

Abstract
Obstructive sleep apnea (OSA) is characterized by recurrent upper airway obstruction occurring at the level of the pharynx during sleep. Although cephalometric analysis is an important method in the diagnosis of craniofacial deformities, CT and magnetic resonance imaging have been highlighted as the major imaging methods to investigate the possible causes of OSA, which, in most cases, is multifactorial. Magnetic resonance and CT both allow an excellent evaluation of the various anatomical planes of the site of obstruction, which enables better clinical assessment and surgical approach. This pictorial essay aims to describe the aspects that must be evaluated in the diagnostic imaging of patients presenting with the major predisposing factors for OSA.
Keywords: Sleep apnea syndromes; Magnetic resonance imaging; Tomography, X-ray computed
Abstract
A apneia obstrutiva do sono (AOS) é caracterizada por obstruções recorrentes das vias aéreas superiores durante o sono que ocorrem no nível da faringe. Apesar de a análise cefalométrica ser um importante método no diagnóstico das deformidades craniofaciais, a TC e a ressonância magnética vêm se destacando como os principais métodos de imagem para a investigação das eventuais causas da AOS que, na maioria das vezes, é multifatorial. Esses métodos permitem uma excelente avaliação nos diversos planos anatômicos do eventual sítio da obstrução, o que permite uma melhor avaliação clínica e abordagem cirúrgica. O presente ensaio pictórico tem como objetivo descrever os aspectos que devem ser avaliados no diagnóstico por imagem dos principais fatores predisponentes para a AOS.
Obstructive sleep apnea (OSA) is characterized by recurrent upper airway obstruction occurring at the level of the pharynx during sleep.( 1 ) It is a chronic progressive disease associated with high rates of cardiovascular morbidity.( 2 )
The diagnosis of OSA is confirmed by polysomnography. However, imaging studies are highly relevant supporting methods in the evaluation of patients with OSA.
Cephalometric analysis, performed using X-rays, is an important method in the diagnosis of craniofacial deformities. With this method, it is possible to measure the skull base, as well as to determine the position of the hyoid bone, the configuration of the mandible, the posterior pharyngeal airspace, the dimensions of the tongue, the length and thickness of the uvula, etc. Anatomical changes in these sites can predispose patients to OSA.( 3 )
Magnetic resonance imaging (MRI) and CT have been highlighted for their ability to perform multiplanar imaging. Because it allows a better anatomical resolution and it does not use ionizing radiation, MRI has been used as the major imaging method for this type of investigation.( 4 ) This article aims to describe the major MRI and CT findings in the diagnostic evaluation of patients with OSA.
In most cases, OSA is multifactorial,( 5 ) being the result of upper airway collapse or narrowing occurring during sleep. In general, the greatest narrowing of the pharyngeal air passage is seen at the level of the lower soft palate. In the protocols to be used, axial and sagittal images of the oropharyngeal and hypopharyngeal air passages should always be included, and imaging studies should be performed as soon as possible.
Midsagittal slices are of fundamental importance, because they make it possible to characterize the airway contour, the maxillomandibular relationship (to evaluate patients for retrognathia and micrognathia), the volume of the soft palate, the palate shapes, the position of the hyoid bone, and the position and volume of the dorsum of the tongue. Figure 1 shows a midsagittal slice of a normal MRI scan. Axial slices should be acquired at the levels of the nasopharynx, hypopharynx, palates, dorsum of the tongue, and vocal cords.
Figure 1. Midsagittal slice of a magnetic resonance image from a normal subject. Note the maxillomandibular relationship, the symmetry of the palate, and the diameter of the air passage.

One of the most important changes that must be investigated on imaging studies in patients with OSA is the pattern of the airway passage on the axial CT or MRI slices. Physiologically, the pattern that is observed in normal subjects is laterolateral (Figure 2).( 2 ) Increased soft tissue (fat, muscle, or lymphoid tissue) volume in the oropharyngeal region can make the oropharynx exhibit a pathological pattern anteroposteriorly (Figure 3).
Figure 2. Axial CT slice showing the physiological pattern of the air passage, the laterolateral axis being the longest.

Figure 3. Axial CT slice at the oropharyngeal level showing the pathological pattern of the air passage anteroposteriorly.

The conditions that can predispose to OSA include the following:
Vocal cord paralysis
Micrognathia and retrognathia (Figure 4)
Soft palate abnormalities
Increased soft palate size (Figure 5)
Deviation of the nasal septum
Tonsil or adenoid hypertrophy, or both
Tumors or cysts in the pharyngeal region (Figure 6)
Macroglossia(Figure 7)
Hard palate deformities: high-arched palate (Figure 7)
Obesity( 2 ) (because an excess of soft tissue in the pharynx hampers the pharyngeal air passage from remaining open)
Glossoptosis (tongue ptosis has been highlighted as a cause of OSA in children)( 6 - 8 )
A low hyoid bone, ectopic thyroid, and craniofacial abnormalities ( 8 )
Acromegaly
Figure 4. Sagittal slice of a magnetic resonance image showing retrognathia (arrow), the dorsum of the tongue in contact with the soft palate (arrowheads), and narrowing of the nasopharyngeal air passage.
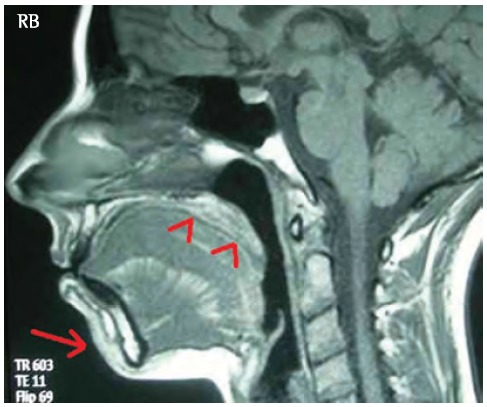
Figure 5. Sagittal slice of a magnetic resonance image showing a pathological pattern of the soft palate. The patient had a high-arched palate (arrow) and increased soft palate size (arrow heads), with consequent narrowing of the air passage.
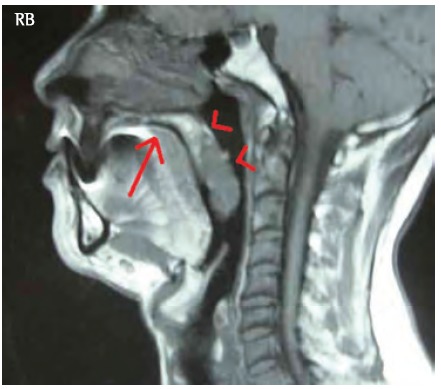
Figure 6. Sagittal reconstruction of a CT scan showing a massive polyp protruding toward the nasopharynx and oropharynx, causing significant narrowing of the lumen of the air passage (arrow).
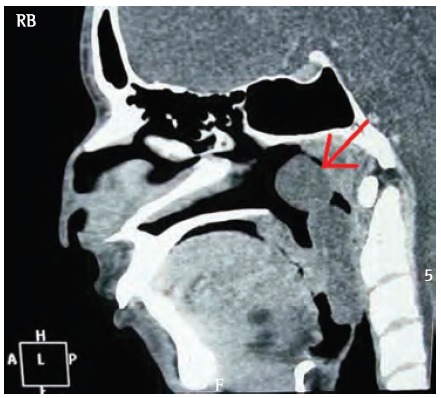
Figure 7. Midsagittal slice of a magnetic resonance image from a patient with macroglossia. Note that the dorsum of the tongue is in contact with the soft palate and epiglottis (arrows). Also note the narrowing of the air passage (arrowhead).

Although polysomnography is the method used to confirm the diagnosis of OSA,( 2 ) CT and especially MRI have established themselves as important supporting methods in the clinical diagnosis, preoperative evaluation, and post-treatment follow-up of patients who do not respond well to initial therapy. Both CT and MRI can provide an excellent evaluation of the various anatomical planes of the site of obstruction, which enables better clinical assessment as well as better planning for a possible surgical approach.
Footnotes
Financial support: None
Study carried out at the Universidade Federal da Paraíba - UFPB, Federal University of Paraíba - João Pessoa, Brazil
Contributor Information
Carlos Fernando de Mello, Junior, Federal University of Paraíba, School of Medicine, João Pessoa, Brazil. Department of Radiology, Universidade Federal da Paraíba – UFPB, Federal University of Paraíba – School of Medicine, João Pessoa, Brazil.
Hélio Antonio Guimarães, Filho, Ecoclínica, João Pessoa, Brazil. Ecoclínica, João Pessoa, Brazil.
Camila Albuquerque de Brito Gomes, Nova Esperança School of Medicine, João Pessoa, Brazil. Nova Esperança School of Medicine, João Pessoa, Brazil.
Camila Caroline de Amorim Paiva, Federal University of Paraíba, João Pessoa, Brazil. Universidade Federal da Paraíba – UFPB, Federal University of Paraíba – School of Medicine, João Pessoa, Brazil.
References
- 1.Suto Y, Matsuo T, Kato T, Hori I, Inoue Y, Ogawa S, et al. Evaluation of the pharyngeal airway in patients with sleep apnea: value of ultrafast MR imaging. AJR Am J Roentgenol. 1993;160(2):311–314. doi: 10.2214/ajr.160.2.8424340. [DOI] [PubMed] [Google Scholar]
- 2.Mancini MC, Aloe F, Tavares S. Apnéia do sono em obesos. Arq Bras Endocrinol Metab. 2000;44(1):81–90. http://dx.doi.org/10.1590/S0004-27302000000100013 [Google Scholar]
- 3.Salles C, Campos PS, Andrade NA, Daltro C. Obstructive sleep apnea and hypopnea syndrome: cephalometric analysis. Rev Bras Otorrinolaringol. 2005;71(3):369–372. doi: 10.1016/S1808-8694(15)31338-0. http://dx.doi.org/10.1590/S0034-72992005000300018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Abbott MB, Donnelly LF, Dardzinski BJ, Poe SA, Chini BA, Amin RS. Obstructive sleep apnea: MR imaging volume segmentation analysis. Radiology. 2004;232(3):889–895. doi: 10.1148/radiol.2323031581. http://dx.doi.org/10.1148/radiol.2323031581 [DOI] [PubMed] [Google Scholar]
- 5.Suto Y, Matsuda E, Inoue Y, Suzuki T, Ohta Y. Sleep apnea syndrome: comparison of MR imaging of the oropharynx with physiologic indexes. Radiology. 1996;201(2):393–398. doi: 10.1148/radiology.201.2.8888230. [DOI] [PubMed] [Google Scholar]
- 6.Donelly LF. Obstructive sleep apnea in pediatric patients: evaluation with cine MR sleep studies. Radiology. 2005;236(3):768–778. doi: 10.1148/radiol.2363040306. http://dx.doi.org/10.1148/radiol.2363040306 [DOI] [PubMed] [Google Scholar]
- 7.Donnelly LF, Strife JL, Myer CM 3rd. Glossoptosis (posterior displacement of the tongue) during sleep: a frequent cause of sleep apnea in pediatric patients referred for dynamic sleep fluoroscopy. AJR Am J Roentgenol. 2000;175(6):1557–1560. doi: 10.2214/ajr.175.6.1751557. [DOI] [PubMed] [Google Scholar]
- 8.Donnelly LF, Surdulescu V, Chini BA, Casper KA, Poe SA, Amin RS. Upper airway motion depicted at cine MR imaging performed during sleep: comparison between young patients with and those without obstructive sleep apnea. Radiology. 2003;227(1):239–245. doi: 10.1148/radiol.2271020198. http://dx.doi.org/10.1148/radiol.2271020198 [DOI] [PubMed] [Google Scholar]