

Abstract
In a randomized, phase III trial of nilotinib versus imatinib in patients with newly diagnosed Philadelphia chromosome positive chronic myeloid leukemia in chronic phase, more patients had suboptimal response or treatment failure on front-line imatinib than on nilotinib. Patients with suboptimal response/treatment failure on imatinib 400 mg once or twice daily or nilotinib 300 mg twice daily could enter an extension study to receive nilotinib 400 mg twice daily. After a 19-month median follow up, the safety profile of nilotinib 400 mg twice daily in patients switching from imatinib (n=35) was consistent with previous reports, and few new adverse events occurred in patients escalating from nilotinib 300 mg twice daily (n=19). Of patients previously treated with imatinib or nilotinib 300 mg twice daily, respectively, 15 of 26 (58%) and 2 of 6 (33%) without complete cytogenetic response at extension study entry, and 11 of 34 (32%) and 7 of 18 (39%) without major molecular response at extension study entry, achieved these responses at any time on nilotinib 400 mg twice daily. Estimated 18-month rates of freedom from progression and overall survival after entering the extension study were lower for patients switched from imatinib (85% and 87%, respectively) versus nilotinib 300 mg twice daily (95% and 94%, respectively). Nilotinib dose escalation was generally well tolerated and improved responses in about one-third of patients with suboptimal response/treatment failure. Switch to nilotinib improved responses in some patients with suboptimal response/treatment failure on imatinib, but many did not achieve complete cytogenetic response (clinicaltrials.gov identifiers:00718263, 00471497 - extension).
Introduction
Nilotinib is a more potent and selective inhibitor of BCR-ABL than imatinib.1 Results of the Evaluating Nilotinib Efficacy and Safety in Clinical Trials-Newly Diagnosed Patients (ENESTnd) phase III trial demonstrated the superior efficacy of nilotinib compared with imatinib. After 1, 2 and 3 years of follow up, patients treated with nilotinib 300 mg twice daily or nilotinib 400 mg twice daily had significantly lower rates of progression to accelerated phase/blast crisis (AP/BC) and fewer deaths, as well as significantly higher molecular and cytogenetic response rates, compared with patients receiving imatinib.2–4 Nilotinib is approved for the treatment of patients with newly diagnosed Philadelphia chromosome positive (Ph+) chronic myeloid leukemia in chronic phase (CML-CP) and for the treatment of imatinib-resistant or -intolerant adult patients with Ph+ CML in CP or AP.5,6
Despite the positive impact of tyrosine kinase inhibitors (TKIs) such as nilotinib and imatinib on the treatment of CML, some patients do not achieve optimal responses to TKI therapy. Patients who experience treatment failure on TKI therapy are unlikely to achieve long-term disease control and are at high risk of disease progression; patients with suboptimal responses to TKI therapy have a reduced likelihood of achieving future optimal responses and outcomes compared with patients who achieve optimal responses to therapy.7–9 Thus, careful management of patients with CML-CP who have non-optimal responses to front-line TKI therapy is necessary.
For patients who experience treatment failure on TKI therapy, the European LeukemiaNet recommends switching to a different therapy “whenever available and applicable”.8 However, for patients with suboptimal responses, who may continue to derive benefit from their current treatment, the decision for clinicians is less clear.10 Several studies have shown that imatinib dose escalation may provide additional benefit in some patients with suboptimal responses/treatment failure on standard-dose imatinib;11–13 however, high-dose imatinib is associated with an increased risk of adverse events (AEs), particularly grade 3/4 hematologic toxicity.14,15 The safety and efficacy of nilotinib in patients with imatinib-resistant or -intolerant CML are well established.16–20 However, prospective clinical data evaluating the benefits of switching patients with suboptimal response on front-line imatinib to nilotinib are limited.19,21 Furthermore, the impact of nilotinib dose escalation in patients with suboptimal responses/treatment failure on frontline nilotinib has yet to be explored.
An extension study to ENESTnd was designed to provide patients who experienced suboptimal responses or treatment failure on front-line imatinib or nilotinib in the core study the opportunity to receive other treatment options. This report describes the frequency of suboptimal responses/treatment failure in newly diagnosed CML-CP patients treated with imatinib, nilotinib 300 mg twice daily, or nilotinib 400 mg twice daily in the ENESTnd core study. It also presents the first results of the ENESTnd extension study, including the safety and efficacy of nilotinib 400 mg twice daily in patients with suboptimal responses/treatment failure on front-line imatinib or nilotinib 300 mg twice daily, with a median follow up of 19 months.
Methods
ENESTnd core study
The design of ENESTnd has been previously reported2–4 and is described in the Online Supplementary Appendix. Patients with suboptimal response or treatment failure in the core study were eligible for the extension study. Definitions of suboptimal response and treatment failure were based on those in the 2009 European LeukemiaNet recommendations8 and are described in the Online Supplementary Methods. Patients who were intolerant of imatinib or nilotinib in the core study were ineligible for the extension study.
ENESTnd extension study: patients, study design and treatments
Patients with suboptimal response or treatment failure on imatinib (400 mg once or twice daily) or nilotinib 300 mg twice daily in the core study received nilotinib 400 mg twice daily in the extension study. Patients with treatment failure on nilotinib 400 mg twice daily in the core study received imatinib 400 mg twice daily in the extension study. Dose reductions of nilotinib or imatinib were allowed for patients who experienced treatment-related toxicity. Patients could be withdrawn from the extension study for the following reasons: death, intolerable toxicity, disease progression, or patient’s or investigator’s decision. Survival information and progression events in patients who discontinued were collected every three months (1 month=28 days) for up to ten years.
End points
The primary objective of the extension study was to characterize the safety and tolerability of nilotinib 400 mg twice daily after insufficient response to imatinib or nilotinib 300 mg twice daily in the core study. The secondary objective was to evaluate the efficacy of nilotinib 400 mg twice daily after insufficient response to imatinib or nilotinib 300 mg twice daily. Molecular response was assessed in all patients by real-time quantitative reverse transcriptase polymerase chain reaction (RQ-PCR) every month for the first three months and every three months thereafter in a central laboratory (MolecularMD, Portland, OR, USA). Other study definitions and assessments were as defined previously for the ENESTnd core study.2–4
Statistical analysis
Incidence of suboptimal response and treatment failure in the ENESTnd core study was analyzed descriptively by treatment arm. Safety and efficacy data from the ENESTnd extension study were analyzed descriptively according to original core study treatment arm. Rates of complete cytogenetic response (CCyR) and major molecular response (MMR) at any time during the extension study (from time of entry to time of data cut off) and rates of MMR by 12 months were determined according to response at time of extension study entry. Time-to-event outcomes were analyzed using the Kaplan-Meier method.
The cut-off date for all analyses was July 27, 2011 (the same cutoff date as for the 3-year analysis of the ENESTnd core study4). The ENESTnd core and extension studies are being conducted according to the ethical principles of the Declaration of Helsinki, and written informed consent was obtained from each patient. The study protocols and amendments were approved by the institutional review board, independent ethics committee, or research ethics board at each center. These studies are registered at www.clinicaltrials.gov (clinicaltrials.gov identifiers:00718263, 00471497 - extension).
Results
ENESTnd core study: incidence of suboptimal response/treatment failure
The ENESTnd core study enrolled 846 patients with newly diagnosed CML-CP, randomized to nilotinib 300 mg twice daily (n=282), nilotinib 400 mg twice daily (n=281), or imatinib 400 mg once daily (n=283). The incidence of suboptimal response by 6, 12 and 18 months was lower in each nilotinib arm than in the imatinib arm (Figure 1A). By 6 months, 6 (2%), 7 (2%), and 18 (6%) patients in the nilotinib 300 mg twice-daily, nilotinib 400 mg twice-daily, and imatinib arms, respectively, had suboptimal response. By 12 months, 11 (4%), 12 (4%), and 38 (13%) patients in the nilotinib 300 mg twice-daily, nilotinib 400 mg twice-daily, and imatinib arms, respectively, had suboptimal response. The incidence of suboptimal response by 18 months (when a lack of MMR first became a criterion for suboptimal response) was higher across all 3 treatment arms, and the difference between the nilotinib arms and the imatinib arm persisted, with suboptimal response in 68 (24%), 84 (30%), and 128 (45%) patients in the nilotinib 300 mg twice-daily, nilotinib 400 mg twice-daily, and imatinib arms, respectively. Similarly, fewer nilotinib-treated patients than imatinib-treated patients had treatment failure by 6, 12, and 18 months (Figure 1B).
Figure 1.
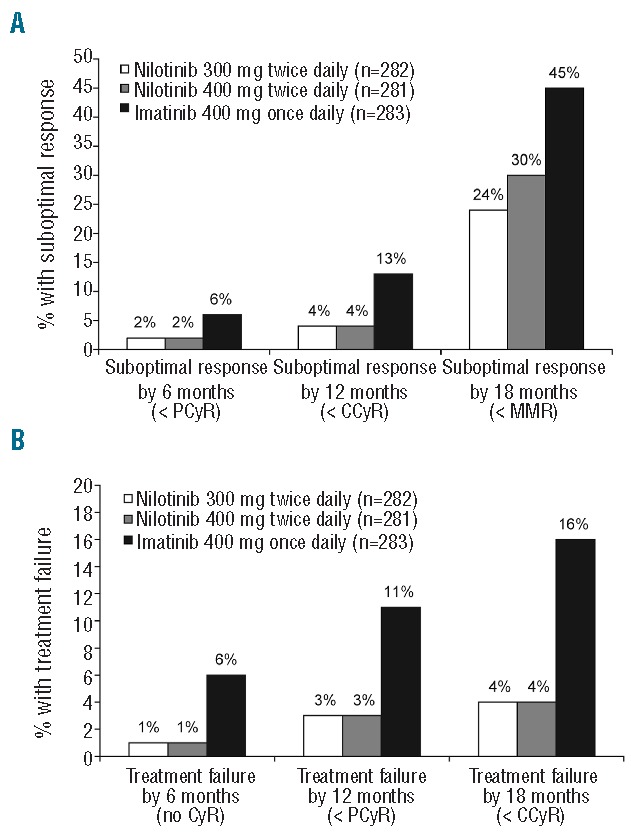
Cumulative incidence of suboptimal response (A) and treatment failure (B) in the ENESTnd core study by 6, 12, and 18 months. Key criteria for suboptimal response/treatment failure at 6, 12, and 18 months are shown in parentheses on the x-axis. Suboptimal response also included loss of major molecular response (MMR) at any time. Treatment failure also included loss of complete hematologic response (CHR), loss of partial cytogenetic response/complete cytogenetic response (PCyR/CCyR), or progression to accelerated phase/blast crisis at any time. Patients satisfying criteria for both suboptimal response and treatment failure were considered to have treatment failure. Only a patient’s worst response at or before each time point was counted.
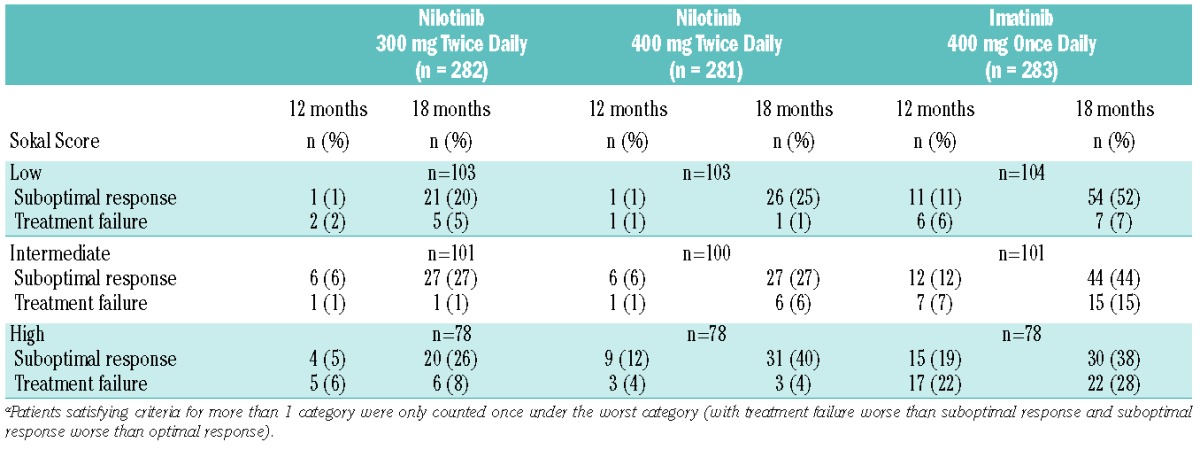
When responses were evaluated in patients stratified by Sokal risk score, rates of suboptimal response and treatment failure were generally lower in nilotinib-treated patients than in imatinib-treated patients, regardless of Sokal risk (Table 1). The differences in rates of treatment failure between the nilotinib arms and the imatinib arm were greatest in high Sokal risk patients; rates of treatment failure by 12 and 18 months were 6% and 8%, 4% and 4%, and 22% and 28% in the nilotinib 300 mg twice-daily, nilotinib 400 mg twice-daily, and imatinib arms, respectively.
Table 1.
Cumulative incidence of suboptimal response and treatment failure by 12 and 18 months in the ENESTnd Core Study stratified by Sokal Risk Scorea.
Patients with suboptimal response or treatment failure on imatinib 400 mg once daily were permitted to dose escalate to imatinib 400 mg twice daily. However, as has been previously reported,22 over half of these patients did not achieve improved responses following imatinib dose escalation, and many required subsequent dose reductions or interruptions.
ENESTnd extension study: patients, treatments, and disposition
In the ENESTnd core study, 57 patients discontinued from the imatinib arm due to suboptimal response or treatment failure; 35 of these patients entered the extension study to receive nilotinib 400 mg twice daily (Table 2). Many of these patients (24 of 35; 69%) had dose-escalated to imatinib 400 mg twice daily while on the core study. The majority of patients entering the extension study from the imatinib arm had treatment failure in the core study (60%; 21 of 35), 34% (12 of 35) had suboptimal response, and 6% (2 of 35) entered the extension study based on the investigator’s assessment without meeting the criteria for suboptimal response/treatment failure. In the nilotinib 300 mg twice-daily arm of the core study, 28 patients discontinued due to suboptimal response or treatment failure, and 19 of these patients entered the extension study to receive nilotinib 400 mg twice daily. The majority of patients entering the extension study from the nilotinib 300 mg twice daily arm had suboptimal response in the core study (79%; 15 of 19), 16% (3 of 19) had treatment failure, and 5% (1 patient) entered the extension study based on the investigator’s assessment without meeting the criteria for suboptimal response/treatment failure.
Table 2.
ENESTnd Core Study: reasons for entry into the ENESTnd Extension Studya.

With a median follow up of 19 months in the extension study, 63% (22 of 35) of patients previously treated with imatinib and 74% (14 of 19) of patients previously treated with nilotinib 300 mg twice daily remained on extension treatment with nilotinib 400 mg twice daily at the time of data cut off. In patients previously treated with imatinib, the median time on extension treatment was 15.5 months (range 0.2–35.2 months), and the median dose intensity was 799 mg/day (range 421–800 mg/day); 17 patients (49%) experienced a dose reduction or interruption because of an AE or laboratory abnormality. Of patients previously treated with imatinib, 13 discontinued extension treatment for the following reasons: unsatisfactory therapeutic effect (n=5), AEs or laboratory abnormalities (n=4), disease progression (n=2), death (n=1), and protocol deviation (n=1). In patients previously treated with nilotinib 300 mg twice daily, the median time on extension treatment was 18.0 months (range 1.0–25.5 months), and the median dose intensity was 800 mg/day (range 605–800 mg/day); 4 patients (21%) experienced a dose reduction or interruption because of an AE or laboratory abnormality. Of patients previously treated with nilotinib 300 mg twice daily, 5 discontinued extension treatment (4 due to unsatisfactory therapeutic effect and 1 due to protocol deviation).
A total of 11 patients in the core study discontinued nilotinib 400 mg twice daily due to treatment failure, and 3 of these patients entered the extension study to receive imatinib 400 mg twice daily. Given the limited number of patients receiving imatinib 400 mg twice daily in the extension study, analysis of imatinib safety and efficacy in these patients was not performed.
Safety of nilotinib 400 mg twice daily in the extension study
In patients previously treated with imatinib, the safety profile of nilotinib 400 mg twice daily was consistent with that in previous reports of patients who switched from imatinib to nilotinib.16,19,20 Nineteen patients (54%) experienced grade 3/4 AEs, and 4 patients (11%) discontinued treatment because of AEs. The most common non-hematologic AEs of any grade were rash (29%), headache (23%), and dyspnea (17%) (Table 3). Grade 3/4 non-hematologic AEs were uncommon. Grade 3/4 anemia (9%), neutropenia (9%), and thrombocytopenia (6%) occurred infrequently. The most common (occurring in at least 2 patients) grade 3/4 biochemical abnormalities were hyperbilirubinemia in 3 patients (9%), hyperglycemia in 2 patients (6%), and decreased phosphorus in 2 patients (6%). In patients previously treated with nilotinib 300 mg twice daily, there were minimal changes in safety from those reported with nilotinib 300 mg twice daily in the ENESTnd core study.2–4 Six patients (32%) had grade 3/4 AEs, and no patient discontinued because of AEs or laboratory abnormalities. There were no grade 3/4 myelosuppression events and few newly occurring or worsening grade 3/4 biochemical abnormalities (Table 3).
Table 3.
Most frequently reported (≥ 10%) adverse events and newly occurring or worsening hematologic and biochemical abnormalities in patients treated with nilotinib 400 mg twice daily in the ENESTnd Extension Study by previous therapy, regardless of relationship to study druga.

Efficacy of nilotinib 400 mg twice daily in the extension study
Many patients with suboptimal response/treatment failure on front-line imatinib achieved improved cytogenetic and molecular responses after switching to nilotinib 400 mg twice daily. Analysis of CCyR and MMR rates in patients previously treated with imatinib excluded 9 and one patients, respectively, who had these responses at extension study entry. Of the 26 patients previously treated with imatinib who did not have CCyR at extension study entry, 15 (58%) achieved CCyR at any time (from date of extension study entry to data cut-off date; median follow up 19 months) on nilotinib 400 mg twice daily (Figure 2A). Of the 34 patients previously treated with imatinib who did not have MMR at extension study entry, 11 (32%) achieved MMR at any time on nilotinib 400 mg twice daily. These same 11 patients all achieved MMR by 12 months, so the rate of MMR by 12 months was also 32%. Two of 8 patients (25%) without MMR but with CCyR at extension study entry achieved MMR by 12 months.
Figure 2.
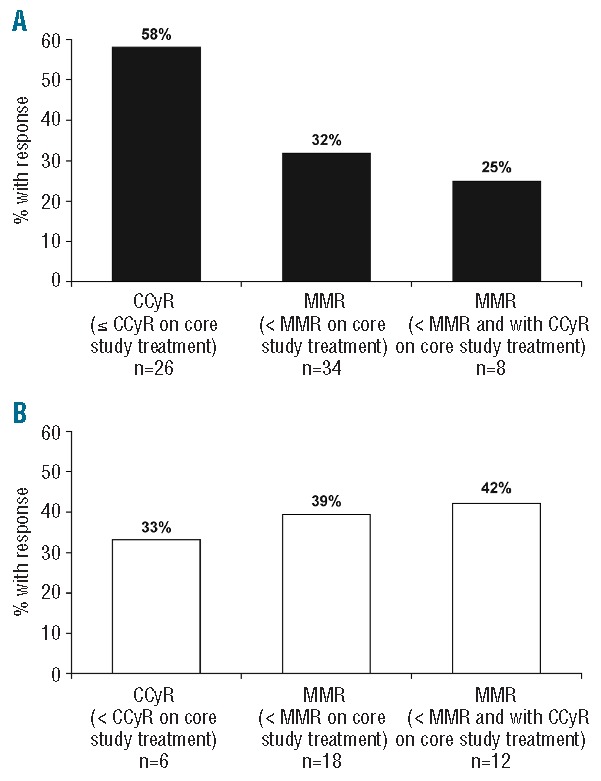
Cumulative incidence of complete cytogenetic response (CCyR) and major molecular response (MMR) on extension study treatment (nilotinib 400 mg twice daily) in patients previously treated with (A) imatinib or (B) nilotinib 300 mg twice daily. Shown from left to right are rates of CCyR at any time (from date of extension study entry to data cut-off date; median follow up of 19 months) in patients without CCyR at extension study entry, rates of MMR at any time and by 12 months in patients without MMR at extension study entry, and rates of MMR by 12 months in patients without MMR but with CCyR at extension study entry.
Analysis of CCyR and MMR rates in patients previously treated with nilotinib 300 mg BID excluded 13 and one patients, respectively, who had these responses at extension study entry. In patients previously treated with nilotinib 300 mg twice daily, 2 of 6 patients (33%) without CCyR at extension study entry achieved CCyR at any time on nilotinib 400 mg twice daily, and 7 of 18 patients (39%) without MMR at extension study entry achieved MMR at any time (Figure 2B). These same 7 patients all achieved MMR by 12 months, so the rate of MMR by 12 months was also 39%. Five of 12 patients (42%) without MMR but with CCyR at extension study entry achieved MMR by 12 months.
Molecular responses were achieved in the extension study in patients of all Sokal risk groups (Table 4). Among patients previously treated with imatinib without MMR at extension study entry, 4 of 8 (50%) low Sokal risk patients, 4 of 9 (44%) intermediate-risk patients, and 3 of 17 (18%) high-risk patients achieved MMR or better at any time on nilotinib 400 mg twice daily. Of the 11 patients with high Sokal risk and treatment failure on previous imatinib, 2 (18%) had a molecular response on extension treatment (1 achieved MR4, 1 achieved MR45). Among patients previously treated with nilotinib 300 mg twice daily without MMR at extension study entry, one of 4 (25%) low Sokal risk patients, 4 of 6 (67%) intermediate-risk patients, and 2 of 8 (25%) high-risk patients achieved MMR or better at any time on nilotinib 400 mg twice daily.
Table 4.
Best molecular response on nilotinib 400 mg twice daily extension treatment at any timea according to Sokal risk and reason for discontinuation of core treatment in patients without MMR at extension study entry.

The estimated rates of freedom from progression to AP/BC at 18 months from start of extension treatment were 85% (95%CI: 71–99%) and 95% (95%CI: 85–100%) in patients previously treated with imatinib and with nilotinib 300 mg twice daily, respectively. In total, 5 patients previously treated with imatinib who switched to nilotinib on the extension study progressed to AP/BC: 2 progressed during extension treatment and 3 progressed after discontinuation of extension treatment. Additionally, one patient previously treated with nilotinib 300 mg twice daily progressed to AP/BC after discontinuation of the extension treatment. All progression events reported here were also included in the overall reported progression events from the ENESTnd core study with three years of follow up.4
The estimated rates of overall survival at 18 months from the start of extension treatment were 87% (95%CI, 75–99%) and 94% (95%CI, 83%–100%) in patients previously treated with imatinib and with nilotinib 300 mg twice daily, respectively. Seven patients previously treated with imatinib died on the extension study: 5 from CML-related causes at 2, 246, 286, 326, and 593 days after treatment discontinuation, 1 from chronic renal failure 91 days after treatment discontinuation, and 1 from pneumonia 788 days after treatment discontinuation. One patient previously treated with nilotinib 300 mg twice daily died 305 days after treatment discontinuation due to CML-related complications. All deaths reported here were also included in the overall deaths reported in the ENESTnd core study with 3 years of follow up.4
Discussion
In the ENESTnd core study, rates of suboptimal response and treatment failure by 6, 12, and 18 months were lower in patients treated with front-line nilotinib than in patients treated with front-line imatinib. Strikingly, the rate of treatment failure by 18 months was nearly 4 times higher in the imatinib arm than in the nilotinib arms. This difference was most pronounced among high Sokal risk patients, who had a high rate of treatment failure on imatinib but who fared similarly to patients with low or intermediate Sokal risk when treated with nilotinib. This may be because the increased potency and selectivity of nilotinib can more effectively compensate for unfavorable host factors than imatinib. These results are consistent with previously reported efficacy data demonstrating numerically higher rates of CCyR, MMR, and deep molecular response (i.e. MR4 (BCR-ABLIS ≤ 0.01%) and MR4.5 (BCR-ABLIS ≤ 0.0032%)23 with nilotinib versus imatinib in all Sokal risk groups.3,4
Results from the ENESTnd extension study demonstrate that many patients with suboptimal response or treatment failure on imatinib may benefit from switching to nilotinib. More than half of patients who did not achieve CCyR on imatinib core treatment achieved this response on nilotinib 400 mg twice daily, and over 30% of patients who did not achieve MMR on imatinib core treatment achieved this response with nilotinib 400 mg twice daily. Safety and efficacy results observed in this study were consistent with those in previous reports of second-line nilotinib treatment in patients with imatinib-resistant or -intolerant CML-CP.16,19,20
Rates of suboptimal response and treatment failure with front-line nilotinib 300 mg twice daily and nilotinib 400 mg twice daily in the ENESTnd core study were similar, yet for patients with suboptimal response or treatment failure on nilotinib 300 mg twice daily, dose escalation to nilotinib 400 mg twice daily provided additional efficacy benefit in approximately one-third of patients (33% of patients who did not achieve CCyR on nilotinib 300 mg twice daily core treatment achieved this response on nilotinib 400 mg twice daily, and 39% of patients who did not achieve MMR on nilotinib 300 mg twice daily core treatment achieved this response on nilotinib 400 mg twice daily). Dose escalation of nilotinib was safe, with few new AEs observed, and may represent a viable treatment strategy in patients with suboptimal response or treatment failure on front-line nilotinib 300 mg twice daily. However, it remains unknown whether dose escalation of nilotinib in such patients is preferable to alternate therapies, including other TKIs and stem cell transplantation.
Responses of MMR or better were observed on nilotinib 400 mg twice daily both in patients with suboptimal response and in patients with treatment failure on front-line imatinib across all Sokal risk groups (including 2 patients with treatment failure on imatinib who went on to achieve deep molecular responses on nilotinib 400 mg twice daily), suggesting that a switch to nilotinib 400 mg twice daily is a reasonable strategy in patients of any Sokal risk category. However, this switch in therapy is not effective in all patients. Many patients with suboptimal response/treatment failure on previous imatinib in our study did not achieve improved responses on extension treatment; such patients may be candidates for treatment with an alternate TKI or stem cell transplantation.
Notably, although all patients in the extension study received the same treatment of nilotinib 400 mg twice daily, the estimated 18-month rates of freedom from progression and overall survival were lower for patients switched from imatinib (85% and 87%, respectively) than for those initially treated with nilotinib 300 mg twice daily (95% and 94%, respectively). In addition, opposing trends in response rates between the two groups were observed, with higher rates of CCyR achievement on nilotinib 400 mg twice daily in patients previously treated with imatinib, and higher rates of MMR achievement in patients previously treated with nilotinib 300 mg twice daily (Figure 2). These differences in outcomes could be related to the higher proportion of patients in this study who switched from imatinib due to treatment failure versus suboptimal response; in contrast, most patients from the nilotinib 300 mg twice-daily arm entered the extension study due to suboptimal response. Very few patients entered the extension study having not achieved a CCyR on nilotinib 300 mg twice daily, and the relatively low rate of CCyR achievement in these patients on nilotinib dose escalation may be an indication of more aggressive disease biology. Nonetheless, the increased risk of disease progression or death in patients with suboptimal response/treatment failure on front-line imatinib, despite a subsequent switch to nilotinib, highlights the importance of optimal front-line therapy selection, in order to achieve and sustain the best possible responses early in a patient’s treatment course.
Acknowledgments
We thank Karen Miller-Moslin, PhD and Karen Kaluza, PhD (of Articulate Science) for medical editorial assistance with this manuscript. Financial support for medical editorial assistance was provided by Novartis Pharmaceuticals Corporation.
Footnotes
The online version of this article has a Supplementary Appendix
Funding
TPH received consultation fees and research funding from Novartis, BMS, and Ariad. AH received consultation fees and research funding from Novartis, BMS, Pfizer, and Ariad. HMK acted as a consultant for Novartis and received research funding from BMS, Novartis, Ariad, and Pfizer. FC received lecture fees from Novartis. FG received lecture fees and research funding from Novartis. DN received consultation fees from Novartis and lecture fees from Novartis, BMS, and Gentium. PDlC received consultation fees from Novartis, lecture fees from Novartis and BMS, and research funding from Novartis. GR received consultation fees for Novartis, BMS, and Roche and received research funding from Novartis. GO acted as a consultant and received honoraria from Novartis and BMS, and received research funding from Novartis. CL has nothing to disclose. HS received lecture fees from Novartis. XF, HDM, and CK are Novartis employees. RAL acted as a consultant and received research funding from Novartis. GS acted as a consultant for Novartis and BMS and received lecture fees from Novartis, BMS, Pfizer, and Ariad.
Authorship and Disclosures
Information on authorship, contributions, and financial & other disclosures was provided by the authors and is available with the online version of this article at www.haematologica.org.
References
- 1.Weisberg E, Manley PW, Breitenstein W, Bruggen J, Cowan-Jacob SW, Ray A, et al. Characterization of AMN107, a selective inhibitor of native and mutant bcr-abl. Cancer Cell. 2005;7(2):129–41 [DOI] [PubMed] [Google Scholar]
- 2.Saglio G, Kim DW, Issaragrisil S, le Coutre P, Etienne G, Lobo C, et al. Nilotinib versus imatinib for newly diagnosed chronic myeloid leukemia. N Engl J Med. 2010;362(24):2251–9 [DOI] [PubMed] [Google Scholar]
- 3.Kantarjian HM, Hochhaus A, Saglio G, De Souza C, Flinn IW, Stenke L, et al. Nilotinib versus imatinib for the treatment of patients with newly diagnosed chronic phase, philadelphia chromosome-positive, chronic myeloid leukaemia: 24-month minimum follow-up of the phase 3 randomised ENESTnd trial. Lancet Oncol. 2011;12(9):841–51 [DOI] [PubMed] [Google Scholar]
- 4.Larson RA, Hochhaus A, Hughes TP, Clark RE, Etienne G, Kim DW, et al. Nilotinib vs imatinib in patients with newly diagnosed philadelphia chromosome-positive chronic myeloid leukemia in chronic phase: ENESTnd 3-year follow-up. Leukemia. 2012;26(10):2197–203 [DOI] [PubMed] [Google Scholar]
- 5.Novartis Pharmaceuticals Corporation. Tasigna prescribing information. 2012 [Google Scholar]
- 6.Novartis Europharm Limited. Tasigna summary of product characteristics. 2012 [Google Scholar]
- 7.Marin D, Milojkovic D, Olavarria E, Khorashad JS, de Lavallade H, Reid AG, et al. European LeukemiaNet criteria for failure or suboptimal response reliably identify patients with CML in early chronic phase treated with imatinib whose eventual outcome is poor. Blood. 2008;112(12):4437–44 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Baccarani M, Cortes J, Pane F, Niederwieser D, Saglio G, Apperley J, et al. Chronic myeloid leukemia: an update of concepts and management recommendations of European LeukemiaNet. J Clin Oncol. 2009;27(35):6041–51 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Alvarado Y, Kantarjian H, O’Brien S, Faderl S, Borthakur G, Burger J, et al. Significance of suboptimal response to imatinib, as defined by the european LeukemiaNet, in the long-term outcome of patients with early chronic myeloid leukemia in chronic phase. Cancer. 2009;115(16):3709–18 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Jabbour E, Saglio G, Hughes TP, Kantarjian H. Suboptimal responses in chronic myeloid leukemia: Implications and management strategies. Cancer. 2012;118(5):1181–91 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kantarjian HM, Larson RA, Guilhot F, O’Brien SG, Mone M, Rudoltz M, et al. Efficacy of imatinib dose escalation in patients with chronic myeloid leukemia in chronic phase. Cancer. 2009;115(3):551–60 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Koh Y, Kim I, Yoon SS, Kim BK, Kim DY, Lee JH, et al. Phase IV study evaluating efficacy of escalated dose of imatinib in chronic myeloid leukemia patients showing suboptimal response to standard dose imatinib. Ann. Hematol. 2010;89(7):725–31 [DOI] [PubMed] [Google Scholar]
- 13.Jabbour E, Kantarjian HM, Jones D, Shan J, O’Brien S, Reddy N, et al. Imatinib mesylate dose escalation is associated with durable responses in patients with chronic myeloid leukemia after cytogenetic failure on standard-dose imatinib therapy. Blood. 2009;113(10):2154–60 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Cortes JE, Baccarani M, Guilhot F, Druker BJ, Branford S, Kim DW, et al. Phase III, randomized, open-label study of daily imatinib mesylate 400 mg versus 800 mg in patients with newly diagnosed, previously untreated chronic myeloid leukemia in chronic phase using molecular end points: Tyrosine kinase inhibitor optimization and selectivity study. J Clin Oncol. 2010;28(3):424–30 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Petzer AL, Wolf D, Fong D, Lion T, Dyagil I, Masliak Z, et al. High dose imatinib improves cytogenetic and molecular remissions in pretreated Ph+/BCR-ABL+ CML chronic phase patients: First results from the randomized CELSG phase III CML 11 “ISTAHIT” study Haematologica. 2010;95(6):908–13 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Giles FJ, le Coutre PD, Pinilla-Ibarz J, Larson RA, Gattermann N, Ottmann OG, et al. Nilotinib in imatinib-resistant or imatinib-intolerant patients with chronic myeloid leukemia in chronic phase: 48-month follow-up results of a phase II study. Leukemia. 2013;27(1):107–12 [DOI] [PubMed] [Google Scholar]
- 17.Giles FJ, Kantarjian HM, le Coutre PD, Baccarani M, Mahon FX, Blakesley RE, et al. Nilotinib is effective in imatinib-resistant or -intolerant patients with chronic myeloid leukemia in blastic phase. Leukemia. 2012;26(5):959–62 [DOI] [PubMed] [Google Scholar]
- 18.le Coutre PD, Giles FJ, Hochhaus A, Apperley JF, Ossenkoppele GJ, Blakesley R, et al. Nilotinib in patients with ph+ chronic myeloid leukemia in accelerated phase following imatinib resistance or intolerance: 24-month follow-up results. Leukemia. 2012;26(6):1189–94 [DOI] [PubMed] [Google Scholar]
- 19.Nicolini FE, Turkina A, Shen ZX, Gallagher N, Jootar S, Powell BL, et al. Expanding nilotinib access in clinical trials (ENACT): An open-label, multicenter study of oral nilotinib in adult patients with imatinib-resistant or imatinib-intolerant philadelphia chromosome-positive chronic myeloid leukemia in the chronic phase. Cancer. 2012;118(1):118–26 [DOI] [PubMed] [Google Scholar]
- 20.Kantarjian HM, Giles FJ, Bhalla KN, Pinilla-Ibarz JA, Larson RA, Gattermann N, et al. Nilotinib is effective in patients with chronic myeloid leukemia in chronic phase following imatinib resistance or intolerance: 24-month follow-up results. Blood. 2011;117(4):1141–5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Yeung DT, Osborn M, White DL, Branford S, Kornhauser M, Slader C, et al. Upfront imatinib therapy in CML patients with rapid switching to nilotinib for failure to achieve molecular targets or intolerance achieves high overall rates of molecular response and a low risk of progression - an update of the TIDEL-II trial. Blood. 2011;118(21):451 [Google Scholar]
- 22.Saglio G, Hochhaus A, Guilhot F, Gatterman N, Wang MC, De Souza C, et al. Nilotinib is associated with fewer treatment failures and suboptimal responses vs imatinib in patients with newly diagnosed chronic myeloid leukemia in chronic phase (CML-CP): Results from ENESTnd. Haematologica. 2011;96(s2):58–9(Abstract 0145) [Google Scholar]
- 23.Cross NCP, White H, Müller MC, Saglio G, Hochhaus A. Standardized definitions of molecular response in chronic myeloid leukemia. Leukemia. 2012;26(10):2172–5 [DOI] [PubMed] [Google Scholar]