

Abstract
Extracorporeal Shock Wave Lithotripsy (SWL) has long been used successfully to dissolve ureteral stones. We researched whether Hounsfield values of ureteral stones is a factor that affects the success of SWL. Methods: Data from 144 patients who had diagnoses of ureteral stones and underwent SWL, were retrospectively reviewed between January 2011 and December 2012. Urinary tomography of patients was processed and classified into 3 groups by Hounsfield units (Group 1, < 500 HU; Group 2, 500-1000 HU; and Group 3, > 1000 HU) and 2 groups by stone size (Group A; < 1 cm, Group B; > 1 cm). SWL success was analyzed for both of these group types. Failure was defined as any fragments of the stone that remained within the ureter. Results were analyzed by evaluating the predictive factors in both groups. Results: The study included 144 patients (100 men, 44 women) who fit the inclusion criteria. In Hounsfield unit Group 1 (12 women and 44 men), the mean age was 37.2 ± 13.2, stone size was 8.5 ± 2.5 mm, number of shocks was 3240 ± 1414 (1200-7500) and number of treatments was 1.4 ± 0.6. In Group 2 (26 women and 32 men), the mean age was 33.6 ± 7.6, stone size was 9.6 ± 3.1 mm, process number was 3375 ± 2103 (1200-8750) and shock amount was 1.6 ± 0.8. In Group 3 (6 women and 24 men), the mean age was 42.2 ± 13.6, stone size was 11.7 ± 3.0 mm, number of shocks was 4513 ± 2458 (1300-8700) and number of treatments was 2.1 ± 1.2. In size Group 1 (28 women and 74 men), the mean age was 35.8 ± 10.6, stone size was 8.1 ± 1.4 mm, process number was 3105 ± 1604, shock amount was 1.4 ± 0.5 and HU value was 580 ± 297. In Group 2 (16 women and 26 men), the mean age was 39.9 ± 14.2, stone size was 13.9 ± 2.4 mm, number of shocks was 4722 ± 2467, number of treatments was 2.3 ± 1.1 and HU value was 912 ± 270. Conclusion: Although stone density predicted the failure of SWL, size of the stone is more important criterion for successful lithotripsy of ureteral stones.
Keywords: Ureteral stone, SWL, stone size, Hounsfield unit
Introduction
Before the period when Extracorporeal Shock Wave Lithotripsy (SWL) entered therapeutic use in the 1980’s, invasive methods had been used in urolithiasis treatment. Today more than 90% of urolithiasis cases are treated with SWL and this is the primary treatment modality for stones in the kidney and ureter [1].
The success rate of this procedure is influenced by stone factors (stone size, location, composition, degree of obstruction), clinical factors (comorbidities such as concomitant infection, solitary kidney, abnormal ureteral anatomy), and technical factors (available equipment, source of energy) [2]. Several factors influencing the stone clearance and success rate such as body mass index, skin-to-stone distance, and the grade of hydronephrosis have been widely studied [3]. In addition, the attenuation value of calculi on computed tomography, measured in Hounsfield units (HUs), has also been studied to determine its ability to predict the stone-free rate after SWL [4].
Non-Contrast-enhanced Computed Tomography (NCCT) has become the radiographic modality of choice in the diagnosis of urinary stone disease [5]. CT has emerged as the modality of choice in the evaluation of acute flank pain. It is safe, rapid and accurate, with one series reporting 96% sensitivity, 99% specificity, and 98% accuracy in the diagnosis of urolithiasis [6].
Material and methods
Data from144 patients undergoing SWL for ureteral stones between June 2008 and December 2012 were retrospectively reviewed.
Indications for SWL were presence of symptoms (pain, obstruction) typically found with stone size larger than 6 mm, and lack of and spontaneous passage. Prior to the treatment, patients were assessed by urinary tract tomography (CT). Non-enhanced computed tomography (NECT) was used in the diagnosis. Stone localizations, dimensions, Hounsfield units and the effect on the urinary system on these patients were determined before the treatment. After treatment, patients were evaluated by Direct Urinary System Graphy (DUSG) and Ultrasonography (USG) for a period of 1 month. Also, non-contrasted CT was added to the evaluation methods when required. Urea, creatinine, urinalysis and urine culture examinations were carried out on patients diagnosed with ureteral stones, prior to SWL treatment. During SWL, non-steroidal analgesics (diclofenac sodium) were applied to patients who had pain scores (numerical pain ratings) of 5 and above. Before SWL, none of the patients had prophylactic antibiotics or analgesia. After the procedure, the patients received diclofenac, tamsulosin, nitrofurantoin, and were recommended to consume copious fluids.
A Storz Medical Modulith SLK was used in the SWL process. This device includes both ultrasonic and X-ray fluoroscopic focus systems. To give minimum radiation exposure with this device, the ultrasonic focus was typically applied. In order to better view the stone with ultrasound, patients were processed while their bladders were half full. SWL was not performed on those whom were pregnant, had bleeding diathesis, had significant deterioration in renal function, or had a urinary tract infection.
One to four (mean: 1.65) sessions of SWL were applied to the patients. For each session, the average shock number was 3812 (1200-8750) and shock severity was 30-75kv (mean: 60kv). Patients were examined on the 7th, 14th, 21st, and 30th days after the SWL process. Stones were analyzed with USG and DUSG. SWL was applied if the stone was not fragmented at the 7th day examination. SWL was not applied if the stone was fragmented. Success was determined by all fragments of the stone having passed through the ureter.
Patients’ age, sex, stone dimension, Hounsfield unit, and stone locations were evaluated. Patients were divided into 3 groups according to their Hounsfield unit values (Group 1; < 500 HU, Group 2; 500-1000 HU, Group 3; > 1000 HU). Also they were divided into 2 groups according to stone radius (Group A; < 1 cm, Group B; > 1 cm). Both groups’ success for SWL was analyzed. Failure was defined as the presence of any remaining stones or fragments of 3 mm or larger. The data were analyzed to determine clinical and radiological factors associated with treatment. Univariate analysis was used to evaluate the effects of single or multiple factor results. After this, multivariate logistic regression analysis was performed. This was done to determine independent predictors of treatment failure.
Statistical evaluation
The SPSS 11.5 (Statistical Package for Social Sciences, Chicago, USA) software was used for all statistical evaluations. The differences between the data of the patient groups were examined by Independent Sample t-test and box plots. The similarity between the data of the patient groups was examined by Pearson’s correlation analysis and scatter grams. Correlations with p < 0.05 values were considered statistically significant.
Results
The study included 144 patients (100 men, 44 women) who matched the inclusion criteria. Average age was 37.7 (16-73), average stone size was 9.6 mm (6-19), the average number of treatments was 1.65 (1-4), and the average number of shocks was 3812 (1200-8750).
In the Hounsfield unit Group 1 (12 women and 44 men), the mean age was 37.2 ± 13.2, stone size was 8.5 ± 2.5 mm, number of shocks was 3240 ± 1414 (1200-7500) and the mean number of treatments was 1.4 ± 0.6. In Group 2 (26 women and 32 men), the mean age was 33.6 ± 7.6, stone size was 9.6 ± 3.1 mm, the number of shocks was 3375 ± 2103 (1200-8750) and the number of treatments was 1.6 ± 0.8. In Group 3 (6 women and 24 men), the mean age was 42.2 ± 13.6, stone size was 11.7 ± 3.0 mm, number of shocks was 4513 ± 2458 (1300-8700) and number of treatments was 2.1 ± 1.2 (Table 1).
Table 1.
Data values of Housfield unit (HU) groups
| Group 1 (n = 56) Mean ± SD | Group 2 (n = 58) Mean ± SD | Group 3 (n = 30) Mean ± SD | |
|---|---|---|---|
| Age (years) | 37.2 ± 13.2 | 33.6 ± 7.6 | 42.2 ± 13.6 |
| Male/Female (M/F) | 12/44 | 26/32 | 6/24 |
| Stone diameter (mm) | 8.5 ± 2.5 | 9.6 ± 3.1 | 11.7 ± 3.0 |
| SWl shocks | 3240 ± 1414 (1200-7500) | 3375 ± 2103 (1200-8750) | 4513 ± 2458 (1300-8700) |
| SWL sessions | 1.4 ± 0.6 | 1.6 ± 0.8 | 2.1 ± 1.2 |
In size Group 1 (28 women and 74 men), the mean age was 35.8 ± 10.6, stone size was 8.1 ± 1.4 mm, number of shocks was 3105 ± 1604, number of treatments was 1.4 ± 0.5 and HU value was 580 ± 297. In Group 2 (16 women and 26 men), the mean age was 39.9 ± 14.2, stone size was 13.9 ± 2.4 mm, number of shocks was 4722 ± 2467, number of treatment was 2.3 ± 1.1 and HU value was 912 ± 270 (Table 2).
Table 2.
Variables per group according to the diameter of the Stone (SD Groups)
| M/F | Age (years) | Stone Diameter (mm) | SWl Shocks | SWL Sessions | Housfield Unit (HU) | |
|---|---|---|---|---|---|---|
| SD Group I (n = 102) ≤ 10 mm | 28/74 | 35.8 ± 10.6 | 8.1 ± 1.4 | 3105 ± 1604 | 1.4 ± 0.5 | 580 ± 297 |
| SD Group II (n = 40) > 10 mm | 16/26 | 39.9 ± 14.2 | 13.9 ± 2.4** | 4722 ± 2467* | 2.3 ± 1.1* | 912 ± 270 |
Independents Samples Test:
P < 0.05;
p < 0.01.
Anatomical placements of the stones were proximal-right ureter (32), mid-right ureter (18), distal-right ureter (28), proximal-left ureter (24), mid-left ureter (12), and distal-left ureter (30).
There were 57 patients with a stone size less than 1 cm, and 23 patients who had a stone size greater than 1 cm. As a result, the stone was isolated for 136 patients (94.5%), and 8 patients (5.5%) required extra treatment. Failure to fragment the stone occurred in 5 patients. Successful fragmentation which, nonetheless, required further treatment occurred in 3 patients. Eighty-six patients (59.7%) had macroscopic hematuria in their initial urine sample after an SWL session. Two patients developed urinary tract infections within one week after an SWL session. One of these patients was treated as an inpatient with parenteral antibiotic therapy; the other one was treated with oral antibiotic therapy. Out of 8 patients who had unsuccessful SWL sessions, two had proximal, two had middle and four had distal ureteral stones. These stones’ sizes were all greater than 15 mm.
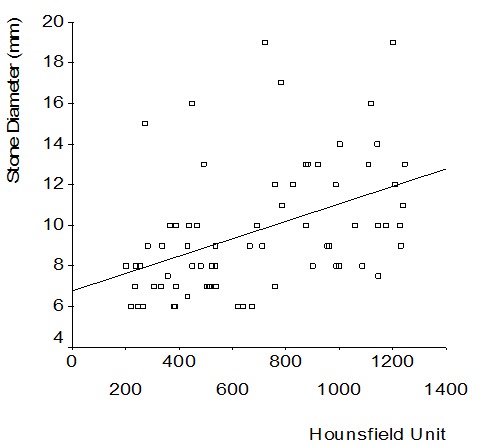
There was significant correlation between stone size and shocks (r: 0.544, p < 0.001). There was significant correlation between stone size and number of sessions (r = 0.609, p < 0.001). There was significant correlation between process amounts and Hounsfield units (r = 0.219, p = 0.008). There was also significant correlation between stone size and Hounsfield units (r = 0.447, p < 0.001).
Hounsfield groups 1 and 2 showed no significant differences between process amount and sessions (p = 0.688 and p = 0.131). Group 1 and group 3 had significant correlation between process amounts and sessions (p = 0.003 and p = 0.000). Groups 2 and 3 showed significant correlation between process amounts and sessions (p = 0.026 and p = 0.10). The comparison of differences in data values between groups was shown in Table 3 and depicted in Figures 1, 2, 3 and 4.
Table 3.
The comparison of differences in data values between groups
| Age | Size | Shock | Sessions | |
|---|---|---|---|---|
| Group 1-Group 2 | 0.080 | 0.047* | 0.688 | 0.131 |
| Group 1-Group 3 | 0.105 | 0.000** | 0.003* | 0.000** |
| Group 2-Group 3 | 0.000** | 0.003* | 0.026* | 0.010* |
P < 0.05;
p < 0.01.
Figure 1.

Data of Hounsfield unit groups (boxplots).
Figure 2.

Data of stone diameter groups (boxplots).
Figure 3.

The correlation plot of Hounsfield Unit and stone diameter and shockwave number.
Figure 4.
The correlation plot of Hounsfield unit.
The stone radius was greater than 1 cm in 8 patients who had unsuccessful ESWL sessions. Out of these 8 patients, 5 patients’ stone densities were over 1000 HU (Group 3), 2 patients’ stone densities were between 500 and 1000 HU (Group-2) and one patient’s stone density was under 500 HU (Group-1).
Discussion
Effective treatment for ureteral stones should resolve clinical complaints of the patient and avoid the negative impacts of the obstruction on the kidney [7]. Ureteral stones that are under 3 mm or less will pass spontaneously 86-97% of the time without symptoms or sequelae and do not require medical treatment. At 4 mm and above, ureteral stones will pass spontaneously 80% of the time [8]. A meta-analysis which considered only the stone size, regardless of the location, determined that stones that are less than 5 mm pass 68% of the time. In contrast, stones that are 5-10 mm pass 47% of the time [1].
Spontaneous passage depends on stone size, location, and right laterality [8]. Solitary or bilateral ureteral stones which do not pass spontaneously and create renal dysfunction require medical intervention. While expectantly managing spontaneous passage in patients with associated pain, intervention can be carried out per patient’s preference. Intervention methods available for ureteral stones are SWL, URS + lithotripsy and open or minimally invasive surgical procedures. SWL is more advantageous compared to the alternatives, because it is an outpatient procedure with minimal complications compared to surgery and anesthesia. Today, 90% of ureteral stones are treated with SWL [1].
Renal stones were evaluated in the vast majority of studies on factors affecting the success of SWL. Factors affecting the success of SWL were separated into 3 groups to improve intelligibility. These include factors related to the stones (size, surface area, volume, location, composition, degree of obstruction), clinical factors (concomitant infection, solitary kidney, the presence of a stent, abnormal urethral anatomy) and technical factors (hand equipment, energy supply and shock intensity) [10-12]. In recent studies, the data for body mass index (BMI), skin-stone distance (SSD), the stone Hounsfield units (HU) are also considered [5,13]. Even though they appear to be clinical factors, BMI and SSD are physical characteristics of conditions associated with lithotripsy.
Unfavorable composition of the stone is the major factor for failure of SWL. It is therefore important that the composition of the stone must be known before starting a treatment. This information can be assessed by stone analysis in patients with recurrent disease. In studies in the 1990s, success of SWL was estimated by looking at density on DUSG and shape of the stone [13-15]. The accuracy of the estimation of stone composition in DUSG and the success rate of the estimation were 39% and 40% respectively [15].
This was clearly a poor predictor of the success of SWL. Today, diagnosis of the stone can be done by helical NCCT with 96% sensitivity, 99% specificity and 98% accuracy. NCCT is an advanced image reconstruction technology that is capable of producing multiple, thin-slice images with advanced computer software. Stone shape, stone size, and attenuation values can be measured in order to predict the success of SWL.
The relationship between stone compositions and density of stone has been accomplished by in vitro studies. Thus, HU values of pure stones are distinct because they do not overlap [16-20]. In one study, these values were 112-436 HU for uric acid stones, 510-681 HU for struvite stones, 994-1180 HU for cystine calculi, 1252-1640 HU for calcium phosphate, 1813 HU for calcium oxalate dihydrate and 1743-2857 HU for calcium oxalate monohydrate. In another analytical study, stones were classified on the basis of urate, phosphate, and oxalate. These classes (urate, Ca, phosphate, oxalate, H, N, C, Mg) were studied, and different HU values were found (urate 513 ± 197 HU; phosphate 1660 ± 292 HU; oxalate 1684 ± 290 HU) [21]. However, stones often comprise a combination of crystals. Approximately 80% of the stones in the urinary tract are formed by two or more different combinations of crystal phase. Thus, every stone should preferably be fragmented by an appropriate number and severity of shocks based on their composition [22].
Recent studies were carried out to evaluate the role of HU values in predicting the success of SWL [3,4,23-30]. These studies (prospective and retrospective) clearly showed HU values affected ESWL results (number of shocks, session, success), and tried to determine a threshold value. According to the values of these first prospective studies, stones were classified by HU values (< 500, 500-1000, > 1000) and success of SWL was found to be 100%, 85.7%, and 54.5% respectively [22]. If the threshold value was taken as 1000 HU, then there was a statistically significant difference between 94.7% and 54.5%. In other prospective studies, the threshold value was taken as approximately 1000 HU [25,28,30].
Retrospective studies have tried to derive the value of density in predicting the success rates of patients who often get ESWL. For this purpose, fragmented and unfragmented stone density values were correlated. These values, in many of Pareek’s studies, were 551.20 ± 46.66 HU versus 926.20 ± 51.42 HU, and 577.8 ± 182.5 HU versus 910.4 ± 190.2 HU4. In other retrospective studies, the threshold value was taken as 750 or 1000 HU [24,26,27,29]. In studies in which the threshold value was taken as 1200 HU, the success rate was determined (80.4% and 66.2%). Also, shock number and increase in shock density were both found to be meaningful [23]. Stone density was found to be a significant predictor of success as well as the failure on multivariate analysis [26]. Beyond this, it is remarkable that stone density was a better independent predictor than the size of the stone [17,24,26-30].
In most of these studies, ureteral stones were the topic of discussion [3,4,23-30]. In some of these studies, only HU and SWL values for proximal-ureter stones were evaluated [4,24-28]. We reviewed data for ureteral stones in 144 patients in all three locations. It was a considerably larger study compared to the current literature. We reviewed the relationship between stone size and density, and shock to shock amount to predict the success or failure of SWL. Also we compared the results with current information.
When the results were evaluated, there was success in 136 out of 144 patients (94.4%). Eight cases were unsuccessful: 2 proximal, 2 mid, and 4 distal stones were remaining (n = 8). According to the localization, our success rates were 96.4% on proximal, 93.3% on mid, and 93.1% on distal stones. These values were higher than those reported in previous literature. When comparing between groups, the characteristics of age, sex, and laterality were very similar (p > 0.05). Shock and shockwave values for the larger stone radius group were higher than in the smaller group (p < 0.01). Analyzing density values showed that the group with > 1000 HU values was significantly different from those with HU values of < 500 HU (p = 0.000) and 500-1000 HU (p = 0.010). There were no meaningful differences between the last two groups.
When correlation was evaluated, there was a significant relevance for several variables, including (from strongest to the weak respectively) stone radius to shock numbers (r = 0.544), stone radius to density (r = 0.447) and density to shock numbers (r = 0.219).
Conclusion
According to our study, stone size is one of two factors that affect the success of SWL. When correlation was evaluated, the size of ureteral stones (r = 0.544) was the most significant affecting factor predicting the result of SWL, rather than the stone density (r = 0.219). Contrary to previous results reported in the literature [17,24,26-30], we believe that stone radius is the more independent predictor of successful lithotripsy for ureteral stones rather than stone density. When the unsuccessful group was evaluated, the > 1000 HU value was highlighted as a threshold. Density of ureteral stones was seen as an important criterion in predicting the failure of SWL [25]. As a result, although stone density does predict the failure of SWL, the size of the stone is the more important predictive variable.
Acknowledgements
Thanks are due to Bekir Sami Uyanik for helpful statistics and data collection. The data base and evaluation of results were approved by the ethics committee of Hisar Intercontinental Hospital (08/2011).
References
- 1.Segura JW, Preminger GM, Assimos DG, Dretler SP, Kahn RI, Lingeman JE, Macaluso JN Jr. Ureteral Stones clinical guidelines panel summary report on the management of ureteral calculi. J Urol. 1997;158:1915–1921. doi: 10.1016/s0022-5347(01)64173-9. [DOI] [PubMed] [Google Scholar]
- 2.Lingeman JE, Matlaga BR. Surgical management of upper urinary tract calculi. In: Wein AJ, Kavoussi LR, Novick AC, Partin AW, Peters CA, editors. Campbell-Walsh Urology. 10th ed. Philadelphia: Saunders; 2010. pp. 1375–1377. [Google Scholar]
- 3.Pareek G, Armenakas NA, Panagopoulos G, Bruno JJ, Fracchia JA. Extracorporeal shock wave lithotripsy success based on body mass index and Hounsfield units. Urology. 2005;65:33–36. doi: 10.1016/j.urology.2004.08.004. [DOI] [PubMed] [Google Scholar]
- 4.Pareek G, Armenakas NA, Fracchia JA. Hounsfield units on computerized tomography predict stone-free rates after extracorporeal shock wave lithotripsy. J Urol. 2003;169:1679–1681. doi: 10.1097/01.ju.0000055608.92069.3a. [DOI] [PubMed] [Google Scholar]
- 5.Pareek G, Hedican SP, Lee FT, Stephen JR, Nakada Y. Shock Wave Lithotripsy success determined by skin-to-stone distance on computed tomography. Urology. 2005;66:941–944. doi: 10.1016/j.urology.2005.05.011. [DOI] [PubMed] [Google Scholar]
- 6.Dalrymple NC, Verga M, Anderson KR, Bove P, Covey AM, Rosenfield AT, Smith RC. The value of unenhanced helical computerized tomography in the management of acute flank pain. J Urol. 1998;159:735–740. [PubMed] [Google Scholar]
- 7.Shokeir AA. Renal colic: pathophysiology, diagnosis and treatment. Eur Urol. 2001;39:241–249. doi: 10.1159/000052446. [DOI] [PubMed] [Google Scholar]
- 8.Miller OF, Kane CJ. Time to stone passage for observed ureteral calculi: a guide of patient education. J Urol. 1999;162:688–690. doi: 10.1097/00005392-199909010-00014. [DOI] [PubMed] [Google Scholar]
- 9.Preminger GM, Tiselius HG, Assimos DG, Alken P, Buck AC, Gallucci M, Knoll T, Lingeman JE, Nakada SY, Pearle MS, Sarica K, Türk C, Wolf JS Jr. American Urological Association Education and Research, Inc; European Association of Urology. 2007 Guideline for the Management of Ureteral Calculi. Eur Urol. 2007;52:1610–1631. doi: 10.1016/j.eururo.2007.09.039. [DOI] [PubMed] [Google Scholar]
- 10.Augustin H. Prediction of stone-free rate after ESWL. Eur Urol. 2007;52:318–320. doi: 10.1016/j.eururo.2007.03.059. [DOI] [PubMed] [Google Scholar]
- 11.Kanao K, Nakashima J, Nakagawa K, Asakura H, Miyajima A, Oya M, Ohigashi T, Murai M. Preoperative nomograms for predicting stone-free rate after extracorporeal shock wave lithotripsy. J Urol. 2006;176:1453–1456. doi: 10.1016/j.juro.2006.06.089. [DOI] [PubMed] [Google Scholar]
- 12.Delakas D, Karyotis I, Daskalopoulos G, Lianos E, Mavromanolakis E. Independent predictors of failure of shockwave lithotripsy for ureteral stones employing a second generation lithotripter. J Endourol. 2003;17:201–205. doi: 10.1089/089277903765444302. [DOI] [PubMed] [Google Scholar]
- 13.Patel T, Kozakowski K, Hruby G, Gupta M. Skin to stone distance is an independent predictor of stone-free status following shockwave lithotripsy. J Endourol. 2009;23:1383–1385. doi: 10.1089/end.2009.0394. [DOI] [PubMed] [Google Scholar]
- 14.Dretler SP, Polykoff G. Calcium oxalate stone morphology: fine tuning our therapeutic distinctions. J Urol. 1996;155:828–833. doi: 10.1016/s0022-5347(01)66319-5. [DOI] [PubMed] [Google Scholar]
- 15.Ramakumar S, Patterson DE, LeRoy AJ, Bender CE, Erickson SB, Wilson DM, Segura JW. Prediction of stone composition from plain radiographs: a prospective study. J Endourol. 1999;13:397–401. doi: 10.1089/end.1999.13.397. [DOI] [PubMed] [Google Scholar]
- 16.Newhouse JH, Prien EL, Amis ES Jr, Dretler SP, Pfister RC. Computed tomographic analysis of urinary calculi. Am J Roentgenol. 1984;142:545–548. doi: 10.2214/ajr.142.3.545. [DOI] [PubMed] [Google Scholar]
- 17.Marchiñena PG, Peres NB, Liyo J, Ocantos J, Gonzalez M, Jurado A, Daels F. CT scan as a predictor of composition and fragility of urinary lithiasis treated with extracorporeal shock wave lithotripsy in vitro. Arch Esp Urol. 2009;62:215–221. doi: 10.4321/s0004-06142009000300007. [DOI] [PubMed] [Google Scholar]
- 18.Mostafavi MR, Ernst RD, Saltzman B. Accurate determination of chemical composition of urinary calculi by spiral computerized tomography. J Urol. 1998;159:673–675. [PubMed] [Google Scholar]
- 19.Motley G, Dalrymple N, Keesling C, Fischer J, Harmon W. Hounsfield unit density in the determination of urinary stone composition. Urology. 2001;58:170–173. doi: 10.1016/s0090-4295(01)01115-3. [DOI] [PubMed] [Google Scholar]
- 20.Nakada SY, Hoff DG, Attai S, Heisey D, Blankenbaker D, Pozniak M. Determination of stone composition by noncontrast spiral computed tomography in the clinical setting. Urology. 2000;55:816–819. doi: 10.1016/s0090-4295(00)00518-5. [DOI] [PubMed] [Google Scholar]
- 21.Abdel-Halim RE, Abdel-Aal RE. Classification of urinary stones by cluster analysis of ionic composition data. Computer Methods and Programs in Biomedicine. 1999;58:69–81. doi: 10.1016/s0169-2607(98)00075-3. [DOI] [PubMed] [Google Scholar]
- 22.Ringdén I, Tiselius HG. Composition and clinically determined hardness of urinary tract stones. Scand J Urol Nephrol. 2007;41:316–323. doi: 10.1080/00365590601154551. [DOI] [PubMed] [Google Scholar]
- 23.Joseph P, Mandal AK, Singh SK, Mandal P, Sankhwar SN, Sharma SK. Computed tomography attenuation value of renal calculus: can it predict successful fragmentation of the calculus by extracorporeal shock wave lithotripsy? A preliminary study. J Urol. 2002;167:1968–1971. doi: 10.1016/s0022-5347(05)65064-1. [DOI] [PubMed] [Google Scholar]
- 24.Gupta NP, Ansari MS, Kesarvani P, Kapoor A, Mukhopadhyay S. Role of computed tomography with no contrast medium enhancement in predicting the outcome of extracorporeal shock wave lithotripsy for urinary calculi. BJU Int. 2005;95:1285–1288. doi: 10.1111/j.1464-410X.2005.05520.x. [DOI] [PubMed] [Google Scholar]
- 25.El-Nahas AR, El-Assmy AM, Mansour O, Sheir KZ. A prospective multivariate analysis of factors predicting stone disintegration by extracorporeal shock wave lithotripsy: the value of high-resolution noncontrast computed tomography. Eur Urol. 2007;51:1688–1693. doi: 10.1016/j.eururo.2006.11.048. discussion 1693-1694. [DOI] [PubMed] [Google Scholar]
- 26.Kacker R, Zhao L, Macejko A, Thaxton CS, Stern J, Liu JJ, Nadler RB. Radiographic parameters on noncontrast computerized tomography predictive of shockwave lithotripsy success. J Urol. 2008;17:1866–1871. doi: 10.1016/j.juro.2008.01.038. [DOI] [PubMed] [Google Scholar]
- 27.Wiesenthal JD, Ghiculete D, D’A Honey RJ, Pace KT. Evaluating the importance of mean stone density and skin-to-stone distance in predicting successful shock wave lithotripsy of renal and ureteric calculi. Urol Res. 2010;38:307–313. doi: 10.1007/s00240-010-0295-0. [DOI] [PubMed] [Google Scholar]
- 28.Shah K, Kurien A, Mishra S, Ganpule A, Muthu V, Sabnis R, Desai M. Predicting effectiveness of extracorporeal shockwave lithotripsy by stone attenuation value. J Endourol. 2010;24:1169–1173. doi: 10.1089/end.2010.0124. [DOI] [PubMed] [Google Scholar]
- 29.Ouzaid I, Al-qahtani S, Dominique S, Hupertan V, Fernandez P, Hermieu JF, Delmas V, Ravery V. A 970 Hounsfield units (HU) threshold of renal stone density on non-contrast computed tomography (NCCT) improves patients’ selection for extracorporeal shockwave lithotripsy (ESWL): evidence from a prospective study. BJU Int. 2012;110:E438–442. doi: 10.1111/j.1464-410X.2012.10964.x. [DOI] [PubMed] [Google Scholar]
- 30.Vivaldi B, Fernández MI, López JF, Fuentes F, Urzúa C, Krebs A, Domenech A, Figueroa PA, Pizzi P, Westendarp M, Zambrano N, Castro M, Coz LF. Single-session extra corporeal shock wave lithotripsy for urinary calculi: factors predicting success after three weeks of follow-up. Actas Urol Esp. 2011;35:529–533. doi: 10.1016/j.acuro.2011.04.008. [DOI] [PubMed] [Google Scholar]