

Abstract
Background
The burden of ill-health due to inactivity has recently been highlighted. Better studies on environments that support physical activity are called for, including longitudinal studies of environmental interventions. A programme of residential street improvements in the UK (Sustrans ‘DIY Streets’) allowed a rare opportunity for a prospective, longitudinal study of the effect of such changes on older adults’ activities, health and quality of life.
Methods
Pre–post, cross-sectional surveys were carried out in locations across England, Wales and Scotland; participants were aged 65+ living in intervention or comparison streets. A questionnaire covered health and quality of life, frequency of outdoor trips, time outdoors in different activities and a 38-item scale on neighbourhood open space. A cohort study explored changes in self-report activity and well-being postintervention. Activity levels were also measured by accelerometer and accompanying diary records.
Results
The cross-sectional surveys showed outdoor activity predicted by having a clean, nuisance-free local park, attractive, barrier-free routes to it and other natural environments nearby. Being able to park one's car outside the house also predicted time outdoors. The environmental changes had an impact on perceptions of street walkability and safety at night, but not on overall activity levels, health or quality of life. Participants’ moderate-to-vigorous activity levels rarely met UK health recommendations.
Conclusions
Our study contributes to methodology in a longitudinal, pre–post design and points to factors in the built environment that support active ageing. We include an example of knowledge exchange guidance on age-friendly built environments for policy-makers and planners.
Keywords: Walking, Intervention Effectiveness, Outdoor Medicine
Background
In July 2012, The Lancet committed one issue to a series of papers on the importance of physical activity for physical and mental health and on the burden of ill-health due to inactivity. ‘Physical inactivity is a significant predictor of cardiovascular disease, type 2 diabetes mellitus, obesity, some cancers, poor skeletal health, some aspects of mental health, and overall mortality, as well as poor quality of life’.1 Yet, most older adults in the developed world are not sufficiently active; in the UK less than 25% of adults aged 65–74 and less than 13% of those aged 75+ meet general recommended levels of physical activity for adults (at least 150 min of moderate intensity activity per week in bouts of 10 min or more).2 3 With the number and proportion of adults aged 65+ increasing worldwide—in the UK, for example, the fastest-growing age group is aged 85 years and older—there is an urgent and growing need to consider how adults can maintain health-protective activity into old age.4 Physical activity not only can improve the physical and psychological health of older adults, including maintaining healthy brain structure, but it can also assist in reversing the decline of physical function even in late old age.4 5 Remaining active into old age can also help prevent social isolation, identified as a major problem for older adults and linked to a variety of adverse physical and mental health outcomes.6
The same volume of Lancet states: “There has been far too little consideration of the social and physical environments that enable [everyday] activity to be taken.”7 Good environmental planning should lead to the design of a built environment that supports public health.8 9 Following Van Cauwenberg et al,10 we define built environment here as ‘the objective and perceived characteristics of the physical context in which people spend their time (eg, home, neighborhood)’, including aspects of detailed design (eg, sidewalks and seating), traffic density and speed, locations for physical activity (eg, streets and parks), crime and safety. Historically, urban built environments were developed as walkable places before motor car ownership and use predominated.8 Recently, there has been a renewed interest in ways that built environment can be supportive of, or inhibit, physical activity.11
Social ecological models of behaviour have been recommended as a way to consider more carefully the role of the physical environment in relation to activity.12–15 Social ecological models recognise that individual characteristics and preferences are active within the context of socioeconomic, political, cultural and environmental factors that operate at different scales, from household and community to wider geographic levels.16 Development of a ‘walkability index’ in the US context, based on land-parcel level, objective measures of neighbourhood environment and drawing on an ecological model, recognised that environmental influences on older adults’ walking deserve further investigation.17
Being physically active can be ‘a major contributor to one's overall physical and mental wellbeing. Positive outcomes include a sense of purpose and value, a better quality of life, improved sleep, and reduced stress, as well as stronger relationships and social connectedness’.7 Aspects of the physical environment in and around older people's homes may represent a greater constraint on activities than for other adult age groups18–20 and the environment can become a limiting factor on people's mobility (their physical ability to undertake everyday activities such as walking, climbing stairs, etc) as their functional capabilities change in old age.21 A built environment that makes it easy and enjoyable to be active outdoors is therefore contributing to the quality of life in multiple ways. Such a supportive built environment has been shown to be a significant predictor of older people's walking activity, beyond factors of age, sex, socioeconomic status or living arrangement.22 23 Attributes of the environment associated with higher levels of walking (for adults aged 65+) included good-quality paving and tree-lined walks en route to local open spaces, as well as a lack of incivilities such as dog fouling.24 Studies on utilitarian walking routes only for adults aged 55+ in the Netherlands25 found that parks and green strips were apparently inhibitors of walking, as were changes in level, litter on the streets and ‘blind’ or windowless walls facing the streets. Those factors that supported walking were good pavements, front gardens, dwellings or shops at street level and low traffic volume. Such studies suggest that environmental improvements might influence activity levels in older adults and in turn have benefits for wider social wellbeing and quality of life.
A recent review called for more studies in different contexts utilising longitudinal designs, standardised, reliable and validated physical activity and environmental measurements, and the investigation of possible moderating effects.10 We were provided with a rare opportunity to assess a programme of residential street improvements in the UK, across a range of socioeconomic contexts, in a prospective, longitudinal study of the effect of the street improvements on older adults’ activities and quality of life. The environmental interventions were part of the ‘Liveable Neighbourhoods’ programme promoted by Sustrans, a sustainable transport charity in the UK (http://www.sustrans.org.uk). Under their ‘DIY (Do It Yourself) Streets’ pilot projects, Sustrans partnered with local communities to intervene using urban and landscape design to make streets safer and more attractive, for example, by inserting planters, changing parking space provision and layout, and by the addition of features to reduce the speed and volume of traffic.
This is an emerging field of research; we highlight here a natural experiment undertaken in UK urban contexts. There may be similar opportunities to apply outcomes from this in other locations around the world and this study contributes to discussions on what constitute apposite instruments for this type of research. We also share some of the key findings as a prelude to more detailed forthcoming publications.
Aims
We had three principal aims:
To understand the influence of aspects of the built environment on older adults’ outdoor activity, wellbeing and quality of life through two waves of cross-sectional survey, preintervention and postintervention.
To evaluate the effect of changes to the residential street environment on a cohort of older adults’ activity, wellbeing and quality of life.
To investigate the levels of physical activity in older adult participants, measured objectively by accelerometer, in relation to self-reported outdoor activities.
Methods
Study design
Cross-sectional surveys
Nine sites planned for intervention were chosen for the study, located in urban areas in England, Wales and Scotland and including the majority of the projects in Sustrans’ ‘DIY Streets’ pilot phase. We paired each intervention street with a local comparison street where no intervention was undertaken, matched as closely as possible in terms of housing type, street layout and socioeconomic status as measured by the relevant Index of Multiple Deprivation for the local census area.26
We undertook preintervention and postintervention questionnaire surveys by interview. All data were collected between May and September, the summer months in Britain, to minimise effects of variation in season. Preintervention, baseline data were collected in 2008 and again an average of 2 years later, between 3 and 6 months postintervention (due to difficulties and delays in implementation of the interventions, only seven sites were available for postintervention survey).
Longitudinal cohort survey
A subset of the participants in the baseline survey described above was recruited as a longitudinal cohort, surveyed by questionnaire interview both preintervention and postintervention.
Activity survey
Additional data were collected from participants on their activity levels: objective measures and self-reported frequency, type and location of activities that involved going outdoors.
Recruitment of participants
Cross-sectional surveys
The target participants were all those aged 65 or older living on the intervention or comparison streets in each study site. Participants were recruited by door-to-door leafleting and through community meetings and information sessions facilitated by the Sustrans project officers and local community leaders. The sample of 96 at baseline (n=56 in intervention, n=40 in comparison streets) was estimated to be c. 50% of the target population, based on 2001 local area census data. The sample postintervention was 61 (n=29 in intervention, n=32 in comparison streets; see table 1).
Table 1.
Participant characteristics for the cross-sectional survey samples
| Cross-sectional study | ||||
|---|---|---|---|---|
| 2008 | 2010/2011 | |||
| Intervention group, n=56 | Comparison group, n=40 | Intervention group, n=29 | Comparison group, n=32 | |
| Age: mean (SD) | 75.92 (7.3) | 74.11 (7.35) | 77.00 (8.24) | 73.77 (6.3) |
| Sex (% male) | 49.0 | 37.0 | 37.9 | 34.4 |
| Ethnicity (% not white British) | 24.5% | 11.1% | 20.6% | 15.7% |
| Functional capability* | 2.02 (0.76) | 2.11 (0.91) | 1.80 (0.77) | 1.91 (0.95) |
| Living arrangement (%) | ||||
| At home alone | 48.0 | 39.1 | 44.8 | 38.7 |
| At home with other(s) | 52.0 | 34.8 | 55.2 | 41.9 |
| Sheltered housing alone | – | 26.1 | – | 19.4 |
*Measure has a range 1–5 with higher levels associated with lower functional ability.
Longitudinal cohort
All participants in the baseline, cross-sectional survey were invited to participate in the longitudinal study, that is, to be surveyed preintervention and postintervention. We retained 51% of participants from baseline in this cohort (n=36; see table 2).
Table 2.
Participant characteristics for the longitudinal cohort
| Longitudinal cohort | ||||
|---|---|---|---|---|
| 2008 | 2010/11 | |||
| Intervention group, n=20 | Comparison group, n=16 | Intervention group, n=20 | Comparison group, n=16 | |
| Age: mean (SD) | 73.84 (7.49) | 70.87 (4.83) | ||
| Sex (% male) | 36.8 | 31.3 | ||
| Ethnicity (% not white British) | 20.0 | 12.6 | ||
| Functional capability* | 1.90 (0.84) | 1.84 (1.03) | 1.84 (0.78) | 1.92 (0.97) |
| Living arrangement (%) | ||||
| At home alone | 55.0 | 37.5 | 50.0 | 37.5 |
| At home with other(s) | 45.0 | 50.0 | 50.0 | 50.0 |
| Sheltered housing alone | – | 12.5% | – | 12.5% |
*Measure has a range of 1–5 with higher levels associated with lower functional ability
Activity survey
All participants in the cross-sectional surveys preintervention and postintervention were also invited to participate in the activity survey. We present here the findings from the baseline survey (n=47; see table 3) as postintervention data (n=22) have yet to be analysed.
Table 3.
Participant characteristics for the baseline activity survey Activity study 2008
| n=50 | |
|---|---|
| Age: mean (SD) | 74.19 (7.62) |
| Sex (% male) | 44.7 |
| Ethnicity (% not white British) | 6.5 |
| Functional capability* | 1.88 (0.785) |
| Living arrangement(%) | |
| At home alone | 46.8 |
| At home with other(s) | 36.2 |
| Sheltered housing alone | 17.0 |
*Measure has a range of 1–5 with higher levels associated with lower functional ability.
Figure 1 shows the numbers of participants for each survey at baseline and follow-up.
Figure 1.

Participant numbers in each survey, by intervention or comparison group preintervention and postintervention.
Measurements and analysis
Cross-sectional survey
Measures
All participants were invited to complete a multiscale questionnaire by interview. The principal outcome measures were general health (EQ-5D)27 and quality of life (CASP-19).28 Secondary outcome measures, as potential mediators, were frequency of outdoor visits in a typical summer month and typical time spent outdoors in relation to utilitarian walking, recreational walking, gardening, outdoor sports and other outdoor activities.23 Independent variables were perceptions of the outdoor environment around the home, local street and local neighbourhood, building on a neighbourhood open space (NOS) scale developed in previous work with older adults in the UK.23 Postintervention, the survey included additional questions asking for perceived change in physical activity, knowing neighbours and neighbourhood tranquillity compared with 2 years ago.
The following additional personal data were collected: age, gender, ethnicity, living arrangement and functional capability (an adapted version of IADL (Instrumental Activities of Daily Living)29). Control variables were selected from these data for use in subsequent analyses.
Analysis
Differences (t-test) preintervention and postintervention were examined for each variable, taking into account whether participants lived in intervention or comparison streets. The difference in the degree of change over time (t-test) was also examined for each variable between intervention and comparison groups. To assist in analysis of the NOS variables, the 38 items in the NOS scale were reduced to 9 factors using factor analysis (maximum likelihood method) and the resultant variables re-examined in the same way.
To test the relationship between NOS factors and our primary and secondary outcome measures, we used hierarchical blocked linear regressions, with potentially confounding variables in the first block and independent variables in the second. The univariate relationship between variables of interest and outcome variables were first tested using non-parametric tests (Mann–Whitney U or Kruskal–Wallis). Only those variables showing correlation with the outcome variable were included in each regression model. As the functional capability measure,29 was frequently the only predictor of outcome measures, we have indicated where regressions were run again excluding this variable, to identify environmental factors that may covary with IADL (see table 4).
Table 4.
Linear regression results: factors predicting outcome measures of interest across full dataset preintervention (2008, n=96) and postintervention (2010/2011, n=61)
| Outcome measure | CASP 19 | EUROQOL (EQ-5D) | EUROQOL (VAS) | Unhealthy days (no.) | Summer activity | Time outdoors | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2008 | 2010/2011 | 2008 | 2010/2011 | 2008 | 2010/2011 | 2008 | 2010/2011 | 2008 | 2010/2011 | 2008 | 2010/2011 | |
| R2 | 0.503 (0.247) | 0.522 (0.209) | 0.407 (0.103) | 0.606 (0.329) | 0.302 (0.111) | 0.479 (0.317) | 0.221 (0.221) | 0.550 (0.375) | 0.249 (0.189) | 0.393 (0.308) | 0.187 (0.117) | 0.283 (0.208) |
| F | 10.875 (4.083) | 9.483 (2.803) | 11.403 (3.535) | 9.633 (5.139) | 9.624 (3.735) | 9.576 (6.159) | 2.199 (3.023) | 8.379 (4.907) | 5.162 (4.594) | 5.504 (4.623) | 3.827 (2.774) | 4.108 (3.477) |
| Control variable | ||||||||||||
| Age | (−0.200)* | (−0.227)* | (−0.299)* | |||||||||
| IADL | −0.590*** | −0.616*** | −0.590*** | −0.550*** | −0.493** | −0.443*** | 0.513*** | −0.274* | −0.327* | −0.270** | −0.331* | |
| Predictor variable | ||||||||||||
| Factor 1 pleasant local open space | −0.204* (−0.224)* | |||||||||||
| Factor 2 barriers/nuisance in local open space and neighbourhood | (−0.286)** | (−0.323)** | (−0.410)** | (−0.340**) | (0.427)** | (−0.247)* | (−0.309)* | |||||
| Factor 3 bad footways/paths | −0.362** (−0.432)** | 0.247* (0.338)* | ||||||||||
| Factor 7 easy to get out and about | 0.168* (0.231)* | 0.228* (0.236)* | ||||||||||
| Factor 8 good paths and cycleways | 0.280** | 0.282* (0.367)** | −0.340* (−0.340)* | (0.293)* | ||||||||
Only significant results (standardised coefficients, β values) are reported for predictor variables.
Brackets indicate co-efficient after IADL variable removed from regression equation.
*Significant at p<0.05.
**Significant at p<0.01.
***Significant at p<0.001.
Longitudinal cohort
We used the same analytical approach for the cohort study as for the cross-sectional survey described above.
Activity survey
Measures
We assessed physical activity by accelerometry using an Actigraph GT1M (Pensacola, FL, USA), recording intensity of activity in counts/minute. Participants wore accelerometers for 7 days. Participants also completed a daily activity diary for the same, 7-day period. They recorded activity that took them outside the home, including the time of day, duration, destination and type of activity involved in each trip. Multiple activities could be indicated for any one outdoor trip.
Analysis
We classified the intensity of physical activity according to ‘moderate-to-vigorous’, ‘low-light’ and ‘high-light’ levels by accelerometry.30–32 Low-light activity was 100–1040 counts/min and high-light was 1041–1951 counts/min. We report activity in terms of minutes per hour and by time of day.
Results
Cross-sectional surveys
For participants living on intervention streets, there was a positive change postintervention in perceptions that ‘most of the streets and paths in my neighbourhood are safe to walk after dark’ (p=0.04). However, self-reported frequency of summer outdoor activities had declined (p=0.02). There was also a negative change in perceptions relating to factor 4 (good outdoor facilities, including garden and parking, at home; p=0.02). For those living in the comparison streets, there were no significant differences in measures over time.
Table 4 shows the NOS factors that were significant in blocked linear regression models to predict primary and secondary outcome measures in the baseline (2008) and postintervention (2010/2011) surveys. A power calculation was carried out for the multiple regression R2 value and number of predictors in table 4. Results showed that the sample size for α=0.05 and power=0.8 was adequate for both the 2008 and the 2010/2011 outcome measures in the table.
Factor 2, covering barriers and nuisances (including ‘steep hills and steps in the neighbourhood’, ‘problems with youths hanging around’, ‘dogs and dog fouling’ and barriers such as ‘busy roads’) is a significant environmental predictor at some level for all outcome measures. Other factors of importance across several outcome measures are factor 8, covering good paths and cycleways (including ‘paths to the local open space are easy and enjoyable to walk on’, ‘it is easy for me to cycle on my street’, and enjoying ‘watching children play in the street’) and factor 7, covering ease of getting out and about (including ‘It is easy for me to be physically active living on this street’ and ‘it is easy to get to the local open space using public transport’).
Longitudinal cohort
Participants in the intervention group perceived that they were more active postintervention than 2 years previously, significantly more so than those in the comparison group (p=0.04) (differences based on t-test). Responses to the statement ‘it is easy for me to walk on my street’ also showed an increase in the intervention group, a change that was significant compared with the comparison group (p=0.03). However, self-reported levels of outdoor activity in summer did not increase significantly for either group.
Change in factor 5 (contact with nature, natural features and growing things) was significantly different between the comparison and intervention group (p=0.02), with an increase in the comparison group compared with the intervention.
There were some common trends across the two groups, whether the intervention or comparison group: a decline in CASP-19 (p=0.04) and an increase in the number of unhealthy days (p=0.006). However, perceptions that ‘the paths to get to the local open space are easy to walk on’ (p=0.02), ‘there is an attractive fountain or water feature in the local open space’ (p=0.05) and factor 7 (easy to get out and about; p=0.01), increased significantly across both groups in the cohort.
Activity survey
The baseline survey data show that maximum activity levels among participants were recorded between 10:00 and 13:00, when the mean level of any activity above sedentary was 20 min/h (SD 14). However, most activity recorded was in the low-light category, with a mean of 17 min/h (SD 10.27) of light activity (the maximum level for any hour of the day) between 12:00 noon and 13:00. The peak in moderate-to-vigorous activity was a mean of 3.5 min/h (SD 4.06), occurring between 10:00 and 15:00; short bouts of 1 or 2 min/h gave rise to a mean accumulated total of 11 min (SD 3.7) of moderate-to-vigorous activity over the course of the day (between 8:00 and 19:00; see figure 2).
Figure 2.
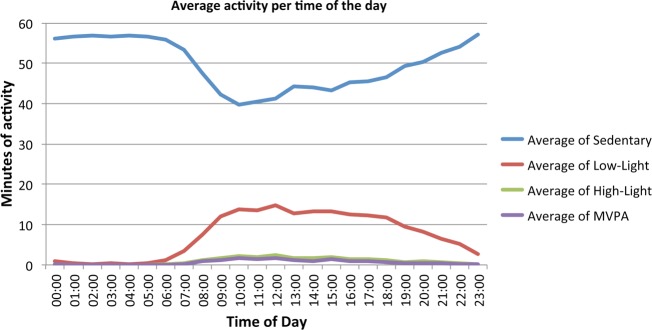
Average daily activity levels of participants in 2008 (n=50).
A typical diary entry suggests that the times of greatest intensity of activity are the moments of going out of the house or returning home, whatever the purpose of the trip. The data indicate that going for a walk was the principal outdoor activity for participants, with visiting the shops second most frequent, followed by sitting outdoors or going to the doctor. Participants went out every 2 days, on average, but only went walking on fewer than 3 days/week.
Discussion
Our study makes a new contribution through the use of a longitudinal, preintervention and postintervention design to look at the influence of change in microscale urban residential street environments on older people's quality of life. We worked with Sustrans to evaluate outcomes from their ‘DIY Streets’ pilot programme, engaging with communities, many of which suffer considerable deprivation, across the UK. We explored the quality of the outdoor built environment in relation to older people's wellbeing and outdoor activities,
Many of the findings reinforce those of Sugiyama and Ward Thompson.23 24 They underline the importance of footways that are attractive and easy to use to access local open space as factors in remaining active into old age and influencing overall quality of life. They also suggest that access to these features in the wider neighbourhood environment may be as important as the local street quality in terms of wellbeing.
When we considered the factors that best predict health and quality of life in our cross-sectional surveys, we found that a lack of barriers and perceived nuisances, as well as good paths and cycleways and enjoyable routes to local open space are consistently associated with time outdoors and with general health and wellbeing. Summer outdoor activity and time outdoors is predicted by having a clean and nuisance-free local park and attractive routes to it, as well as other natural environments nearby. These support findings from a study on utilitarian walking in the Netherlands, which found changes in level and litter on the streets as barriers and good pavements and front gardens as supportive of older adults’ walking25 but, unlike this study, we found parks a significant support for outdoor activity. Our findings support a recent systematic review on physical environment and older adults’ physical activity, which found that the perceived number of recreational facilities and high-quality paths to these facilities was positively related to total and recreational walking,10 and a mixed-method study on neighbourhood activity in UK older adults which found similar physical environment barriers (eg, steep hills) and facilitators (eg, attractive local environment, accessible green space) to those in our study.33
Interestingly, being able to park one's car outside the house was also found to be a predictor of time spent outdoors in our cross-sectional study. Other UK studies have shown that access to a car is a predictor of activity levels and the number of outdoor trips taken may be highest among car owners or users,33 34 reinforcing the importance of car-based mobility for older people.35 36
Our cohort study found that participants in the intervention group perceived it was easier to walk on their street, and that they were more active, postintervention, yet their self report levels of activity did not increase over time. This may reflect a more positive outlook on the local environment as a result of participants seeing investment in their community, but a failure to sustain any temporary increase in activity levels.37 The overall decline in health and wellbeing found across both groups in the cohort may reflect their ageing over 2–3 years and the environmental intervention did not appear to moderate this, perhaps because no behaviour change was discernible at the time of the postintervention survey.
Social interaction has been found to have high impact as a facilitator of neighbourhood activity in UK older adults.33 Our participants did not report a perceived change in social links in the neighbourhood in either our cross-sectional or our cohort studies. However, the perception of cross-sectional study participants that safety for walking after dark had improved postintervention, despite the fact that there were no reported improvements to street lighting as part of interventions, suggests that interpersonal social factors may have played a part in this enhancement. The community engagement activities that form part of the Sustrans ‘DIY Streets’ programme will have involved some social interaction, which may have contributed indirectly to enhanced perceptions of safety.
In our activity study, most participants did not achieve current UK-recommended levels for moderate-or-vigorous physical activity in older adults.2 These recommend that activity over a week should add up to at least 150 min of moderate intensity activity in bouts of 10 min or more. Our participants were most active between 10:00 and 13:00 but they rarely achieved more than 4 min of moderate-to-vigorous activity in any 1 h, with a mean weekly total of 105 min. Such patterns are confirmed by another recent UK study.38 These are disturbing findings in the light of evidence on the importance of physical activity as protective of physical, neurological and psychological health into old age.1 5 39
Walking was by far the most frequent outdoor activity noted by participants but getting out of the house at all, for whatever reason, even if people use a car or public transport, seems to be associated with greater levels of activity. Again, this supports other recent UK findings that ‘trips away from the home are associated with objectively measured physical activity, both as volume of MVPA, and steps per day’.34 Further, future analysis of the longitudinal accelerometer data, although limited in power, may help understand better the links in our study between environmental change and activity.
Limitations
Our study has a number of limitations. The availability of only seven of the original nine sites, postintervention, resulted in smaller sample sizes for both cross-sectional and cohort data collection. Our longitudinal cohort was further reduced due to some participants no longer living on the street and due to dissatisfaction with interventions in one location in particular. In addition, our recruitment and retention of participants for the activity study was limited, possibly because the burden of participation was considered too high, especially for an older population in often deprived circumstances.
Conclusion
In summary, the ‘DIY Street’ environmental changes appear to have had an impact on older adults’ perceptions of street walkability and safety at night, if not on overall levels of physical activity or wellbeing. Such responses may reflect participants’ openness to behaviour change in activity levels that has yet to be planned or enacted.37 Our study found that environmental changes of the sort used in DIY Streets projects are not sufficient on their own to support behaviour change, at least within a 3-to-6-month timeframe after the intervention. Changes to the street environment may have had a negative effect on older people's outdoor patterns of use, or perceptions of outdoor accessibility, if they could no longer easily park their car outside the house and their car is a major mode of transport for outdoor trips.
The WHO recommends better design of the built environment to create age-friendly cities that support public health into old age.40 We provide an example of a knowledge exchange product that we have used for dissemination to policy-makers and other research end-users as part of the wider, I'DGO project (http://www.idgo.ac.uk), of which this study forms a part. Urban planners, engineers and landscape designers need to reconcile good environmental design with requirements for public health and this leaflet highlight key messages from the study to assist in evidence-based practice. Such messages include noting that ‘the pedestrian experience is vitally important to older people’ and that ‘for the many who find it difficult to get around, it is often due to the poor design, provision, installation or upkeep of neighbourhood features, especially footways’. Results such as those of our study need to be considered within a wider framework of built environment planning, design and management, perhaps based on systems theory.41 Nonetheless, they point to certain factors in the design and management of the built and natural environment that may be important in supporting active ageing and the design of age-friendly environments.40
Acknowledgments
This study was part of the I'DGO TOO (Inclusive Design for Getting Outdoors 2) OPENspace project. The I'DGO consortium is led by OPENspace at Edinburgh College of Art, University of Edinburgh and Heriot-Watt University, with partners in Salford and Warwick Universities. We are grateful for the support of Sustrans and I'DGO partners in this project.
Footnotes
Contributors: This paper was drafted by CWT, who leads the I'DGO TOO study on which it reports; she was responsible for the study design and PA was responsible for the data analysis strategy. AC, SA and AZ, as Research Associates on the project, were responsible for the data collection and undertaking analysis of results. SA managed the data collection and preliminary analysis, AC undertook the questionnaire survey analysis, AZ undertook the accelerometry analysis. All authors have contributed to the final version of the paper, for which CWT takes overall responsibility as the guarantor.
Funding: Funding for this project was provided by the UK Engineering and Physical Sciences Research Council under grant no. EP/D079861/1.
Competing interests: None.
Ethics approval : Edinburgh College of Art.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Hallal PC, Bauman AE, Heath GW, et al. Physical activity: more of the same is not enough. Lancet 2012;380:190–1 [DOI] [PubMed] [Google Scholar]
- 2.Department of Health, Physical Activity, Health Improvement and Protection. Start active, stay active: a report on physical activity from the four home countries’ Chief Medical Officers. London: Department of Health, 2011 [Google Scholar]
- 3.British Heart Foundation National Centre (BHFNC) for Physical Activity and Health. Fact sheet: current levels of physical activity in older adults.. BHFNC, Loughborough University, 2012, http://www.bhfactive.org.uk (accessed 24 Oct 2012) [Google Scholar]
- 4.British Heart Foundation National Centre (BHFNC) for Physical Activity and Health. Evidence briefing: physical activity for older adults (65+years). BHFNC, Loughborough University, 2012, http://www.bhfactive.org.uk (accessed 24 Oct 2012). [Google Scholar]
- 5.Gow AJ, Bastin ME, Muñoz Maniega S, et al. Neuroprotective lifestyles and the aging brain: activity, atrophy, and white matter integrity. Neurology 2012;79:1802. [DOI] [PubMed] [Google Scholar]
- 6.Sorkin D, Rook KS, Lu JL. Loneliness, lack of emotional support, lack of companionship, and the likelihood of having a heart condition in an elderly sample. Ann Behav Med 2002;24:290–8 [DOI] [PubMed] [Google Scholar]
- 7.Das P, Horton R. Rethinking our approach to physical activity. Lancet 2012;380:189–90 [DOI] [PubMed] [Google Scholar]
- 8.Frank LD, McKay HA. Time to walk the talk: embracing the built environment to promote physical mobility. Br J Sports Med 2010;44:615 [Google Scholar]
- 9.Murray A. Physical inactivity—getting Scotland on the move. Br J Sports Med 2013;47:191–2 [DOI] [PubMed] [Google Scholar]
- 10.Van Cauwenberg J, De Bourdeaudhuij I, De Meester F, et al. Relationship between the physical environment and physical activity in older adults: a systematic review. Health Place 2011;17:458–69 [DOI] [PubMed] [Google Scholar]
- 11.Global Advocacy for Physical Activity (GAPA) the Advocacy Council of the International Society for Physical Activity and Health (ISPAH). NCD prevention: investments that work for physical activity . Br J Sports Med 2012;46:704–7 [DOI] [PubMed] [Google Scholar]
- 12.Scottish Government. Good places, better health. a new approach to environment and health in Scotland: implementation plan. Edinburgh: Scottish Government, 2008 [Google Scholar]
- 13.Sallis JF. Measuring physical activity environments: a brief history. Am J Prev Med 2009;36:86–92 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Millington C, Ward Thompson C, Rowe D, et al. Development of the Scottish Walkability Assessment Tool (SWAT). Health Place 2009;15:474–81 [DOI] [PubMed] [Google Scholar]
- 15.Bull F, Giles-Corti B, Wood L. Active landscapes: the methodological challenges in developing the evidence on urban environments and physical activity. In: Ward Thompson C, Aspinall P, Bell S. eds. Innovative approaches to researching landscape and health: open space: people space 2. Abingdon: Routledge, 2010:96–116 [Google Scholar]
- 16.Barton H, Grant M. A health map for the local human habitat. J R Soc Promot Health 2006;126:252–3 [DOI] [PubMed] [Google Scholar]
- 17.Frank LD, Sallis JF, Saelens BE, et al. The development of a walkability index: application to the Neighborhood Quality of Life Study. Br J Sports Med 2010;44:924–33 [DOI] [PubMed] [Google Scholar]
- 18.Lawton MP. Environment and aging. Los Angeles: Brooks/Cole, 1980 [Google Scholar]
- 19.Kahana EA. congruence model of person-environment interaction. In: Lawton MP, Windley PG, Byerts TO. eds. Aging and the environment: theoretical approaches. New York: Springer, 1982:97–121 [Google Scholar]
- 20.Carp FM, Carp A. A complementary/congruence model of well-being or mental health for the community elderly. In: Altman I, Lawton MP, Wohlwill JF. eds. Elderly people and the environment. Palo Alto, CA: Plenum, 1984:279–336 [Google Scholar]
- 21.Iwarsson SA. Long-term perspective on person-environment fit and ADL dependence among older Swedish adults. Gerontologist 2005;45:327–36 [DOI] [PubMed] [Google Scholar]
- 22.Sugiyama T, Ward Thompson C. Measuring the quality of the outdoor environment relevant to older people's lives. In: Ward Thompson C, Travlou P. eds, Open space: people space. Abingdon, UK: Taylor and Francis, 2007:153–62 [Google Scholar]
- 23.Sugiyama T, Ward Thompson C. Older people's health, outdoor activity and supportiveness of neighbourhood environments. Landscape Urban Plan 2007;83:168–75 [Google Scholar]
- 24.Sugiyama T, Ward Thompson C. Associations between characteristics of neighbourhood open space and older people's walking. Urban For Urban Greening 2008;7:41–51 [Google Scholar]
- 25.Borst HC, de Vries SI, Graham JMA, et al. Influence of environmental street characteristics on walking route choice of elderly people. J Environ Psychol 2009;9:477–84 [Google Scholar]
- 26. Indices of Deprivation are combined measures of local area economic, social and environmental deprivation, defined in similar but distinct ways by the governments of England ( http://www.communities.gov.uk/publications/communities/indiciesdeprivation07), Wales ( http://wales.gov.uk/topics/statistics/theme/wimd) and Scotland ( http://www.scotland.gov.uk/topics/Statistics/SIMD) (accesses 3Nov 2012)
- 27.EuroQol Group. EQ-5D Health Questionnaire. 1990. http://www.euroqol.org (accessed 29 Apr 2011).
- 28.Hyde M, Wiggins RD, Higgs P, et al. A measure of quality of life in early old age: the theory, development and properties of a needs satisfaction model (CASP-19). Aging Mental Health 2003;7:186–94 [DOI] [PubMed] [Google Scholar]
- 29.Jette M, Davies AR, Cleary PD, et al. The functional status questionnaire: reliability and validity when used in primary care. J Gen Intern Med 1986;1:143–9 [DOI] [PubMed] [Google Scholar]
- 30.Freedson PS, Melanson E, Sirard J. Calibration of the computer science and applications, Inc. accelerometer . Med Sci Sports Exerc 1998;30:777–81 [DOI] [PubMed] [Google Scholar]
- 31.Copeland J, Eslinger D. Accelerometer assessment of physical activity in active, healthy, older adults. J Aging Phys Act 2009;17:17–30 [DOI] [PubMed] [Google Scholar]
- 32.Buman MP, Hekler EB, Haskell WL, et al. Objective lght-intensity physical activity associations with rated health in older adults. Am J Epidemiol 2010;172:1155–65 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Stathi AS, Gilbert H, Coulson JC, et al. Determinants of neighborhood activity of adults aged 70 and over: a mixed methods study. J Aging Phys Act 2012;20:148–70 [DOI] [PubMed] [Google Scholar]
- 34.Davis MG, Fox KR, Hillsdon M, et al. Getting out and about in older adults: the nature of daily trips and their association with objectively assessed physical activity. Int J Behav Nutr Phys Act, 2011;8:116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Schwanen T, Ziegler F. Wellbeing, independence and mobility: an introduction. Ageing Soc 2011;31:719–33 [Google Scholar]
- 36.Mollenkopf H, Hieber A, Wahl H-W. Continuity and change in older adults’ perceptions of out-of-home mobility over ten years: a qualitative-quantitative approach. Ageing Soc 2011;31:782–802 [Google Scholar]
- 37.Marcus BH, Simkin LR. The transtheoretical model: applications to exercise behavior. Med Sci Sports Exerc 1994;26:1400–4 [PubMed] [Google Scholar]
- 38.Davis MG, Fox KR, Hillsdon M, et al. Objectively measured physical activity in a diverse sample of older urban UK adults. Med Sci Sports Exerc 2011;43:647–54 [DOI] [PubMed] [Google Scholar]
- 39.Lee I-M, Shiroma EJ, Lobelo F, et al. for the Lancet Physical Activity Series Working Group. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy . Lancet 2012;380:219–29 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.World Health Organisation. Global age-friendly cities: a guide. Geneva: WHO Press, 2007 [Google Scholar]
- 41.Giles-Corti B, King AC. Creating active environments across the life course: ‘thinking outside the square’. Br J Sports Med 2009;43:109–13 [DOI] [PubMed] [Google Scholar]