

Abstract
[Purpose] The aim of this paper was to report the efficacy of kinesiology taping for recovery from wrist pain and limited range of motion (ROM) in a physical therapist with repetitive strain injuries. [Subjects] A 32 year-old male physical therapist developed recurring severe pain in the dominant wrist and limited active ROM with extremely painful supination. [Methods] The kinesiology tape was applied to the lumbricals, musculi interossei dorsales, palmares, the wrist extensor and flexor muscles, and the wrist joint for 3 weeks for an average of 10 h/day. [Results] After application of the kinesiology tape, the Numeric Pain Rating Scale and Patient-rated Wrist Evaluation scores decreased, and the Patient-Specific Functional Scale score increased in comparison with the initial score. [Conclusion] Repeated kinesiology taping of the wrist muscles and joint could be an effective method for recovery from occupational wrist disorders experienced by physical therapists.
Key words: Occupational wrist pain, Kinesiology tape, Work-related musculoskeletal disorders
INTRODUCTION
Physical therapy practice is associated with an increased risk of the development of work-related musculoskeletal disorders (WMSDs)1) because physical therapists engage in manual therapy, twisting, bending, reaching, and lifting and maintain awkward positions for prolonged periods of time while tending to patients2, 3). Grooten et al.4) reported that more than half of the physical therapists employed for their study experienced discomfort or pain in the hand/wrist area (58.5%). Previous studies have shown that manual traction, joint mobilization, or performance of orthopaedic manual therapy techniques, alone or in combination, is related to an increased prevalence of WMSDs affecting the hand/wrist region3, 5). Even though studies have frequently reported the prevalence of WMSDs in physical therapists1,2,3, 5), no study has been carried out to evaluate the appropriate treatment for occupational wrist pain experienced by physical therapists. In this report, we describe the efficacy of kinesiology taping of the wrist muscles and joint for recovery from occupational wrist pain that developed in a physical therapist.
CASE DESCRIPTION
A 32-year-old male physical therapist developed recurring severe pain in the dominant (right) wrist and limited active range of motion (ROM) with extremely painful supination. He described the pain as a constant “achy” and occasionally “sharp” sensation that varied in intensity depending on his wrist activities. He complained that all his repetitive occupational activities, such as joint mobilization and manual traction in patients with musculoskeletal disorders, neurodevelopmental treatment in patients with stroke, and transferring of patients, aggravated his wrist pain and limited ROM. He was diagnosed with repetitive strain injuries and received a prescription for rest and a wrist brace. However, he could not suspend his wrist movement because of the many patients in his charge. In addition, keeping the brace on to immobilize his wrist made it difficult to perform physical therapy. The subject signed an informed consent document that was approved by the Ethics Committee of Dong-Eui University, in accordance with the ethical standards of the Declaration of Helsinki.
He had a Numeric Pain Rating Scale (NPRS) score (0, no pain; 10, the worst imaginable pain) of 7/10 for the wrist area. The wrist and forearm ROMs were measured by using a goniometer. The following ROMs were documented during the initial assessment: wrist flexion of 58° (normal range, 0–80°)6), extension of 38° (normal range, 0–80°)6), radial deviation of 8° (normal range, 0–20°)6), ulnar deviation of 25° (normal range, 0–30°)6), pronation of 68° (normal range, 0–80°)6), and supination of 46° (normal range, 0–80°)6).
The pain subset score derived from the Patient-rated Wrist Evaluation (PRWE) (0, no difficulty; 10, unable to perform the activity), which is a validated instrument used for assessing wrist pain and functional disability while performing activities of daily living7), was 38/50, and the function subset score was 55/100 (specific function activities, 31/50; usual function activities, 24/50). The total baseline score obtained with the Patient-Specific Functional Scale (PSFS) (0, unable to perform the activity; 10, able to perform the activity), which is another validated instrument used for measuring functional status associated with a patient’s condition8), was 20/50 (Table 1).
Table 1. . Outcomes of the patient-specific functional scale.
| Assessment | Baseline score | Final score |
| PSFS (score) | 20/50 | 45/50 |
| Activity 1 (turn a door knob) | 6/10 | 9/10 |
| Activity 2 (manual traction) | 3/10 | 8/10 |
| Activity 3 (joint mobilization) | 3/10 | 9/10 |
| Activity 4 (transfer stroke patient) | 3/10 | 9/10 |
| Activity 5 (neurodevelopmental treatment) | 5/10 | 9/10 |
PSFS, Patient-Specific Functional Scale
METHODS
We applied kinesiology tape (BB Tape, WETAPE Inc, Seoul, Korea) with 30–40% stretch on the wrist muscle and joint for an average of 12 h/day for 7 days. The kinesiology tape was applied on the flexors of the right wrist from the medial epicondyle to the wrist joint on the palmar side when the wrist was in the extension position (Fig. 1A). For the lumbricals, musculi interossei dorsales, and palmares, the tape was cut in half and was applied from the region between the fingers to both wrist joint while the fingers were spread apart (Fig. 1B and 1C). For the wrist extensors, the tape was applied from the lateral epicondyle to the wrist joint on the dorsal side while the wrist was flexed (Fig. 1C). For the forearm pronation (to limit painful supination), the tape was applied with 40–50% stretch from the styloid process of the ulnar and was internally rotated around the wrist joint 2–3 times while the wrist was in a pronated position (Fig. 1D).
Fig. 1.
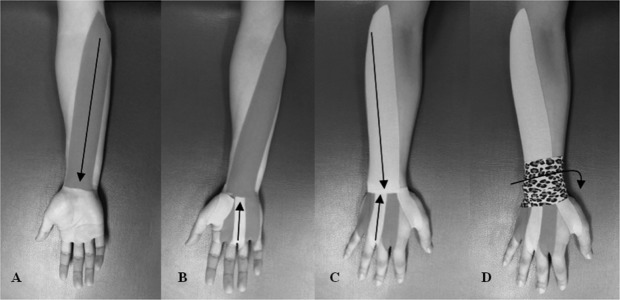
Kinesiology tape application for the wrist flexor (A), lumbricals, musculi interossei dorsales and palmares (B), extensor (C) muscles, and pronation (D).
RESULTS
As shown in Table 1, after kinesiology taping, the NPRS scores decreased and the wrist and forearm ROMs increased. During the taping intervention, the patient could perform occupational wrist activities more easily than he could with a brace on. By the final assessment, the NPRS score had decreased to 0/10; the pain subset score of the PRWE had decreased to 5/50; the function subset score of the PRWE had decreased to 2/100 (specific function activities, 1/50; usual function activities, 1/50); the PSFS score had increased to 45/50 (Table 1); and wrist flexion had increased to 78°, extension had increased to 73°, radial deviation had increased to 20°, ulnar deviation had increased to 30°, pronation had increased to 78°, and supination had increased to 77°. The pain had resolved, and he was able to perform physical therapy involving repetitive wrist activity without any pain or limited ROM in his wrist.
DISCUSSION
Repetitive strain injuries in the wrist may be caused by repetitive tasks, vibrations, forceful exertions, or mechanical compression during repetitive wrist activity9). The repetitive wrist activity required to perform physical therapy, such as manual traction, joint mobilization, and neurodevelopmental treatment, may cause excessive stress on muscles, tendons, ligaments, and nerves in the wrist.
Skin deformation caused by application of kinesiology tape stimulates cutaneous mechanoreceptors10). According to the counterirritant theory, the excitement of mechanoreceptive afferents induces the release of enkephalin (i.e., inhibition of the neurotransmitter involved in the integration of pain [substance P] and hyperpolarization of interneurons), which results in inhibition of the transmission of nociceptive signals11). Therefore, we assume that the elasticity of kinesiology tape is effective in relieving occupational wrist pain.
The elasticity of kinesiology tape allows free ROM within the range of its elasticity and controls joint instability12). Therefore, wrist activity with kinesiology tape may provide support to an injured wrist joint and could be easier for the patient compared with keeping a brace on. In addition, kinesiology tape is stretched and under increased tension during wrist activity, which forces the wrist to return to forearm pronation. Therefore, painful supination is avoided by the flexibility of the tape, and the natural healing process is assisted.
Although the effects of kinesiology taping, such as increased muscle strength and activity, are still controversial, from the findings of a few previous studies, it is assumed that kinesiology taping at the calves may improve the functioning of the medial gastrocnemius and thus, enhance vertical jumping13) and posture balance14). Therefore, kinesiology taping may improve the functioning of the wrist extensor and flexor muscles and reduce wrist pain, which can be estimated based on the gradual increase in wrist and forearm ROMs and the PSFS score and the gradual decrease in the PRWE score. However, the mechanisms underlying the effects of kinesiology taping on muscle function cannot be confirmed on the basis of our findings, and further investigations should be carried out.
REFERENCES
- 1.Campo M, Weiser S, Koenig KL, et al. : Work-related musculoskeletal disorders in physical therapists: a prospective cohort study with 1-year follow-up. Phys Ther, 2008, 88: 608–619 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Holder NL, Clark HA, DiBlasio JM, et al. : Cause, prevalence, and response to occupational musculoskeletal injuries reported by physical therapists and physical therapist assistants. Phys Ther, 1999, 79: 642–652 [DOI] [PubMed] [Google Scholar]
- 3.Bork BE, Cook TM, Rosecrance JC, et al. : Work-related musculoskeletal disorders among physical therapists. Phys Ther, 1996, 76: 827–835 [DOI] [PubMed] [Google Scholar]
- 4.Grooten WJ, Wernstedt P, Campo M: Work-related musculoskeletal disorders in female Swedish physical therapists with more than 15 years of job experience: prevalence and associations with work exposures. Physiother Theory Pract, 2011, 27: 213–222 [DOI] [PubMed] [Google Scholar]
- 5.Glover W, McGregor A, Sullivan C, et al. : Work-related musculoskeletal disorders affecting members of the Chartered Society of Physiotherapy. Physiotherapy, 2005, 91: 138–147 [Google Scholar]
- 6.Green WB, Heckman JD: The clinical measurement of joint motion. Rosemont: Americal academy of orthopaedic surgeons, 1994
- 7.MacDermid JC, Turgeon T, Richards RS, et al. : Patient rating of wrist pain and disability: a reliable and valid measurement tool. J Orthop Trauma, 1998, 12: 577–586 [DOI] [PubMed] [Google Scholar]
- 8.Stratford P, Gill C, Westaway M, et al. : Assessing disability and change on individual patients: a report of a patient specific measure. Physiother Can, 1995, 47: 258–263 [Google Scholar]
- 9.van Tulder M, Malmivaara A, Koes B: Repetitive strain injury. Lancet, 2007, 369: 1815–1822 [DOI] [PubMed] [Google Scholar]
- 10.Yamashiro K, Sato D, Yoshida T, et al. : The effect of taping along forearm on long-latency somatosensory evoked potentials (SEPs): an ERP study. Br J Sports Med, 2011, 45: A9 [Google Scholar]
- 11.Lundy-Ekman L: Neuroscience fundamentals for rehabilitation, 3rd ed. St. Louis: Saunders Elsevier, 2007 [Google Scholar]
- 12.Jaraczewska E, Long C: Kinesio taping in stroke: improving functional use of the upper extremity in hemiplegia. Top Stroke Rehabil, 2006, 13: 31–42 [DOI] [PubMed] [Google Scholar]
- 13.Huang CY, Hsieh TH, Lu SC, et al. : Effect of the Kinesio tape to muscle activity and vertical jump performance in healthy inactive people. Biomed Eng Online, 2011, 10: 70 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Cortesi M, Cattaneo D, Jonsdottir J: Effect of kinesio taping on standing balance in subjects with multiple sclerosis: A pilot study1. NeuroRehabilitation, 2011, 28: 365–372 [DOI] [PubMed] [Google Scholar]