

Abstract
Imaging with positron emission tomography (PET) and 68Ga-DOTA peptides is a promising method in intracranial meningiomas. Especially in recurrent meningioma discrimination between scar tissue and recurrent tumor tissue in magnetic resonance imaging (MRI) is often difficult. We report the first case of 68Ga-DOTATATE-PET/computed tomography (PET/CT) imaging in recurrent spinal meningioma. A 64-year-old Caucasian female patient was referred to our department with the second recurrence of thoracic meningothelial meningioma. In MRI, it remained unclear if the multiple enhancements seen represented scar tissue or vital tumor. We offered 68Ga-DOTATATE-PET/CT imaging in order to evaluate the best strategy. 68Ga-DOTATATE-PET/CT imaging revealed strong tracer uptake in parts of the lesions. The pattern did distinctly differ from MRI enhancement. Multiple biopsies were performed in the PET-positive and PET-negative regions. Histological results confirmed the prediction of 68Ga-DOTATATE-PET with vital tumor in PET-positive regions and scar tissue in PET-negative regions. Differentiating scar tissue from tumor can be challenging in recurrent spinal meningioma with MRI alone. In the presented case, 68Ga-DOTATATE-PET imaging was able to differentiate noninvasively between tumor and scar.
Keywords: DOTATATE-positron emission tomography/computed tomography, meningioma, metabolic imaging, spinal tumor
INTRODUCTION
Imaging of somatostatin receptors with positron emission tomography (PET) and 68Ga-DOTA peptides is a promising method in detection and target volume definition for radiation therapy in intracranial meningiomas.[1,2,3] The superiority of DOTATATOC-PET over conventional contrast-enhanced magnetic resonance imaging (CE-MRI) in cranial meningiomas has been reported recently.[2] Especially in recurrent meningioma where a clear discrimination between scar tissue and recurrent tumor tissue is often difficult, PET with different DOTA peptides may provide additional information.
We report the first case of 68Ga-DOTATATE-PET/computed tomography (CT) imaging in recurrent spinal meningioma.
CASE REPORT
A 64-year-old Caucasian female patient was referred to our department in 2003 with lower limb ataxia and back pain. She completely recovered after resection of a meningothelial meningioma (WHO Grade I) at the level of T4. In 2010 a local recurrence was resected and histology was again meningothelial meningioma (WHO Grade I).
In 2013, the patient presented with a new nodular structure on MRI in the caudal part of the former location lying dorsally at level T4 and T5. Furthermore, an extensive enhancement at levels C6 to T5 ventrally and dorsally of the spinal cord was observed. It was unclear whether this was scar tissue or vital tumor [Figure 1]. At that time, the patient was nearly asymptomatic, but strongly desired surgical treatment in order to prevent a new neurological deficit. We offered 68Ga-DOTATATE-PET/CT imaging in order to evaluate the best strategy and to differentiate actual tumor recurrence from scar tissue. Written informed consent by the patient on usage of medical data and publication was obtained.
Figure 1.
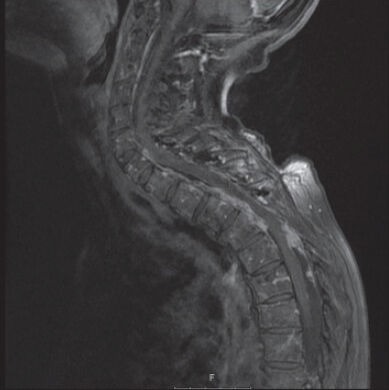
Magnetic resonance imaging, T1 sequences with gadolinium, sagittal view. Imaging after two previous resections. Note strong dorsal (C7/Th1 to Th5) and ventral (C6 to Th3/Th4) enhancement in the spinal canal. Artifacts due to laminoplasty material
RESULTS
68Ga-DOTATATE-positron emission tomography/computed tomography imaging revealed strong tracer uptake in the caudal and dorsal part of the nodular lesion at the level of Th4 + 5. This was interpreted as tumor recurrence. Cranially to this finding (at the level C6-Th4), a divergent tracer pattern was found with a strong tracer uptake in the ventral part and no relevant uptake in the dorsal part. Thus we concluded that there was nonsuspicious tissue dorsally and tumor ventrally [Figures 1 and 2].
Figure 2.
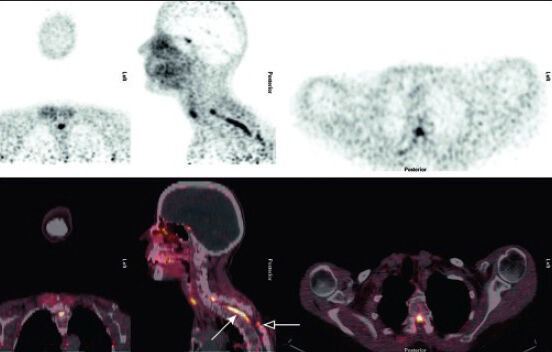
68Ga-DOTATATE-positron emission tomography/computed tomography imaging. Coronal, sagittal and axial views. Images presented a high tracer uptake in the ventral part of the spinal canal esp. at the level C6-Th4 (solid arrow) as well as in the dorsal part at the level Th4 + 5 (hollow arrow) corresponding histological to vital tumor. Note typical intracranial enhancement of the pituitary gland
In this particular case, we considered a dorsal approach for resection of the caudal PET-positive nodules to be the safest and most effective at levels T4 and T5. In addition, multiple biopsies were performed cranially, in the PET-negative, dorsal region, confirming the 68Ga-DOTATATE-PET imaging results (no tumor). When performing biopsies in the ventral portions at the level of C6-Th4, intraoperative neurophysiological monitoring indicated hazard of permanent neurologic deficits. Therefore, surgery was stopped. Postoperatively, no new neurological deficits occurred. The biopsies realized in the PET positive, ventral region between C6 and T4 were positive for tumor, as was the tissue resected dorsally at T4 and T5. Owing to the risks and morbidity a ventral approach was not considered suitable for the patient; she was referred to radiotherapy for local beam irradiation of the tumor bed and the residual solid tumor.
DISCUSSION
Differentiating between scar tissue and local recurrence in meningioma may be challenging especially in small spinal lesions. Hybrid imaging with PET/CT or PET/MR is likely to improve diagnostic yield, which may lead to improved management of disease. Hybrid imaging is helpful for exact anatomic localization of the process and is therefore superior to nonhybrid PET imaging. It allows for planning of surgery and radiotherapy. The spatial resolution of PET is limited (7-8 mm full width at half maximum) but in lesions with high lesion to background contrast even smaller lesions may be detected.
The application of PET imaging in cerebral meningiomas using different tracers is currently under clinical investigation.[4] Beside somatostatin receptor ligands the application of radiolabelled amino acids presents an interesting option. To the best of our knowledge, only one case of 68Ga-DOTATATE uptake in a spinal meningioma has been reported so far.[5] In that case,68Ga-DOATATE uptake was noted in a spinal meningioma of a patient suffering from insulinoma. In that case, unspecific uptake of 68Ga-DOTATATE was observed in a degenerative lesion, which characterizes a potential pitfall in such investigations. In the present case report, CT and MRI failed to differentiate recurrent tumor from scar tissue, while 68Ga-DOTATATE-PET/CT detected recurrent tumor with high lesion to background contrast as confirmed by biopsy. Since conventional imaging techniques did not prove helpful in differentiating tumor tissue from scar tissue, 68Ga-DOTATATE-PET/CT imaging in this case allowed for optimal planning and a safe approach to the pathology discussed herein. The spatial resolution of 68Ga-DOTATATE-PET/CT appeared to be sufficient for precise surgical planning due to high lesion to background contrast. A larger study should be initiated in order to confirm these preliminary results.
CONCLUSION
Differentiating scar tissue from tumor may be challenging in recurrent spinal meningioma with MRI alone. In the presented case, 68Ga-DOTATATE-PET imaging was able to differentiate noninvasively between tumor and scar. This was confirmed histologically.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Henze M, Schuhmacher J, Hipp P, Kowalski J, Becker DW, Doll J, et al. PET imaging of somatostatin receptors using [68GA-DOTA-D-Phe1-Tyr3-octreotide: First results in patients with meningiomas. J Nucl Med. 2001;42:1053–6. [PubMed] [Google Scholar]
- 2.Afshar-Oromieh A, Giesel FL, Linhart HG, Haberkorn U, Haufe S, Combs SE, et al. Detection of cranial meningiomas: Comparison of 68Ga-DOTATOC PET/CT and contrast-enhanced MRI. Eur J Nucl Med Mol Imaging. 2012;39:1409–15. doi: 10.1007/s00259-012-2155-3. [DOI] [PubMed] [Google Scholar]
- 3.Graf R, Nyuyki F, Steffen IG, Michel R, Fahdt D, Wust P, et al. Contribution of 68Ga-DOTATOC-PET/CT to target volume delineation of skull base meningiomas treated with stereotactic radiation therapy. Int J Radiat Oncol Biol Phys. 2013;85:68–73. doi: 10.1016/j.ijrobp.2012.03.021. [DOI] [PubMed] [Google Scholar]
- 4.Cornelius JF, Langen KJ, Stoffels G, Hänggi D, Sabel M, Jakob Steiger H. Positron emission tomography imaging of meningioma in clinical practice: Review of literature and future directions. Neurosurgery. 2012;70:1033–41. doi: 10.1227/NEU.0b013e31823bcd87. [DOI] [PubMed] [Google Scholar]
- 5.Klinaki I, Al-Nahhas A, Soneji N, Win Z. 68Ga-DOTATATE-PET/CT uptake in spinal lesions and MRI correlation on a patient with neuroendocrine tumor: Potential pitfalls. Clin Nucl Med. 2013;38:e449–53. doi: 10.1097/RLU.0b013e31827a2325. [DOI] [PubMed] [Google Scholar]