potential adjunctive treatment in active or latent TB. As see in the Figure 2, the concentrations of 200-600 µg/L were take the most percentage both in the TB groups. In the cases group the male patients shows the 1,25(OH)2D3 concentrations decreased than those healthy male adults (340.7 vs. 429.1, P<0.05), but in the female group, there is no significant difference between the two groups (P>0.05) (Table 2). These findings question the role of estrogen levels maybe affect the 1,25(OH)2D3 status and the active metabolite 1,25(OH)2D3 in vivo easy to be influenced by the environment (22). We also studied the different concentrations of 1,25(OH)2D3 on the numbers of the lesion areas and the smear-negative or positive of TB patients. It revealed that there were no significant difference between the concentrations of 1,25(OH)2D3 with the different lung fields. In the last part, we found that the 1,25(OH)2D3 levels can interact the ratio of CD4/CD8 T lymphocytes, it shows a positive correlation with the ratio of CD4/CD8 T lymphocytes, this findings also coincide with the results of Torres’s (23). This result also broad our mind that maybe the 1,25(OH)2D3 can improve the immune system of TB patient.
Several limitations of our study deserve attention. First, we studied only the activate concentrations of 1,25(OH)2D3 in the two groups, and have not studied the 25(OH)D3, However, to our knowledge, there are litter data that indicate the concentrations of 1,25(OH)2D3 and its effects on the imaging feature of TB. Secondly, we have only studied the different status of 1,25(OH)2D3 that can affect the ratio of CD4/CD8 T lymphocytes, the higher status of 1,25(OH)2D3, the higher ratio of CD4/CD8 T lymphocytes, this result will broaden our mind that the 1,25(OH)2D3 affects the ratio of CD4/CD8 T lymphocytes subtypes and let the person proved susceptible to TB. Further study will need to study the 1,25(OH)2D3 with the immune system.
Conclusions
In conclusion, the main finding of our study is that the 1,25(OH)2D3 concentrations were lower in patients with TB than in those healthy adults. And the 1,25(OH)2D3 levels can interact the ratio of CD4/CD8 T lymphocytes, it shows a positive correlation with the ratio of CD4/CD8 T lymphocytes. These data provide further evidence that lower of 1,25(OH)2D3 status may predispose to TB or the 1,25(OH)2D3 concentrations might exist as a risk factor during the development of TB, however, it is impossible to investigate the causal relationship between vitamin D3 and susceptibility for TB in this paper. Questions about the relation between TB and 1,25(OH)2D3 concentrations are largely unexplored, it can be concluded that vitamin D supplementation is a much needed, low cost, effective, and safe intervention strategy for breast cancer prevention that should be implemented.
Acknowledgements
Disclosure: The authors declare no conflict of interest.
References
- 1.Selvaraj P, Harishankar M, Singh B, et al. Effect of vitamin D3 on chemokine expression in pulmonary tuberculosis. Cytokine 2012;60:212-9 [DOI] [PubMed] [Google Scholar]
- 2.Khoo AL, Chai L, Koenen H, et al. Translating the role of vitamin D3 in infectious diseases. Crit Rev Microbiol 2012;38:122-35 [DOI] [PubMed] [Google Scholar]
- 3.Baeke F, Etten EV, Overbergh L, et al. Vitamin D3 and the immune system: maintaining the balance in health and disease. Nutr Res Rev 2007;20:106-18 [DOI] [PubMed] [Google Scholar]
- 4.Yang HF, Zhang ZH, Xiang LB, et al. 25(OH)D(3) affects the maturation and function of mouse bone marrow-derived dendritic cells stimulated by Mycobacterium bovis BCG. PLoS One 2012;7:e48062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Salahuddin N, Ali F, Hasan Z, et al. Vitamin D accelerates clinical recovery from tuberculosis: results of the SUCCINCT Study [Supplementary Cholecalciferol in recovery from tuberculosis]. A randomized, placebo-controlled, clinical trial of vitamin D supplementation in patients with pulmonary tuberculosis’. BMC Infect Dis 2013;13:22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Cao S, Luo PF, Li W, et al. Vitamin D receptor genetic polymorphisms and tuberculosis among Chinese Han ethnic group. Chin Med J (Engl) 2012;125:920-5 [PubMed] [Google Scholar]
- 7.Tiwari S, Pratyush DD, Gupta B, et al. Prevalence and severity of vitamin D deficiency in patients with diabetic foot infection. Br J Nutr 2013;109:99-102 [DOI] [PubMed] [Google Scholar]
- 8.Wagner CL, McNeil R, Hamilton SA, et al. A randomized trial of vitamin D supplementation in 2 community health center networks in South Carolina. Am J Obstet Gynecol 2013;208:137.e1-13. [DOI] [PMC free article] [PubMed]
- 9.Major JM, Graubard BI, Dodd KW, et al. Variability and reproducibility of circulating vitamin D in a nationwide U.S. population. J Clin Endocrinol Metab 2013;98:97-104 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Gallo S, Comeau K, Vanstone C, et al. Effect of different dosages of oral vitamin D supplementation on vitamin D status in healthy, breastfed infants: a randomized trial. JAMA 2013;309:1785-92 [DOI] [PubMed] [Google Scholar]
- 11.Abrams SA. Targeting dietary vitamin D intakes and plasma 25-hydroxyvitamin D in healthy infants. JAMA 2013;309:1830-1 [DOI] [PubMed] [Google Scholar]
- 12.Biancuzzo RM, Clarke N, Reitz RE, et al. Serum concentrations of 1,25-dihydroxyvitamin D2 and 1,25-dihydroxyvitamin D3 in response to vitamin D2 and vitamin D3 supplementation. J Clin Endocrinol Metab 2013;98:973-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Sato E, Imafuku S, Ishii K, et al. Vitamin D-dependent cathelicidin inhibits Mycobacterium marinum infection in human monocytic cells. J Dermatol Sci 2013;70:166-72 [DOI] [PubMed] [Google Scholar]
- 14.Yuk JM, Shin DM, Lee HM, et al. Vitamin D3 induces autophagy in human monocytes/macrophages via cathelicidin. Cell Host Microbe 2009;6:231-43 [DOI] [PubMed] [Google Scholar]
- 15.Fabri M, Stenger S, Shin DM, et al. Vitamin D is required for IFN-gamma-mediated antimicrobial activity of human macrophages. Sci Transl Med 2011;3:104ra102. [DOI] [PMC free article] [PubMed]
- 16.Kox M, van den Berg MJ, van der Hoeven JG, et al. Vitamin D status is not associated with inflammatory cytokine levels during experimental human endotoxaemia. Clin Exp Immunol 2013;171:231-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Sudfeld CR, Giovannucci EL, Isanaka S, et al. Vitamin D status and incidence of pulmonary tuberculosis, opportunistic infections, and wasting among HIV-infected Tanzanian adults initiating antiretroviral therapy. J Infect Dis 2013;207:378-85 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Jo EK. Innate immunity to mycobacteria: vitamin D and autophagy. Cell Microbiol 2010;12:1026-35 [DOI] [PubMed] [Google Scholar]
- 19.Selvaraj P, Prabhu Anand S, Harishankar M, et al. Plasma 1,25 dihydroxy vitamin D3 level and expression of vitamin d receptor and cathelicidin in pulmonary tuberculosis. J Clin Immunol 2009;29:470-8 [DOI] [PubMed] [Google Scholar]
- 20.Gallagher JC, Peacock M, Yalamanchili V, et al. Effects of vitamin D supplementation in older African American women. J Clin Endocrinol Metab 2013;98:1137-46 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Tostmann A, Wielders JP, Kibiki GS, et al. Serum 25-hydroxy-vitamin D3 concentrations increase during tuberculosis treatment in Tanzania. Int J Tuberc Lung Dis 2010;14:1147-52 [PubMed] [Google Scholar]
- 22.Jamali Z, Asadikaram G, Mahmoodi M, et al. Vitamin D status in female students and its relation to calcium metabolism markers, lifestyles, and polymorphism in vitamin D receptor. Clin Lab 2013;59:407-13 [DOI] [PubMed] [Google Scholar]
- 23.Zofková I, Kancheva RL. The effect of 1,25(OH)2 vitamin D3 on CD4+/CD8+ subsets of T lymphocytes in postmenopausal women. Life Sci 1997;61:147-52 [DOI] [PubMed] [Google Scholar]