

Abstract
Background Spontaneous flexor tendon rupture is considered to be invariably associated with previous hand/wrist injury or systemic disease such as rheumatoid arthritis.
Case Description A 54-year-old man presented with a 4-month history of mild ulnar wrist pain and spontaneous left little finger flexion loss in the absence of distant/recent trauma and systemic arthropathy. Surgical exploration confirmed a zone IV left little finger flexor digitorum profundus (FDP5) attritional rupture (100%), ring finger flexor digitorum profundus (FDP4) attenuation (40%) and a disrupted lunotriquetral ligament and volar-ulnar wrist capsule. Volar subluxation of the narrowed carpal tunnel resulted in flexor tendon attrition against the hamate hook. A side-to-side tendon transfer was performed along with a lunotriquetral ligament repair and temporary Kirschner wire fixation. At 6 months the patient had full active, synchronous flexion of the ring and little fingers and reduced wrist pain.
Literature Review Traumatic flexor tendon ruptures have been reported following distal radius/hamate hook fractures, from carpal bone osteophytes, accessory carpal bones and intraosseous ganglia. Attritional ruptures caused by chronic, degenerative carpal pathology are less common.
Clinical Relevance This case highlights an unusual cause of flexor tendon rupture due to chronic carpal instability.
Keywords: attrition rupture, flexor tendon, hamate, lunate subluxation, carpal instability
We present an unusual case of an attritional rupture of the little finger flexor digitorum profundus (FDP5) tendon due to degenerative wrist disease, within the carpal tunnel, in the absence of known trauma or systemic disease. In addition to tendon rupture, multiple other chronic, degenerative wrist abnormalities were found.
Case Report
A 54-year-old, right handed, healthy male computer operator was referred with a 4-month history of left ulnar wrist pain, a loss of active little finger flexion involving both the proximal (PIP) and distal (DIP) interphalangeal joints, but no history of recent/distant trauma. Fifteen months earlier he had undergone carpal tunnel decompression, which helped the numbness and tingling, but he continued to complain of wrist pain (7/10 on the visual analog scale [VAS]) and grip weakness (left = 25 kg, right = 50 kg). Wrist examination revealed 45° of extension, 55° of flexion, preserved pronosupination, radial-ulnar deviation, and mild foveal tenderness. The Watson scaphoid shift test was negative.
Plain radiographs demonstrated advanced scaphotrapeziotrapezoid (STT) osteoarthritis (OA) with dorsal malrotation of the lunate. Magnetic resonance imaging (MRI) confirmed a flexor tendon sheath effusion, STT joint osteoarthritis, and a central triangular fibrocartilage complex (TFCC) perforation (Fig. 1). Ultrasound was inconclusive for the level of tendon disruption. Serological testing excluded a systemic arthritic disease, autoimmune disorder, or infective etiology.
Fig. 1.

Magnetic resonance image showing STT joint osteoarthritis, with attenuation of the volar wrist capsulo-ligamentous support; Protrusion of the lunate into the carpal tunnel with compression (arrow) of the flexor tendons (F). M = median nerve.
At surgery, exploration of the carpal tunnel revealed an attritional rupture of the little finger flexor digitorum profundus (FDP5) tendon at the level of the hamate hook (Fig. 2) and a 40% rupture of the ring finger flexor digitorum profundus (FDP4) tendon. This was repaired with a continuous 5–0 polypropylene suture (Prolene, Ethicon Inc., Somerville, NJ, USA). The little finger flexor digitorum superficialis tendon was in continuity, but rudimentarily thin. The volar-ulnar wrist capsule and the volar portion of the lunotriquetral ligament were completely disrupted with frayed, degenerate remnants over the corresponding bones (Fig. 3). The scapholunate ligament was not visualized.
Fig. 2.
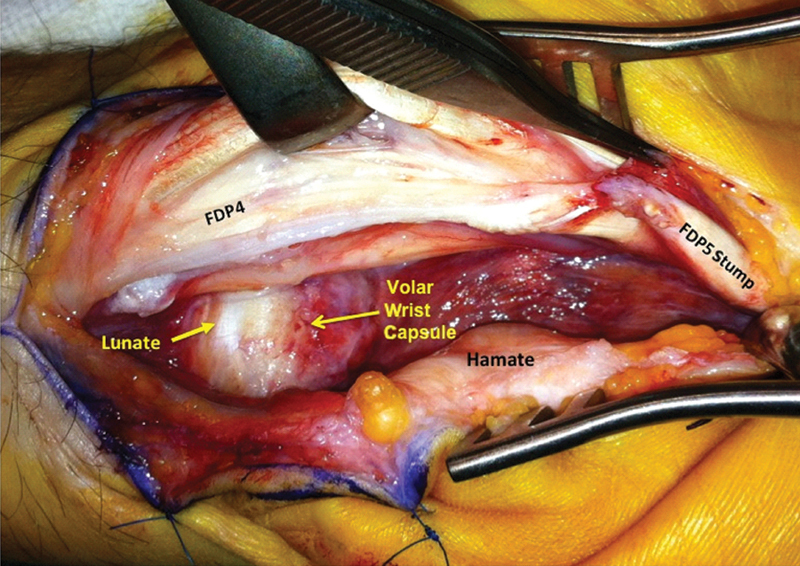
Intraoperative photograph showing 100% disruption of the flexor digitorum profundus to the little finger (FDP5) at the level of the hamate hook (retracted), attritional thinning of the ring finger flexor digitorum profundus (FDP4), disrupted volar wrist capsule and protruding lunate at the base of the carpal tunnel.
Fig. 3.

Intraoperative photograph showing complete disruption of the volar portion of the lunotriquetral ligament (LTq) with frayed, degenerate remnants over the corresponding bones.
The lunate was found to be protruding into the carpal tunnel, but with neither visible nor palpable bony spurs. The lunotriquetral ligament was repaired with 1–0 polyethylene terephthalate (Ethibond EXCEL, Ethicon Inc., Somerville, NJ, SA) interrupted sutures and the joint temporarily stabilized with two Kirschner wires (K-wires). The distal stump of the FDP5 was sutured to FDP4, just distal to zone 3, using a 3–0 polypropylene (Prolene, Ethicon Inc., Somerville, NJ, USA) Pulvertaft weave technique. Histological and microbiological examination of the flexor tendon synovium was unremarkable. The K-wires were removed at 6 weeks.
At 6 months the patient had 180° of composite finger flexion. The wrist pain was 1/10 on the VAS, and there was 40° of wrist joint flexion, 35° of extension, 80% of pronosupination, and improved grip strength (35 kg). The patient was happy with the outcome and declined further treatment.
Discussion
Flexor tendon ruptures are most commonly caused by hand/wrist trauma, having been reported following distal radius fractures/malunion, hamate hook fractures, osteophytes, accessory carpal bones, and intraosseous ganglia.1 2 3 4 5 Attritional ruptures caused by chronic, degenerative carpal pathology are, however, rare. The most widely known include a flexor pollicis longus rupture against a scaphoid osteophyte (the Mannerfelt lesion) or an attritional rupture of ring and little finger extensor tendons against a bony spicule on the ulnar aspect of the wrist (Vaughan-Jackson lesion).6 7 A collapsed lunate was found to be responsible for an attritional rupture of the extensor tendon to the middle and ring fingers in two patients with Kienböck disease.8 Similar to our described case, an attritional rupture caused by lunate malposition has been reported, but in patients with significant previous carpal trauma. Palmar dislocation of the lunate has been reported as a cause of attritional rupture of multiple flexor tendons as late as 40 years after the injury.9 A case of FDP5 tendon attrititional rupture has also been reported secondary to pisotriquetral instability.10 Similarly, FDP5 rupture due to pisotriquetral osteoarthritis and nonrheumatoid bony irregularities in the carpal tunnel have also been reported.1 11 12 Conversely, a dorsal intercalated segment instability (DISI) deformity may typically lead to rupture of the index or thumb flexor tendons due to the malrotated bony prominence of the scaphoid tuberosity in the rheumatoid wrist.13 14
Funding
None
Footnotes
Conflict of Interest None
References
- 1.Takami H, Takahashi S, Ando M. Attritional flexor tendon ruptures after a malunited intra-articular fracture of the distal radius. Arch Orthop Trauma Surg. 1997;116(8):507–509. doi: 10.1007/BF00387589. [DOI] [PubMed] [Google Scholar]
- 2.Crosby E B, Linscheid R L. Rupture of the flexor profundus tendon of the ring finger secondary to ancient fracture of the hook of the hamate. Review of the literature and report of two cases. J Bone Joint Surg Am. 1974;56(5):1076–1078. [PubMed] [Google Scholar]
- 3.Hattori Y, Doi K, Hoshino S, Sakamoto S, Yukata K. Attritional rupture of the flexor tendons to the small finger caused by osteophyte of the ulnar head: case report. J Hand Surg Am. 2010;35(1):24–26. doi: 10.1016/j.jhsa.2009.09.009. [DOI] [PubMed] [Google Scholar]
- 4.Koizumi M, Kanda T, Satoh S, Yoshizu T, Maki Y, Tsubokawa N. Attritional rupture of the flexor digitorum profundus tendon to the index finger caused by accessory carpal bone in the carpal tunnel: a case report. J Hand Surg Am. 2005;30(1):142–146. doi: 10.1016/j.jhsa.2004.08.007. [DOI] [PubMed] [Google Scholar]
- 5.Yamazaki H, Kato H, Murakami N. Closed rupture of the flexor tendons of the index finger caused by a pathological fracture secondary to an intraosseous ganglion in the lunate. J Hand Surg Eur Vol. 2007;32(1):105–107. doi: 10.1016/j.jhsb.2006.08.001. [DOI] [PubMed] [Google Scholar]
- 6.Mannerfelt L, Norman O. Attrition ruptures of flexor tendons in rheumatoid arthritis caused by bony spurs in the carpal tunnel. A clinical and radiological study. J Bone Joint Surg Br. 1969;51(2):270–277. [PubMed] [Google Scholar]
- 7.Vaughan-Jackson O J. Rupture of extensor tendons by attrition at the inferior radio-ulnar joint; report of two cases. J Bone Joint Surg Br. 1948;30B(3):528–530. [PubMed] [Google Scholar]
- 8.Inoué G. Attritional rupture of the extensor tendon due to longstanding Kienböck's disease. Ann Chir Main Memb Super. 1994;13(2):135–138. doi: 10.1016/s0753-9053(05)80386-2. [DOI] [PubMed] [Google Scholar]
- 9.Johnston G H, Bowen C V. Attritional flexor tendon ruptures by an old lunate dislocation. J Hand Surg Am. 1988;13(5):701–703. doi: 10.1016/s0363-5023(88)80128-x. [DOI] [PubMed] [Google Scholar]
- 10.Corten E M, van den Broecke D G, Kon M, Schuurman A H. Pisotriquetral instability causing an unusual flexor tendon rupture. J Hand Surg Am. 2004;29(2):236–239. doi: 10.1016/j.jhsa.2003.11.010. [DOI] [PubMed] [Google Scholar]
- 11.Saitoh S, Kitagawa E, Hosaka M. Rupture of flexor tendons due to pisotriquetral osteoarthritis. Arch Orthop Trauma Surg. 1997;116(5):303–306. doi: 10.1007/BF00390059. [DOI] [PubMed] [Google Scholar]
- 12.Stevenson T R, Louis D S, Zucker S E. Rupture of flexor tendons to the little finger due to bony irregularities in the carpal tunnel. J Hand Surg [Br] 1988;13(3):308–310. doi: 10.1016/0266-7681_88_90095-2. [DOI] [PubMed] [Google Scholar]
- 13.Zangger P, Simmen B R. Spontaneous ruptures of flexor tendons secondary to extreme DISI deformity of the lunate in a rheumatoid wrist. A case report. Ann Chir Main Memb Super. 1993;12(4):250–256. doi: 10.1016/s0753-9053(05)80022-5. [DOI] [PubMed] [Google Scholar]
- 14.Baer W, Dumont C E. Mechanical wearing down of flexor tendons in rheumatoid arthritis as a result of extreme volar-flexed intercalated segment instability. Scand J Plast Reconstr Surg Hand Surg. 2002;36(3):189–191. doi: 10.1080/028443102753718113. [DOI] [PubMed] [Google Scholar]