

Do new standards of care incorporating immunomodulatory agents and proteasome inhibitors benefit all elderly patients with multiple myeloma?
Multiple myeloma (MM) accounts for 1% of all types of cancer and for 2% of all cancer deaths. These numbers are approximately 13% for all hematologic malignancies and 20% for hematologic malignancy-related deaths.1,2 MM is a disease of the elderly reflected by a median age at diagnosis of approximately 70 years, with 35–40% of patients being older than 75 years.3
The introduction of the immunomodulatory agents (IMiDs; thalidomide, lenalidomide and pomalidomide) and the proteasome inhibitors (PIs; bortezomib and carfilzomib) has not only greatly improved the prognosis of younger patients with MM, also in elderly MM patients aged 65 years or over. The addition of bortezomib or thaldiomide to melphalan and prednisone (MP) improved overall survival (OS) by 13.3 and 6.6 months, respectively.4,5 Although the addition of lenalidomide to melphalan and prednisone did not improve OS, progression-free survival (PFS) significantly improved by 18 months, provided that maintenance therapy was given.6 However, when considering the outcome as described in population-based registries, reflecting real-life situations, the elderly patients appear to benefit less. Recently, in the Italian and Dutch population-based registry (PBR), the overall survival of very old patients (≥75 years of age) was found to be similar over time, without any improvement in OS after the introduction of novel agents in 20062 (SG Verelst, personal communication, 2014). This lack of impact does not seem to be explained by a biologically different, more aggressive disease in the elderly. Although differences in cytogenetic abnormalities have been observed between younger and older patients,7 there is currently no evidence for a higher incidence of biologically high-risk disease in the elderly. Moreover, the French Intergroupe Francophone du Myélome (IFM) showed that the incidence of t(4;14) was even significantly less in patients aged over 75 years (8.3%) and aged 66–74 years (10.9%) versus those aged 65 years or under (14.3%). The incidence of del17p was similar (6.1% in patients aged over 75 years, 5.9% in patients aged 66–74 years and 6% in patients aged 65 years or under). Data on del1p and ampl1q were not available.8 Finally, no increase according to age was found in the percentage of prognostic adverse hypermethylation of the tumor modulating genes GPX3, RBP1, SPARC, and TGFBI.9
The limited benefit of novel agents in the elderly, as described in the PBR, might be explained by the fact that the majority of elderly patients are not being included in randomized clinical trials (RCT) because they do not fulfill the eligibility criteria due to co-morbidities. Usually, in these patients, treatment is either not given, or is given but without the addition of novel agents or with a lower dose of novel agents.10 That this fact at least partly explains the difference in outcome between RCT and PBR is, indeed, supported by several observations showing that if novel therapy is given to the elderly outside of RCT, there is an increase in OS, even in the oldest patients. Data analysis of elderly patients actually receiving lenalidomide and/or bortezomib from the Mayo Clinic (89% of all patients used novel agents during the time period 2006–2010 vs. 29% in the period 2001–2005) showed an increase in OS over time, specifically in those aged over 65 years (median OS 5 vs. 3.2 years). Improved survival was seen among patients up to 75 years of age and also in those over 75 years of age.11 In addition, Liwing et al. reported that 1127 patients receiving at least two lines of therapy with bortezomib, thalidomide or lenalidomide had a superior OS (63% at 5 years) compared to those treated with conventional drugs (22% at 5 years).12 Lastly, the IFM presented registry data at ASH 2012 showing an increase in PFS in elderly patients, mainly being treated with thalidomide, irrespective of age.13 Of course, such data analyses are biased by the fact that the reasons for either treatment or no treatment are unknown. However, these data do indicate that also a subgroup of elderly patients do benefit from novel therapies. The challenge, therefore, is to identify those patients who will benefit from therapy.
Does higher toxicity and discontinuation rate negatively affect outcome in patients aged 75 years or over?
Immunomodulatory agents
Data from some clinical trials indicate that even elderly patients who do receive therapy do worse compared to younger patients. The higher incidence of heart, lung, liver, or renal dysfunction, leading to toxic effects of standard treatment regimens requiring treatment discontinuation probably plays a role. This is exemplified by the fact that in the MM015 study comparing melphalan, prednisone and lenalidomide (Revlimid©) with or without maintenance therapy (MPR-R or MPR) versus MP, the patients aged 75 years or over did not benefit from MPR-R as compared to those aged 65–75 years (median PFS 19 vs. 31 months, respectively). Accordingly, a higher percentage of discontinuation rate (22% vs. 12%) and the lower cumulative dose of melphalan (50% vs. 83% of planned dose) and lenalidomide (52% vs. 75% of planned dose) was reported in patients aged 75 years or over.6 The incidence of grade 4 toxicity can be lowered by decreasing the dose of MPR and omitting melphalan in the first induction courses altogether (neutropenia 10% vs. 35% and thrombocytopenia 0% vs. 11% in the MM015). However, whether this negatively affects PFS and OS has to be investigated in randomized trials.14
In contrast, data from the IFM showed that the addition of thalidomide to MP also improved OS in patients aged over 75 years (MPT median OS 44.0 vs. 29.1 months in MP-treated patients), but, importantly, OS was shorter compared to patients aged 75 years or under (median 51.6 vs. 33.2).15 This was confirmed in the meta-analysis on MPT.5,16
Preliminary results on pomalidomide were recently presented at ASH 2013. In contrast to the data on lenalidomide and thalidomide, pomalidomide with low-dose dexamethasone was found to have similar OS rates between the two age groups: 13.4 months in patients aged 70 years or under versus 12.6 months in patients aged over 70 years.17,18
Bortezomib
Analyses from the VISTA trial comparing bortezomib-melphalan-prednisone (VMP) versus MP showed similar outcome: a benefit of addition of bortezomib, irrespective of age. However, age did negatively affect outcome also in the bortezomib-treated patients. The latest update of a planned subgroup analysis showed a persistent benefit from bortezomib irrespective of age (median OS in patients aged >65 to <75 years 58.6 vs. 47.7 months; in patients aged ≥75 years 50.7 vs. 32.9 months).4 It is clear from the data that OS is shorter in those aged 75 years or over. Although non-significant in the original publication, the difference became significant with a longer follow up (3-year OS 55.5% vs. 74.1% in patients <75 years).19 This raises concerns regarding feasibility in patients aged 75 years or over. Indeed, the rate of serious adverse events (SAE) was higher in patients aged 75 years or over (62 vs. 48%). The high discontinuation rate (34%) due to toxicity led to the initiation of trials exploring the safety and efficacy of once-weekly dosing instead of twice-weekly dosing of bortezomib. In the Spanish PETHEMA GEM05-trial, patients were treated with a once-weekly bortezomib scheme, either VMP or bortezomib-thalidomide-prednisone (VTP) followed by VP or VT maintenance therapy every three months. The incidence of severe peripheral neuropathy (PNP) decreased significantly from 14% in VISTA to 7%. Accordingly, the discontinuation rate due to SAE was lower as compared to the VISTA scheme: 17% vs. 34%. In the Italian GIMEMA MM03-05-trial, patients were treated with either nine cycles of MPV without maintenance or nine cycles of MPVT followed by continuous VT as maintenance strategy. Similar to the GEM05-trial, the incidence of grade 3/4 PNP and the discontinuation rate were low. Importantly, the decrease in dose density does not appear to negatively affect outcome in non-head-to-head comparisons with the VISTA trial. The PFS varied from 31–37 months versus 24 months for the VISTA trial. The median cumulative bortezomib dose delivered was similar in these trials,20,21 indicating that a lower dose in induction treatment reduces discontinuation rate allowing for longer treatment.
Meta analysis
A meta analysis of 1435 patients aged 65 years or over treated in 4 European clinical trials confirmed the independent negative impact of age 75 years or over on OS and provided evidence for negative impact of grade 3–4 non-hematologic toxicity (especially cardiac, infectious and gastrointestinal adverse events before 6 months) and discontinuation rate (before 6 months of therapy) on OS as well. The impact of age was most pronounced in the VMPT-treated patients (3.02-fold increase in risk) and the VMP-treated patients (1.62-fold increase in risk). There was no difference in impact of toxicity and discontinuation rate on OS between the treatment regimens.22 On the other hand, even more intense therapy including bortezomib-based induction therapy, followed by intermediate dose melphalan and autologous stem cell transplantation and lenalidomide maintenance was found to be feasible in fit elderly patients. But again, the death rate related to adverse effects was found to be significantly higher in the patients aged 70 years or over (5 of 26 vs. 3 of 76 patients).23 This highlights the need for tailored personalized medicine in these elderly patients.
Are there tools available to define the subpopulation of elderly multiple myeloma patients who will benefit from treatment?
Given the improvement in outcome that can be achieved by the use of IMiDs and PIs in the treatment of elderly patients with MM, even in patients not being treated in the RCT setting, there is an urgent need to identify those patients for whom therapy is feasible and in whom treatment will not only fail but might even compromise quality of life.
The Comprehensive Geriatric Assessment identifies general health status, including functional, cognitive, social, nutritional, and psychological parameters. It has not only been found to predict OS, but also adverse events during chemotherapy.24,25 However, it has two limitations. Firstly, data on the prospective value of CGA in patients with hematologic malignancies are limited, without specific data on MM patients. A recent systematic review of hematologic malignancies revealed 15 studies, showing that geriatric impairments could be detected even in patients with a normal performance status. Comorbidity, physical capacity and nutritional status were independently associated with OS. Only 2 studies investigated the association between geriatric assessments and chemotherapy-related toxicity. Moderate to severe comorbidity was a risk factor for non-hematologic toxicity in one study, whereas in the other study patients deemed to be unfit showed a 20% chemotherapy-related death rate compared with only 2% in fit patients.26 Secondly, the CGA is time consuming. Therefore, several studies investigated the possibility of shorter screening versions in order to identify fit patients who are able to receive standard of care with acceptable toxicity and vulnerable patients in whom extensive GA is needed to individualize therapy. A recent systematic review suggested that the discriminative power of frailty screening scores was not sufficient to select patients for further assessment.27 In contrast, Dupire et al. showed that the Prognostic Inflammatory and Nutritional Index, a relatively simple score incorporating blood markers reflecting inflammatory and nutritional status, was of prognostic value for outcome in elderly MM patients.28 In addition, Offidani et al. defined a vulnerability score (VS) based on the performance score (PS) and Charlson Cormorbidity Index (CCI) that was associated with an inferior median survival. However, treatment could have been a confounding factor in this non-uniformly-treated patient population.29 This methodological flaw was overcome in a recent presentation at ASH 2013 by Palumbo et al. showing that the frailty score, based on age (<75, 75–80, >80 years: score 0, 1, 2 respectively), CCI (≤1 or ≥2: score 0 or 1) and (instrumental) Activities Daily Life score (ADL >4 or ≤4: score 0 or 1; iADL>5 or ≤5: score 0 or 1), predicts non-hematologic toxicity in 869 patients aged 65 years or over uniformly treated within three randomized clinical trials. Frail patients (score ≥2) had a 1.8 times higher discontinuation rate compared to fit patients (score 0). No difference was found in hematologic toxicity. In a multivariate analysis, frailty (HR 1.64, 95%CI: 1.24–2.17), ISS 3 (HR 1.49, 95%CI: 1.17–1.89) and high-risk fluorescence in situ hybridization (FISH) (HR 1.75, 95%CI: 1.38–2.22) equally predicted PFS, whereas for OS the HR was highest for the frailty score: HR 3.11, 95%CI: 1.9–4.90 versus 1.77, 95%CI: 1.26–2.63 (ISS) and 1.83, 95%CI: 1.26–2.63 (high-risk FISH).30 Importantly, of the frail patients, 17% were aged under 75 years (44% of the unfit patients) so geriatric assessments were of value not only in those aged 75 years or over but also in those aged 65 years or over. These data underscore the importance of geriatric assessments as well as the need for prospective validation in uniformly treated patient populations. This will be performed in a Dutch HOVON study that will also implement objectively measured criteria (physical function such as gait speed and handgrip strength, cognitive function and sarcopenia) and explore the value of biomarkers reflecting biological age, such as the senescence marker p16INK4a.31 Hopefully, these biomarkers will be even more precise in predicting toxicity than calendar age.
How to treat elderly multiple myeloma patients in clinical practice?
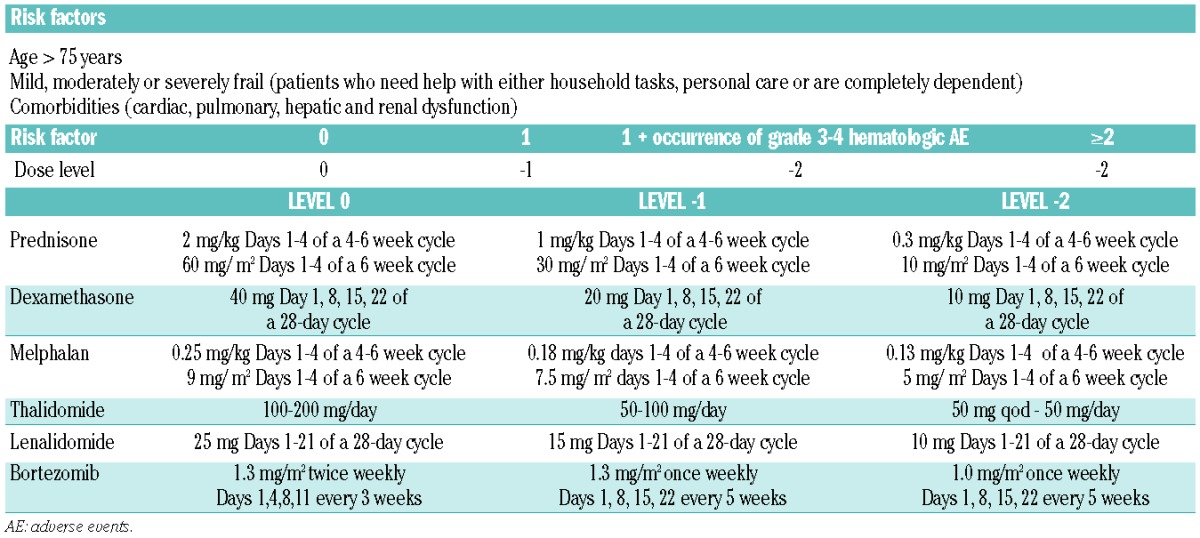
In conclusion, there is evidence that in patients aged 65 years or over, and especially in those aged 75 years or over, the toxicity of anti-myeloma treatment and subsequently the discontinuation rate is higher, negatively affecting outcome. On the other hand, the increasing number of treatment possibilities paves the way for improving the outcome also of the elderly MM patients. Given the first data on the predictive value of geriatric scores (fit – unfit – frail) determined by limited geriatric assessments, these should be implemented in clinical practice. Unfortunately, there are no studies prospectively investigating the clinical outcome in a randomized trial, either adapting the dose of anti-MM therapy according to these geriatric assessments or not. While awaiting the results of these clinical trials, practical guidelines were recently published that can be used to personalize therapy in those elderly patients currently being treated.1,3 In order to promote continuation of treatment by minimizing toxicity, we propose an algorithm that has been developed from these guidelines, and this is available in Table 1.
Table 1.
Algorithm developed from clinical trials practical guidelines.31
Footnotes
Financial and other disclosures provided by the author using the ICMJE (www.icmje.org) Uniform Format for Disclosure of Competing Interests are available with the full text of this paper at www.haematologica.org.
References
- 1.Palumbo A, Anderson K. Multiple myeloma. N Engl J Med. 2011;364(11):1046–60 [DOI] [PubMed] [Google Scholar]
- 2.Pozzi S, Marcheselli L, Bari A, Liardo EV, Marcheselli R, Luminari S, et al. Survival of multiple myeloma patients in the era of novel therapies confirms the improvement in patients younger than 75 years: a population-based analysis. Br J Haematol. 2013;163(1):40–6 [DOI] [PubMed] [Google Scholar]
- 3.Palumbo A, Bringhen S, Ludwig H, Dimopoulos MA, Blade J, Mateos MV, et al. Personalized therapy in multiple myeloma according to patient age and vulnerability: a report of the European Myeloma Network (EMN). Blood. 2011;118(17):4519–29 [DOI] [PubMed] [Google Scholar]
- 4.San Miguel JF, Schlag R, Khuageva NK, Dimopoulos MA, Shpilberg O, Kropff M, et al. Persistent overall survival benefit and no increased risk of second malignancies with bortezomib-melphalan-prednisone versus melphalan-prednisone in patients with previously untreated multiple myeloma. J Clin Oncol. 2013;31(4):448–55 [DOI] [PubMed] [Google Scholar]
- 5.Fayers PM, Palumbo A, Hulin C, Waage A, Wijermans P, Beksac M, et al. Thalidomide for previously untreated elderly patients with multiple myeloma: meta-analysis of 1685 individual patient data from 6 randomized clinical trials. Blood. 2011;118(5):1239–47 [DOI] [PubMed] [Google Scholar]
- 6.Palumbo A, Hajek R, Delforge M, Kropff M, Petrucci MT, Catalano J, et al. Continuous lenalidomide treatment for newly diagnosed multiple myeloma. N Engl J Med. 2012;366(19):1759–69 [DOI] [PubMed] [Google Scholar]
- 7.Nilsson T, Hoglund M, Lenhoff S, Rylander L, Turesson I, Westin J, et al. A pooled analysis of karyotypic patterns, breakpoints and imbalances in 783 cytogenetically abnormal multiple myelomas reveals frequently involved chromosome segments as well as significant age-and sex-related differences. Br J Haematol. 2003;120(6):960–9 [DOI] [PubMed] [Google Scholar]
- 8.Avet-Loiseau H, Hulin C, Campion L, Rodon P, Marit G, Attal M, et al. Chromosomal abnormalities are major prognostic factors in elderly patients with multiple myeloma: the intergroupe francophone du myelome experience. J Clin Oncol. 2013;31(22):2806–9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kaiser MF, Johnson DC, Wu P, Walker BA, Brioli A, Mirabella F, et al. Global methylation analysis identifies prognostically important epigenetically inactivated tumor suppressor genes in multiple myeloma. Blood. 2013;122(2):219–26 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Schaapveld M, Visser O, Siesling S, Schaar CG, Zweegman S, Vellenga E. Improved survival among younger but not among older patients with Multiple Myeloma in the Netherlands, a population-based study since 1989. Eur J Cancer. 2010;46(1):160–9 [DOI] [PubMed] [Google Scholar]
- 11.Kumar SK, Dispenzieri A, Lacy MQ, Gertz MA, Buadi FK, Pandey S, et al. Continued improvement in survival in multiple myeloma: changes in early mortality and outcomes in older patients. Leukemia. 2013. October 25 [Epub ahead of print] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Liwing J, Uttervall K, Lund J, Aldrin A, Blimark C, Carlson K, et al. Improved survival in myeloma patients: starting to close in on the gap between elderly patients and a matched normal population. Br J Haematol. 2014;164(5):684–93 [DOI] [PubMed] [Google Scholar]
- 13.Hulin C, Rodon P, Campion L, Roussel M, Leleu X, Marit G, et al. Clinical Characteristics, Chromosomal Abnormalities and Outcomes in Very Elderly Patients with Multiple Myeloma: The IFM Experience. ASH Annual Meeting Abstracts 2012 [Google Scholar]
- 14.Falco P, Cavallo F, Larocca A, Rossi D, Guglielmelli T, Rocci A, et al. Lenalidomide-prednisone induction followed by lenalidomide-melphalan-prednisone consolidation and lenalidomide-prednisone maintenance in newly diagnosed elderly unfit myeloma patients. Leukemia. 2013;27(3):695–701 [DOI] [PubMed] [Google Scholar]
- 15.Hulin C, Facon T, Rodon P, Pegourie B, Benboubker L, Doyen C, et al. Efficacy of melphalan and prednisone plus thalidomide in patients older than 75 years with newly diagnosed multiple myeloma: IFM 01/01 trial. J Clin Oncol. 2009;27(22):3664–70 [DOI] [PubMed] [Google Scholar]
- 16.Palumbo A, Waage A, Hulin C, Beksac M, Zweegman S, Gay F, et al. Safety of thalidomide in newly diagnosed elderly myeloma patients: a meta-analysis of data from individual patients in six randomized trials. Haematologica. 2013;98(1):87–94 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.San MJ, Weisel K, Moreau P, Lacy M, Song K, Delforge M, et al. Pomalidomide plus low-dose dexamethasone versus high-dose dexamethasone alone for patients with relapsed and refractory multiple myeloma (MM-003): a randomised, open-label, phase 3 trial. Lancet Oncol. 2013;14(11):1055–66 [DOI] [PubMed] [Google Scholar]
- 18.Weisel K, San Miguel J, Wong KW, Delforge M, Karlin L, Goldschmidt H, et al. MM-003 Phase 3 Study Of Pomalidomide In Combination With Low-Dose Dexamethasone (POM + LoDEX) Vs High-Dose Dexamethasone (HiDEX) In Relapsed/Refractory Multiple Myeloma (RRMM): POM + Lodex Is Beneficial For Elderly Patients (> 65 Years of Age). ASH Annual Meeting Abstracts 2013 [Google Scholar]
- 19.Mateos MV, Richardson PG, Schlag R, Khuageva NK, Dimopoulos MA, Shpilberg O, et al. Bortezomib plus melphalan and prednisone compared with melphalan and prednisone in previously untreated multiple myeloma: updated follow-up and impact of subsequent therapy in the phase III VISTA trial. J Clin Oncol. 2010;28(13):2259–66 [DOI] [PubMed] [Google Scholar]
- 20.Mateos MV, Oriol A, Martinez-Lopez J, Gutierrez N, Teruel AI, de PR, et al. Bortezomib, melphalan, and prednisone versus bortezomib, thalidomide, and prednisone as induction therapy followed by maintenance treatment with bortezomib and thalidomide versus bortezomib and prednisone in elderly patients with untreated multiple myeloma: a randomised trial. Lancet Oncol. 2010;11(10):934–41 [DOI] [PubMed] [Google Scholar]
- 21.Palumbo A, Bringhen S, Larocca A, Rossi D, Di Raimondo F, Magarotto V, et al. Bortezomib-melphalan-prednisone-thalidomide followed by maintenance with bortezomib-thalidomide compared with bortezomib-melphalan-prednisone for initial treatment of multiple myeloma: updated follow-up and improved survival. J Clin Oncol. 2014;32(7):634–40 [DOI] [PubMed] [Google Scholar]
- 22.Bringhen S, Mateos MV, Zweegman S, Larocca A, Falcone AP, Oriol A, et al. Age and organ damage correlate with poor survival in myeloma patients: meta-analysis of 1435 individual patient data from 4 randomized trials. Haematologica. 2013;98(6):980–7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Gay F, Magarotto V, Crippa C, Pescosta N, Guglielmelli T, Cavallo F, et al. Bortezomib induction, reduced-intensity transplantation, and lenalidomide consolidation-maintenance for myeloma: updated results. Blood. 2013;122(8):1376–83 [DOI] [PubMed] [Google Scholar]
- 24.Kenis C, Decoster L, Van PK, De Grève J, Conings G, Milisen K, et al. Performance of two geriatric screening tools in older patients with cancer. J Clin Oncol. 2014;32(1):19–26 [DOI] [PubMed] [Google Scholar]
- 25.Hurria A, Togawa K, Mohile SG, Owusu C, Klepin HD, Gross CP, et al. Predicting chemotherapy toxicity in older adults with cancer: a prospective multicenter study. J Clin Oncol. 2011;29(25):3457–65 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Hamaker ME, Prins MC, Stauder R. The relevance of a geriatric assessment for elderly patients with a haematological malignancy - A systematic review. Leuk Res. 2014;38(3):275–83 [DOI] [PubMed] [Google Scholar]
- 27.Hamaker ME, Jonker JM, de Rooij SE, Vos AG, Smorenburg CH, van Munster BC. Frailty screening methods for predicting outcome of a comprehensive geriatric assessment in elderly patients with cancer: a systematic review. Lancet Oncol. 2012;13(10):e437–e444 [DOI] [PubMed] [Google Scholar]
- 28.Dupire S, Wemeau M, Debarri H, Pascal L, Hivert B, Willekens C, et al. Prognostic value of PINI index in patients with multiple myeloma. Eur J Haematol. 2012;88(4):306–13 [DOI] [PubMed] [Google Scholar]
- 29.Offidani M, Corvatta L, Polloni C, Centurioni R, Visani G, Brunori M, et al. Assessment of vulnerability measures and their effect on survival in a real-life population of multiple myeloma patients registered at Marche Region Multiple Myeloma Registry. Clin Lymphoma Myeloma Leuk. 2012;12(6):423–32 [DOI] [PubMed] [Google Scholar]
- 30.Larocca A, Bringhen S, Evangelista A, Offidani M, Ballanti S, Zaccaria A, et al. A Simple Score, Based On Geriatric Assessment, Improves Prediction of Survival, and Risk Of Serious Adverse Events In Elderly Newly Diagnosed Multiple Myeloma Patients. ASH Annual Meeting Abstracts 2013 [Google Scholar]
- 31.Waaijer ME, Parish WE, Strongitharm BH, van Heemst D, Slagboom PE, de Craen AJ, et al. The number of p16INK4a positive cells in human skin reflects biological age. Aging Cell. 2012;11(4):722–5 [DOI] [PMC free article] [PubMed] [Google Scholar]