

Abstract
Objective:
The aim of this study was to estimate the orthodontic treatment need in a sample of 12-year-old Yemeni school children using the dental aesthetic index (DAI).
Materials and Methods:
The sample comprised 3003, 12-year-old children attending school in six of the governorates of Yemen. For each subject, the standard demographic information such as gender and age was collected, after which an intraoral examination for occlusal status using the DAI was performed.
Results:
The mean (SD) of DAI score was 24.86 (8.44) points (95% CI, 24.07-25.65). Overall, 36.6% of the sample found to have a dental appearance that requires orthodontic treatment, ranging from ‘selective’ to ‘mandatory’. Of whom, 19.0% presented with severe and handicapping malocclusion, requiring ‘definite’ and “mandatory’ treatment according to the DAI (DAI ≥ 31). Although there was no gender difference in the mean DAI score (P > 0.05), the sex distribution of the DAI treatment categories was significantly different (Chi-square = 13.258, df = 3, P = 0.004). The results of the individual DAI components showed that about 8% of the sample had more than one missing permanent teeth. Anterior maxillary and mandibular irregularity occurred in more than 33% of the sample. More than 30% of the children examined showed signs of crowding. Spacing in the incisal segments occurred in almost 25% of the sample. Almost 30% of the sample had an antero-posterior molar relation discrepancy.
Conclusion:
According to the findings of this study, almost one in five of the evaluated Yemeni school children had a DAI score above or equal to 31 points, suggesting highly desirable or mandatory orthodontic treatment need.
Keywords: Dental aesthetic index, orthodontic treatment need, Yemen
INTRODUCTION
A systematic and well-organized dental care program for any community requires some basic information such as the prevalence of the condition. In developing countries, such information is scarce. Despite efforts in the Arab world during the last decades to make health systems more equitable, access to dental health-care is still far from adequate, especially in poor communities.[1,2]
In the past, isolated epidemiological studies have been carried out in Arab countries to determine the prevalence of orthodontic treatment need. The reported prevalence of orthodontic need ranged from 17.4% in Iraq to 75.5% in Saudi Arabia.[3,4]
Regarding the perceived need for orthodontic treatment, it was also diverse. Farah[5] examined 101 9-10-year-old Iraqi children and found that 61% were willing to have orthodontic treatment. In Jordan, Abu Alhaija et al.[2] examined 1002 children with age ranging from 12 to 14 year-old and reported that 34% of the children were willing to accept orthodontic treatment. Finally, in Kuwait, it was reported that 36% of the 1076 children with age ranging from 14 to 18 year-old examined subjects would like to have orthodontic treatment.[6]
Eslamipour et al.,[7] reported that about 21.8% of the evaluated Iranian school children in their sample had a DAI score above or equal to 31 points, suggesting highly desirable or mandatory orthodontic treatment need. Another study in the same geographical area; however, reported significantly higher estimate of treatment need.[8,9]
The use of different indices, each one with its own approach, to record the orthodontic treatment need may have contributed to such reported differences.[10] The dental aesthetic index (DAI) is one of the indexes that directly combines professional's and perceived orthodontic need providing a single score linking the public's perceptions for dental aesthetics with objective measurements associated with the malocclusion. The DAI can be useful in both epidemiological surveys and as a screening device to prioritize subsidized orthodontic treatment in public programs where resources are insufficient to meet the demand.[11]
The DAI has been adopted by the World Health Organization as a cross-cultural index to be applied among diverse ethnic groups without modification.[12] Therefore, it can be used as an epidemiological index for using in developing countries, which lack a specifically developed orthodontic treatment need service.[13] It also has been used in some previous epidemiological studies all around the world. Yemen is a country on the Arabian Peninsula in Southwest Asia and is part of the Middle East. However, no available data on the prevalence, distribution and severity of malocclusion or the orthodontic treatment need of the population representative of the whole of Yemen is available. The lack of data on the distribution, prevalence and severity of malocclusion in Yemen likely affects the effective planning for the orthodontic services, which is needed to address the ever-increasing demand for orthodontic treatment.
Therefore, the aim of this study was to evaluate the prevalence and severity of selected malocclusion traits incorporated in the DAI index and orthodontic treatment need in a representative sample of 12-year-old Yemeni schoolchildren using the Dental Aesthetic Index (DAI).
MATERIALS AND METHODS
Ethical permission for this study was obtained from the general directorate of education in Yemen and the regional directorate of education in the governorates. A random sample of 12-year-old children was selected from schools in six randomly selected governorates from Yemen, which included 3003 subjects and consists of 1501 female and 1502 male.
In each governorate, the same multistage stratified sampling technique was implemented. From each sector, 500 children were included in the survey, half of whom were urban and the other half were rural. All school authorities were contacted and the aim of the study was explained for them to ensure full cooperation.
All children were examined seated in a chair with their head supported in an upright position and the examiner standing in front of the chair. Portable light was used to supplement natural daylight during the examination when needed. At the end of every day case sheets were reviewed to ensure the accuracy of recording.
DAI includes ten components that are later combined through rounded regression coefficients (weights). Scores for each component were multiplied by a previously reported weight and a constant was added to obtain a final DAI score for each child.[11,12] Cases are later classified based on four treatment need categories.
Statistical Analysis
The statistical package for the social sciences 13.0, IBM Corporation, New York, NY, was used for statistical analysis and the level of significance was set at 0.05 (P < 0.05). The following tests were performed:
Classification of data and calculation of frequencies for non-parametric variables.
Calculation of statistical parameters for parametric variables such as mean, standard deviation (SD) and 95% confidence interval of the mean DAI scores.
Analysis of the parametric variables by Student t-tests.
The gender distribution of DAI categories was compared using the Chi-square test.
RESULTS
The distribution of DAI scores for the sample is displayed in Figure 1. The highest DAI score recorded was 46 and the most commonly registered DAI score was 23. The mean (SD) of the DAI score was 24.86 (8.44) points. After dichotomizing the study sample according to the recommended cut-off point (DAI score of 31), 36.6% of the students required orthodontic treatment [Table 1].
Figure 1.
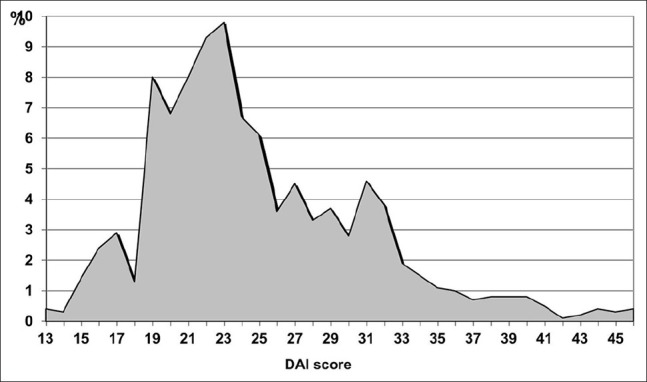
Distribution of the dental aesthetic index scores in the study sample
Table 1.
Distribution of the DAI scores in the study sample
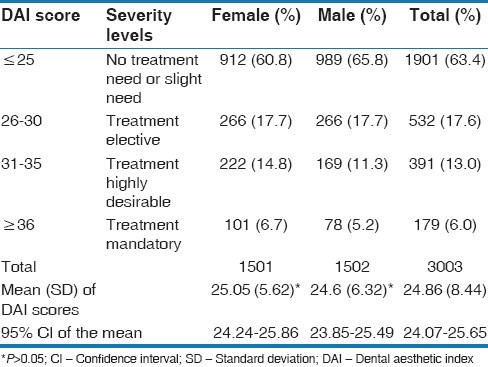
Almost two-third (63.4%) of the children examined had a dental appearance where orthodontic treatment need was considered “slight” or “not indicated.” Approximately, 17.6% fell into the malocclusion group where orthodontic treatment was considered as “elective.” The rest presented with malocclusions with severe to very severe severity according to the DAI (DAI ≥ 31), where orthodontic treatment were “highly desirable” (13.0%) or “mandatory” (6.0%).
Although there was no gender difference in the mean DAI score (P > 0.05), the sex distribution of the DAI treatment categories was significantly different (Chi-square = 13.258, df = 3, P = 0.004). Table 1 demonstrates that DAI scores of 31 and more, where there is severe malocclusion and treatment is highly desirable or mandatory, were more prevalent in females (21.5%) than males (16.5%) while DAI scores of 13-25 where there is no treatment need or slight need were found more prevalent in males (65.8%) than females (60.8%). Females showed a comparable mean (SD) for DAI scores 25.05 (5.62) to that of males 24.67 (6.32). This result was statistically insignificant (P > 0.05).
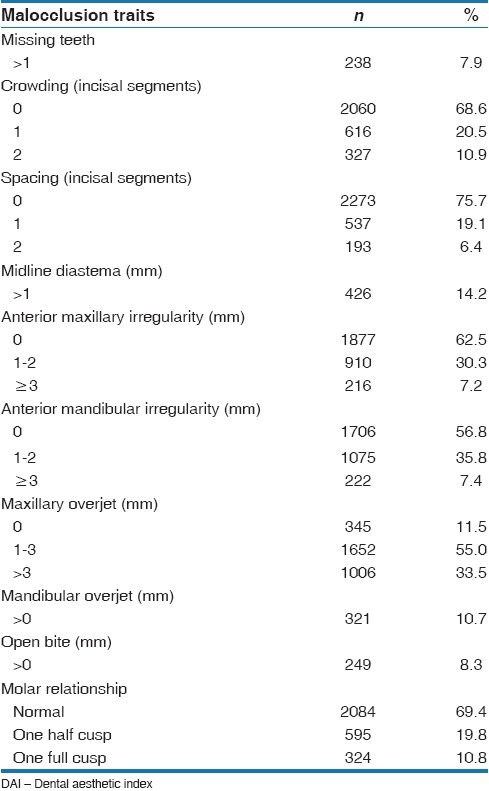
The distribution of the 10 components evaluated for obtaining the DAI score is shown in Table 2. The majority of the sample (69.4%) presented with a normal molar relationship and dental crowding was the most common malocclusion sign.
Table 2.
Selected malocclusion traits of Yemeni school children evaluated using the DAI
DISCUSSION
Although the DAI has been broadly used to determine orthodontic treatment need in epidemiological studies around the world over recent years, it has not been used to estimate the prevalence of malocclusion and orthodontic treatment need in Yemeni populations. The lack of data on the distribution, prevalence and severity of malocclusions in Yemen can potentially influence the effective planning for the orthodontic services, which is needed to address the ever-increasing demand for orthodontic treatment.
The use of dentition stage rather than chronological age as inclusion criteria for surveys using the DAI has not been used to evaluate the orthodontic treatment need in other adolescent populations, except in South Africa where one-third of school children (12 years) had a highly desirable or mandatory orthodontic treatment need.[14] The DAI was selected for this study because it has been recommended by the World Health Organization as a cross-cultural index.[12,15,16,17,18] It combines both objective occlusal and the subjective esthetic aspects of the occlusion;[11,19] although does not allow a clear differentiation between them. It has been claimed that the DAI was a relatively simple and highly reliable index that has been widely used.[20]
Similar to most previously used occlusal indices, DAI has some limitations such as its subjective nature, which is based on aesthetic evaluation of the frontal view of the dentition. It also does not assess all occlusal traits.[21,22] The DAI scores ranged between 13 and 46; the most commonly registered DAI score was 23 (9.8% of the sample). This result of the present investigation showed that the Yemeni, American and Iraqi samples had a comparable median.[3,23] Several studies have previously applied the DAI without modifications or adaptations to different ethnic or cultural settings.[17,19,21] Overall, 36.6% had a dental appearance that required orthodontic treatment, ranging from ‘selective’ to ‘mandatory’. At the cutoff point of 31 suggested by Jenny,[11] 19.0% presented with severe and handicapping malocclusion, requiring ‘definite’ and ‘mandatory’ treatment. When comparing these results with those found by others[22,24,25] the Yemeni sample seems to have a lower orthodontic treatment need than that of samples taken from Australian, New Zealanders or Malaysians. However, for a Nigerian sample, a lower treatment need was reported than that of the present study.[17] These differences might be due to racial variations.
An analysis of the DAI components sheds some light on selected malocclusion traits that are more commonly present. This analysis suggested that malocclusion in the present Yemeni school children can be characterized by significant dental crowding, a relatively high frequency of missing teeth, anterior mandibular overjet and anterior open bite [Table 2]. Only one previous study reporting analysis by components could be found in the Arabic world.[3] This type of analysis has been previously made in Spanish, Nigerian and Peruvian.[18,20,21] Differences in some of the DAI components help explain the differences in the DAI scores reported in the Yemeni and Iraqi school children. The Yemeni schoolchildren appeared to have higher orthodontic treatment needs. In the Iraqi populations,[3] the frequency of individuals presenting with at least one missing tooth was lower (3.4%) compared with the present findings (7.9%). Dental crowding in at least one dental arch was reported in 19.6% of Iraqi children, compared to 31.4% in the present study. The slight increase in the anterior arch dimension during normal development is not sufficient to overcome moderate to severe discrepancies. Therefore, crowding is likely to persist into the permanent dentition, particularly if it was initially severe.[26]
Jenny et al.[23] suggested that inherited differences in tooth size and arch size could be one reason for differences in DAI scores as the DAI includes measurements of the most relevant orthodontic traits that affect dental esthetics, such as crowding. The prevalence of anterior mandibular overjet, indicative of Class III malocclusion or anterior crossbite, was 10.7% in the present sample and that was twice of the reported prevalence by Al-Huwaizi.[3] Another study in the middle east also reported a relatively higher prevalence of Class III malocclusions in that region.[27] In the present study, 8.3% of the children presented with anterior openbite that was four-fold higher than what was found by Al-Huwaizi.[3] This difference may be attributed to varying prevalence of oral habits (i.e. digit sucking), which can have a major role in formation of anterior openbite. In a malocclusion study in Nigeria, on 12-to 13-year-old children, Otuyemi et al.[17] reported that anterior openbite was a common malocclusion trait and that it occurred in 10.2% of the rural and urban Nigerian communities.
When posterior occlusal relationships were compared between the two populations, molar relations other than Class I was similar in Yemeni (30.6%) and Iraqi school children (27.3%). The DAI has been used in the early permanent dentition stage.[28] Most of the present sample (73.9%) fell into that stage. For the rest of the sample some of the occlusal traits measured may improve with the transition from the mixed dentition stage to the permanent dentition stage, resulting in an improvement of the DAI score.[29] Differences in dentition stage according to gender has been reported; Girls were more dentally advanced.[14,24] These variations may be attributed to the differences in dental development and the early maturation of girls.[14,24]
At present, there is no doubt that in Yemen many children with severe and handicapping malocclusion are not receiving orthodontic treatment. As the general dental health and socio-economic status of the population of Yemen improve, it is more likely that the number of children seeking orthodontic treatment increases. This possible increase in patients seeking orthodontic care and the already high prevalence of malocclusion necessitates careful planning of adequate orthodontic services in Yemen. For orthodontic problems, prevention is unlikely to be highly effective as malocclusions change only a little and specific prevention measures for alignment or occlusal problems do not exist at present.[30] Interceptive orthodontic treatment can be very helpful in reducing the severity of the problems, but often later treatment becomes unnecessary.[27] Orthodontic services should therefore be comprehensive, delivering appropriate treatment in response to specific situations, resulting in the efficient treatment of non-skeletal and skeletal problems.
From the findings of the present investigation and other studies conducted elsewhere using the DAI, it appears that the prevalence and treatment need are slightly higher for younger children than for older groups.[7,15,24] This inverse relationship between chronological and DAI findings needs to be taken in consideration when using the DAI to plan orthodontic services. The use of dentition stage rather than chronological age as inclusion criteria for surveys using the DAI also needs to be explored.
To conclude, the limitations of the occlusal indices should be considered in the interpretation of the findings of this study, that is, the lack of evidence based criteria for measuring the malocclusion[31] or subjective nature of some of these indices.[32]
CONCLUSIONS
The DAI score ranged between 13 and 46 with a mean (SD) of 24.89 (8.44).
Malocclusion as assessed by DAI was characterized by a relatively high frequency of missing teeth, dental crowding, as well as a relatively high frequency of anterior mandibular overjet (Class III malocclusions).
According the DAI, almost 6% of the evaluated Yemeni school children had a mandatory need for orthodontic treatment. If the highly desirable category (DAI ≥ 31) is considered, the need would increase to one-fifth (19%) of the sample.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Abu Affan AH, Wisth PJ, Boe OE. Malocclusion in 12-year-old Sudanese children. Odontostomatol Trop. 1990;13:87–93. [PubMed] [Google Scholar]
- 2.Abu Alhaija ES, Al-Nimri KS, Al-Khateeb SN. Orthodontic treatment need and demand in 12-14-year-old north Jordanian school children. Eur J Orthod. 2004;26:261–3. doi: 10.1093/ejo/26.3.261. [DOI] [PubMed] [Google Scholar]
- 3.Al-Huwaizi AF. Doctorate Thesis. Iraq: College of Dentistry, University of Baghdad; 2002. Occlusal features, perception of occlusion, orthodontic treatment need and demand among 13-year-old Iraqi school children. [Google Scholar]
- 4.Al-Emran S, Wisth PJ, Böe OE. Prevalence of malocclusion and need for orthodontic treatment in Saudi Arabia. Community Dent Oral Epidemiol. 1990;18:253–5. doi: 10.1111/j.1600-0528.1990.tb00070.x. [DOI] [PubMed] [Google Scholar]
- 5.Farah ME. Master Thesis. Iraq: College of Dentistry, University of Baghdad; 1988. The orthodontic examination of children aged 9 and 10 years from Baghdad, Iraq: A clinical and radiographic study. [Google Scholar]
- 6.Kerosuo H, Abdulkarim E, Kerosuo E. Subjective need and orthodontic treatment experience in a Middle East country providing free orthodontic services: A questionnaire survey. Angle Orthod. 2002;72:565–70. doi: 10.1043/0003-3219(2002)072<0565:SNAOTE>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 7.Eslamipour F, Borzabadi-Farahani A, Asgari I. Assessment of orthodontic treatment need in 11-to 20-year-old urban Iranian children using the Dental Aesthetic Index (DAI) World J Orthod. 2010;11:e125–32. [PubMed] [Google Scholar]
- 8.Borzabadi-Farahani A, Borzabadi-Farahani A, Eslamipour F. Orthodontic treatment needs in an urban Iranian population, an epidemiological study of 11-14 year old children. Eur J Paediatr Dent. 2009;10:69–74. [PubMed] [Google Scholar]
- 9.Borzabadi-Farahani A, Borzabadi-Farahani A. Agreement between the index of complexity, outcome, and need and the dental and aesthetic components of the index of orthodontic treatment need. Am J Orthod Dentofacial Orthop. 2011;140:233–8. doi: 10.1016/j.ajodo.2010.09.028. [DOI] [PubMed] [Google Scholar]
- 10.Borzabadi-Farahani A. An overview of selected orthodontic treatment need indices. In: Naretto S, editor. Principles in Contemporary Orthodontics. Vienna, Austria: InTech; 2011. [Google Scholar]
- 11.Jenny J, Cons NC. Establishing malocclusion severity levels on the Dental Aesthetic Index (DAI) scale. Aust Dent J. 1996;41:43–6. doi: 10.1111/j.1834-7819.1996.tb05654.x. [DOI] [PubMed] [Google Scholar]
- 12.Geneva, Switzerland: World Health Organization; 1997. WHO. Oral Health Surveys: Basic Methods. [Google Scholar]
- 13.Jenny J, Cons NC. Comparing and contrasting two orthodontic indices, the index of orthodontic treatment need and the Dental Aesthetic Index. Am J Orthod Dentofacial Orthop. 1996;110:410–6. doi: 10.1016/s0889-5406(96)70044-6. [DOI] [PubMed] [Google Scholar]
- 14.Drummond RJ. Master Thesis. South Africa: College of Dentistry, University of Pretoria; 2003. Orthodontic status and treatment need of 12-year-old children in South Africa: An epidemiological study using the dental aesthetic Index. [PubMed] [Google Scholar]
- 15.Cons NC, Jenny J, Kohout FJ, Songpaisan Y, Jotikastira D. Utility of the dental aesthetic index in industrialized and developing countries. J Public Health Dent. 1989;49:163–6. doi: 10.1111/j.1752-7325.1989.tb02054.x. [DOI] [PubMed] [Google Scholar]
- 16.Cons NC, Jenny J, Kohout FJ, Jakobsen J, Shi Y, Ying WH, et al. Comparing ethnic group-specific DAI equations with the standard DAI. Int Dent J. 1994;44:153–8. [PubMed] [Google Scholar]
- 17.Otuyemi OD, Ogunyinka A, Dosumu O, Cons NC, Jenny J, Kohout FJ, et al. Perceptions of dental aesthetics in the United States and Nigeria. Community Dent Oral Epidemiol. 1998;26:418–20. doi: 10.1111/j.1600-0528.1998.tb01981.x. [DOI] [PubMed] [Google Scholar]
- 18.Baca-Garcia A, Bravo M, Baca P, Baca A, Junco P. Malocclusions and orthodontic treatment needs in a group of Spanish adolescents using the Dental Aesthetic Index. Int Dent J. 2004;54:138–42. doi: 10.1111/j.1875-595x.2004.tb00269.x. [DOI] [PubMed] [Google Scholar]
- 19.Cons NC, Jenny K, Kohout FJ. Iowa: College of Dentistry, University of Iowa; 1986. DAI: The Dental Aesthetic Index. [Google Scholar]
- 20.Onyeaso CO. Orthodontic treatment need of Nigerian outpatients assessed with the Dental Aesthetic Index. Aust Orthod J. 2004;20:19–23. [PubMed] [Google Scholar]
- 21.Bernabé E, Flores-Mir C. Orthodontic treatment need in Peruvian young adults evaluated through dental aesthetic index. Angle Orthod. 2006;76:417–21. doi: 10.1043/0003-3219(2006)076[0417:OTNIPY]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 22.Borzabadi-Farahani A, Eslamipour F, Asgari I. A comparison of two orthodontic aesthetic indices. Aust Orthod J. 2012;28:30–6. [PubMed] [Google Scholar]
- 23.Jenny J, Cons NC, Kohout FJ, Jakobsen J. Differences in need for orthodontic treatment between Native Americans and the general population based on DAI scores. J Public Health Dent. 1991;51:234–8. doi: 10.1111/j.1752-7325.1991.tb02221.x. [DOI] [PubMed] [Google Scholar]
- 24.Johnson M, Harkness M. Prevalence of malocclusion and orthodontic treatment need in 10-year-old New Zealand children. Aust Orthod J. 2000;16:1–8. [PubMed] [Google Scholar]
- 25.Abdullah MS, Rock WP. Assessment of orthodontic treatment need in 5,112 Malaysian children using the IOTN and DAI indices. Community Dent Health. 2001;18:242–8. [PubMed] [Google Scholar]
- 26.Proffit WR. 4th ed. St Louis: Mosby; 2007. Contemporary Orthodontics. [Google Scholar]
- 27.Borzabadi-Farahani A, Borzabadi-Farahani A, Eslamipour F. Malocclusion and occlusal traits in an urban Iranian population. An epidemiological study of 11-to 14-year-old children. Eur J Orthod. 2009;31:477–84. doi: 10.1093/ejo/cjp031. [DOI] [PubMed] [Google Scholar]
- 28.Otuyemi OD, Jones SP. Methods of assessing and grading malocclusion: A review. Aust Orthod J. 1995;14:21–7. [PubMed] [Google Scholar]
- 29.Estioko LJ, Wright FA, Morgan MV. Orthodontic treatment need of secondary schoolchildren in Heidelberg, Victoria: An epidemiologic study using the Dental Aesthetic Index. Community Dent Health. 1994;11:147–51. [PubMed] [Google Scholar]
- 30.Kelly JE, Harvey CR. Vital and health statistics. Vol. 11. Washington DC: National Center for Health Statistics, DHEP Publication NO. 77-1644; 1977; 1977. An Assessment of the Occlusion of the Teeth in Youths 12-17 Years; p. 162. [PubMed] [Google Scholar]
- 31.Borzabadi-Farahani A. A review of the oral health-related evidence that supports the orthodontic treatment need indices. Prog Orthod. 2012;13:314–25. doi: 10.1016/j.pio.2012.03.002. [DOI] [PubMed] [Google Scholar]
- 32.Borzabadi-Farahani A. A review of the evidence supporting the aesthetic orthodontic treatment need indices. Prog Orthod. 2012;13:304–13. doi: 10.1016/j.pio.2012.03.003. [DOI] [PubMed] [Google Scholar]