

Abstract
Objective: To identify avoidable factors contributing to neonatal morbidity and mortality due to “birth asphyxia” and to ascertain if hypoxic ischemic encephalopathy (HIE) alone could act as a good marker for avoidable factors associated with “birth asphyxia”.
Setting: Kalafong Hospital, South Africa, a regional hospital unit that caters for mainly indigent urban population but also receives referrals from the Mpumalanga Province.
Methods: All neonates and intrapartum stillbirths fulfilling the criteria of birth asphyxia born at the Kalafong Hospital during 2008 and 2009 were included. Neonates born at less than 34 weeks gestation, born with infection, major congenital malformations or inborn errors of metabolism and intrapartum deaths due to abruption placentae were excluded. Neonates referred from Level 1 clinics postnatally, who qualified with these criteria, were also included in the study. The files were retrieved, and avoidable factors were identified. Avoidable factors were classified into 3 groups: patient associated, administrative and medical personnel associated problems.
Results: In 2008 and 2009, 10117 babies were born at Kalafong Hospital. 224 babies with intrapartum related asphyxia were identified (22.1/1000 births). This group consisted of 14 intrapartum stillbirths, 85 neonates with mild asphyxia, 125 babies with severe asphyxia of which 41 had a neonatal near miss markers without HIE and 84 with HIE. Fifteen of the babies with HIE subsequently died. The number of avoidable factors identified per case file reviewed increased with the severity of the hypoxic event, mild asphyxia 0.74, neonatal near miss without HIE 0.85, HIE survivor 0.91, and stillbirth or neonatal death 1.29. Major avoidable factors for birth asphyxia were refusal of medical treatment, inadequate facilities, no detection of or reaction to fetal distress, and incorrect management of second stage. The avoidable factors detected in neonates with HIE were the same as those detected in the whole group.
Conclusion: The avoidable factors described in a confidential enquiry concentrating on the labour management of women delivering neonates with all grades of “birth asphyxia” were similar to those found in women delivering neonates with HIE. HIE in neonates is a clearly defined condition, making it a good marker to use to review the quality of intrapartum care received by the women who delivered neonates with HIE.
Keywords: Birth Asphyxia, Hypoxic Ischaemic Encephalopathy, Audit, Intrapartum Care, Quality of Care
Introduction
Over 900000 newborns each year die from labour-related causes. This makes intrapartum hypoxia or asphyxia the third most common cause of newborn death (23%) after infections (36%) and preterm birth (28%) (Lawn et al., 2005). Another 1.1 million babies die during labour and are stillborn. Intrapartum hypoxia is the most frequent mechanism of damage in these stillbirths, with the majority of deaths being at term in otherwise uncomplicated pregnancies (CEMACH, 2008). Not surprisingly, a large proportion of these events are considered avoidable (Buchmann et al., 2002; Velaphi and Pattinson, 2005) and audit of such perinatal deaths to ascertain the quality of care provided for the women in labour therefore seems essential (Lawn et al., 2005: Ward et al., 1995).
The majority of women losing babies to intrapartum hypoxia are women considered at low risk and with apparently normal labours. Buchmann and Pattinson (2005) showed that there were signs of probable fetal distress in 80% of intrapartum hypoxia cases (late decelerations and/or thick meconium stained liquor) yet only 25% had an operative delivery due to fetal distress. This demonstrates there is often not an adequate response to abnormal signs in labour. The core problems have been found to be: inadequate clinical skills; poor recording of clinical findings, which lead to substandard (or no) management decisions; andlack of transport for women complicating during labour.
Audit of deaths and neonatal near misses (defined as neonates who almost died but survived) may provide information that can improve perinatal care and prevent future deaths (Avenant, 2009). On their own, low Apgar scores, ‘‘fetal distress’’ during labour, metabolic acidosis at birth, and neonatal encephalopathy, do not provide convincing evidence of severe intrapartum hypoxia. The term “birth asphyxia” has been greatly miss-used and it is unclear as to what it actually represents, although most clinicians believe they can identify a case of birth asphyxia. Nelson et al. (2007) defined the term “hypoxic ischemic encephalopathy” as the presence of encephalopathy developing in the first 24 hours after birth and metabolic acidemia associated with evidence of fetal distress and a low Apgar score. Nelson stated that the term ‘‘hypoxic ischemic encephalopathy’’ (HIE) should be reserved for instances where the clinical and laboratory picture fits with that description (Nelson et al., 2007). HIE correctly defined, provides the near miss outcome that best identifies surviving neonates that almost died as a result of intrapartum hypoxia, with or without an antepartum predisposing cause (Buchmann and Velaphi, 2009).
An atmosphere of ‘guilt’ and blame, and in some cases even medico-legal liability often complicates discussion of cases of “birth asphyxia” thus making it difficult to objectively evaluate the cases. Staff involved in the management of babies with birth asphyxia might have the tendency to be deliberately defensive and may avoid open disclosure of events. Therefore, a confidential enquiry process might provide the best mechanism for disclosure in a non-accusatory atmosphere. The United Kingdom’s Confidential Enquiry into Maternal and Child Health (CEMACH) states that ‘‘the primary purpose of a confidential enquiry is to review deaths and other adverse outcomes, seeking to identify avoidable factors and to derive lessons for wider policy and practice” (Pearson, 2008).
In this study, a confidential enquiry was performed to identify avoidable factors, missed opportunities and substandard care in the management of the labour of women who delivered babies diagnosed as having “birth asphyxia” in Kalafong Hospital to identify areas where intrapartum care can be improved. Further cases of HIE were identified to ascertain if the avoidable factors identified in these cases were similar to those occurring in other cases of “birth asphyxia”.
Methods
The study was performed at the Kalafong Hospital of Pretoria, a regional hospital that caters for a mainly indigent urban population but also receives referrals from the Mpumalanga Province. All babies with mild asphyxia, asphyxia with a near miss marker (more severe cases of asphyxia, but no HIE), HIE, and intrapartum stillbirths and neonatal deaths due to intrapartum hypoxia were identified. Neonates born at less than 34 weeks gestation, born with infection, major congenital abnormality or inborn errors of metabolism were excluded. Mild asphyxia was defined as a baby with a low Apgar and/or a low pH that did not require intubation as part of resuscitation but was admitted to the neonatal unit for observation. Criteria described by Avenant (2009) for identifying neonatal near misses were used (Table 1). Neonates considered to be a neonatal near miss due to intrapartum hypoxia were identified from the neonatal near miss database of the Department of Obstetrics and Gynaecology. Intrapartum deaths and neonatal deaths classified as being due to intrapartum hypoxia were also identified using the departmental database. The department identifies and discusses all cases of neonatal mortality and neonatal near misses weekly with paediatricians. Intrapartum deaths are discussed when they occur. The perinatal death data is collected on the Perinatal Problem Identification Programme (PPIP) database (Pattinson 2003a). Neonates referred from Level 1 clinics after birth, who also qualified using these criteria, were also included in the study, using data obtained from the neonatal care unit using their neonatal database, in cooperation with a senior paediatrician. A cross check between the neonatal and obstetric database was performed to ensure all cases were identified. Cases fulfilling the criteria of HIE were identified, all these neonates were by definition also neonatal near misses. The files of the identified cases were retrieved, and AdK reviewed the cases for avoidable factors. Unfortunately in 49 cases (21.9%) cases, the file was not found. Avoidable factors were classified into 3 groups: patient associated, administrative problems, and medical personnel associated and the PPIP definitions for avoidable factors were used (Pattinson 2003a; 2003b).
Table 1. Neonatal near miss markers.
| A. | Respiratory failure/dysfunction: need for intubation and ventilation including nasal CPAP. |
| B. | Cardiac failure/dysfunction: need for adrenalin, other inotropic support or volume expansion. |
| C. | CNS failure/dysfunction: any convulsions or need for therapeutic anticonvulsants. |
| D. | Hypovolaemia: need for blood transfusion or volume expansion. |
| E. | Haematologic failure/dysfunction: need for phototherapy or exchange blood transfusion, need for neupogen to increase white cells. |
| F. | Endocrine failure/dysfunction: need to treat hypoglycaemia (additional glucose). |
| G. | Renal failure/dysfunction: haematuria and/or oliguria, anuria. |
| H. | Immunologic failure/dysfunction (congenital infection): CRP greater than or equal to 10 or a rising CRP. |
| I. | Musculo-skeletal morbidity: any fracture. |
| J. | GIT/Hepatic failure/dysfunction: jaundice, nil per os for more than 24 hours. |
All cases were analysed by a single observer (AdK), no patient identifiers were used in the analysis. The Chi Square test was used for categorical data and Students t test for continuous variables. Neonatal near miss and stillbirth and neonatal death audit is an established practice in the maternity unit. Permission to perform these neonatal audits has been obtained from the Ethics Committee of the Faculty of Health Sciences at the University of Pretoria.
Results
In 2008 and 2009, 10117 babies were born at Kalafong Hospital. There were 224 babies with intrapartum related asphyxia (in all severities) identified (22.1/1000 births). Fourteen were intrapartum stillbirths related to intrapartum asphyxia. The live born group consisted of 85 babies with mild asphyxia, 125 babies with severe asphyxia (12.4/1000 births) comprising 41 babies with asphyxia and a neonatal near miss marker but no HIE, 84 neonates with HIE (8.3/1000 births), of which 15 neonates subsequently died. There were 29 perinatal deaths related to intrapartum asphyxia (2.8/1000 births) (Fig. 1, Table 2).
1. Avoidable factors in women with neonates with “birth asphyxia”.
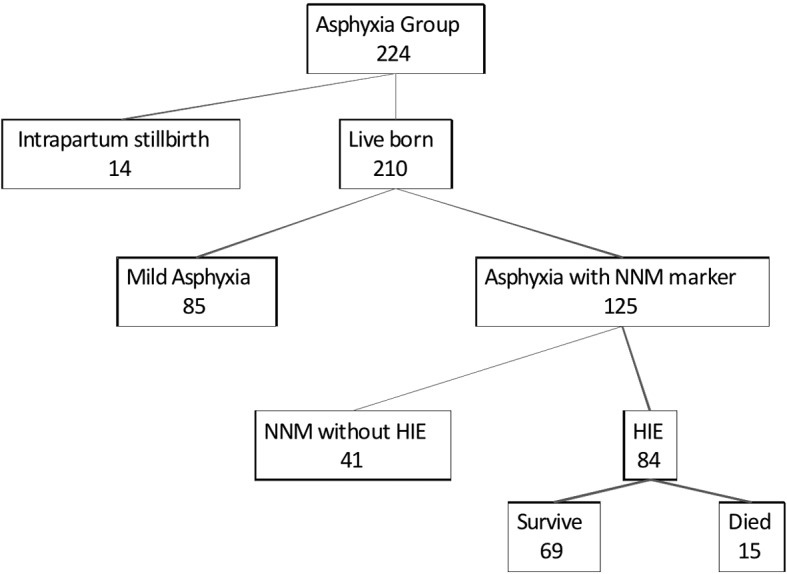
Table 2. Characteristics of the neonates born with “birth asphyxia”.
| Mild Asphyxia (n = 85) | Asphyxia + NNM w/o HIE (n = 41) | HIE but survived (n = 69) | SB (n = 14) and NND (n = 15) | Total Group (n = 224) | |
|---|---|---|---|---|---|
| Mean birth weight (g) | 3010 | 3019 | 3097 | 2846 | 3032 |
| Mean maternal age | 24 | 27 | 25 | 26 | 25 |
| Attended ANC (%) | 98.8 | 92.7 | 100 | 100 | 98.2 |
| Twin pregnancy (%) | 2.4 | 0 | 1.4 | 4.0 | 1.8 |
| RPR pos (%) | 1.2 | 2.4 | 1.4 | 6.1 | 2.7 |
| HIV pos (%) | 24.7 | 26.8 | 18.8 | 28.6 | 24.6 |
| NVD (%) | 45.9 | 46.3 | 58.0 | 53.1 | 48.7 |
| Forceps/vacuum (%) | 15.3 | 7.3 | 14.5 | 6.2 | 12.9 |
| Caesarean-section (%) | 38.8 | 46.3 | 27.5 | 34.7 | 37.1 |
| Number of files reviewed | 67 | 40 | 54 | 14 | 175 |
| Number avoidable factors | 50 | 34 | 49 | 18 (NND 9; SB 9) | 151 |
| Number of avoidable factors per reviewed case | 0.74 | 0.85 | 0.93 | 1.29 | 0.86 |
NNM – Neonatal near miss, HIE – Hypoxic ischemic encephalopathy, SB – Stillbirth, NND – Neonatal death, ANC – Antenatal care, RPR – Rapid Plasma Reagin for syphilis, NVD – normal vaginal delivery.
Another 20 stillbirths due to abruption placentae occurred in this time period but were excluded from the evaluation.
The perinatal deaths tended to have a lower birth weight than the other cases (Table 1). This group also had more HIV infected mothers than the population delivering at Kalafong which has a HIV infection rate of 21.5%. The overall group of infected babies had a higher HIV infection rate than the population delivering at Kalafong Hospital.
No avoidable factors were found in 110 cases of the 175 cases (63%) where the file was reviewed. The number of avoidable factors identified per case file reviewed increased with the severity of the hypoxic event, mild asphyxia 0.74, neonatal near miss without HIE 0.85, HIE survivor 0.91, and stillbirth or neonatal death 1.29 (Table 2).
The avoidable factors of the whole study population (all cases of birth asphyxia in all severities) were analysed and the findings as shown in Figure 2. The major avoidable factors were: refusal of medical treatment; inadequate facilities; no detection of or reaction to fetal distress; and incorrect management of second stage of labour. Incorrect management of the second stage of labour included prolonged second stage without intervention and inappropriate use of vacuum or forceps. Other major avoidable factors included delay in seeking expert advice (in calling the doctor on call or referring to a next level hospital), incorrect use or interpretation of the partogram, and lack of transport. In the HIE group alone, 50 avoidable factors were found. The avoidable factors associated with HIE cases alone (Fig. 3) were comparable with the whole group. The distribution of avoidable factors between patient related, administrative problems, and medical personnel related, was also similar. Again, the major avoidable factor was incorrect management of second stage of labour, followed by denial of medical treatment, poor detection of or reaction to fetal distress.
2. Avoidable factors in women with neonates with “birth asphyxia”.

3. Avoidable factors in women with neonates with HIE.

Discussion
A confidential enquiry into women delivering babies with “birth asphyxia” occurring at Kalafong Hospital was performed on cases delivered in 2008 and 2009. During this time period 210 neonates were born that were considered to have “birth asphyxia’; of these 125 were thought to have severe asphyxia, namely either requiring intubation for resuscitation, other assisted ventilation and/or HIE. Eighty-four cases had HIE of which 15 subsequently died. There were more than five times the number neonates with HIE cases than neonatal deaths due to intrapartum asphyxia. This group of HIE cases makes a useful number to audit to identify failures within the health system. The avoidable factors of the HIE group were similar to the avoidable factors found in the whole group. HIE is an easily identifiable clinical condition which is not readily confused with other conditions. Thus an analysis of the case management of the woman and the neonate that developed HIE can be readily used to identify problems in the management of labour. Neonatal deaths and intrapartum stillbirths should continue to be reviewed, the additional HIE cases will enable a more rapid assessment of problems with intrapartum management without incorporating cases where there was doubt about intrapartum hypoxia. The review of all these cases will identify problems with intrapartum care and by addressing the problems all women in labour should benefit.
The biggest limitation of this study was the case notes that could not be retrieved (21.9% of cases). However, the sample was large enough to be able to identify the major management problems of women in labour. The low number of avoidable factors found in cases of birth asphyxia (37%) was unexpected but in part may be due to the large number of missing files. The avoidable factors were distributed mainly in the neonatal near miss and stillbirth and neonatal death groups, with the least being found in the mild birth asphyxia group. In other words the more severe the hypoxia the more often avoidable factors were identified. In a Scottish report on severe intrapartum events (Kernaghan et al., 2005) similar figures were reported namely: “55% of cases were judged as ‘appropriate care, well managed’ and 5% as ‘incidental sub-optimal care, lessons can be learnt although it did not affect the final outcome”. The Scottish rate of intrapartum-related asphyxia meeting their case definition was 1.5/1000 births. Their case definition was essentially HIE, neonatal deaths and intrapartum deaths due to intrapartum hypoxia. Using the same definition the rate at Kalafong Hospital was 9.7/1000 births.
This “birth asphyxia” group as a whole (24.6%) and the stillbirths and neonatal deaths due to intrapartum hypoxia (28.6%) in particular had a higher rate of HIV infection than the population delivering at Kalafong which had a HIV infection rate of 21.5%. Although not designed to assess the impact of HIV infection on intrapartum outcomes, the finding is in keeping with and increased prevalence of perinatal deaths due to intrapartum asphyxia described in the same population (Pattinson et al., 2010).
One of the goals of this study was to identify avoidable factors related to managing labour and then to make recommendations so that these problems could be avoided in the future.
Strikingly in the patient related group of avoidable factors, missed opportunities and sub-standard care there were a large proportion of patients declining medical treatment: in the case notes this was recorded as ‘uncooperative’. An epidural service is not available in the labour ward at Kalafong Hospital. The high number of “uncooperative” women might be the result of patients not receiving adequate alternative pain relief, and sometimes become difficult to manage. Introducing strict protocols for pain relief in labour, and, ideally the option for an epidural anaesthesia, in combination with counselling at the antenatal clinic about what to expect in labour, might solve this problem.
In the administrative problems group, the problems identified have been detected before, namely inadequate transport (especially when pregnant women are referred between two different health institutions), inadequate facilities (especially availability of adequate equipment for assisted deliveries), and insufficient staff (especially doctors). However, there was also a reasonable number of cases where there was no reason noted for the delay in treatment indicating poor record keeping. An obstetric unit should be organised such that there is the ability to intervene as soon as the decision is made to do so. Another remarkable finding was that in all but one case, there was no note of active intra-uterine resuscitation. Aside from left lateral tilt, there was no note of the use of tocolytica or amnio-infusion. All staff, also from referring centres, should be made aware that introducing intra-uterine resuscitation could decrease the damage the delay in getting definitive treatment might cause in the fetus and mother.
The majority of avoidable factors were medical personnel related, and not related to lack of facilities and transport as is often supposed. A significant number of cases were found with inadequate management of the second stage of labour. This inadequate management included prolonged second stage of labour without intervention, but also inappropriate use of forceps or vacuum. Attempted assisted delivery failed in a number of cases, after which a caesarean section was performed. This suggests the selection of cases for assisted delivery was sub-optimal. Other problems in this group were delay in seeking expert advice (calling the doctor on duty, referring to a next level of care), incorrect use and interpretation of the partogram, and delay in making the diagnosis of abnormalities in labour such as breech presentation.
Inevitably recommendations advise a programme of further training of medical personnel, (both midwives and doctors) in the skills required to manage labour. This must include training in the interpretation of cardiotocographs. Emphasis will need to be put on the second stage of labour, with training sessions in assisted deliveries using mannequins (Draycott et al., 2006; 2008). Furthermore, the introduction of a checklist to promote decision making in the labour ward while using the partogram might be valuable. In general, organising more effective teaching and training occasions for the staff dealing with patients in labour and ensuring all are trained and involved in simulation training exercises should decrease the amount of neonates suffering from intrapartum asphyxia (Siassakos et al., 2009).
Conclusion
The avoidable factors described in a confidential enquiry concentrating on the labour management of women delivering neonates with all grades of “birth asphyxia” were similar to those found in women delivering neonates with HIE. “Birth Asphyxia” is a poorly defined condition with many causes. HIE in neonates results from intrapartum hypoxia and is a clearly defined condition. Thus analysing the intrapartum care of women who delivered neonates with HIE is useful to identify problems in the management of women in labour in general. By studying these relatively few cases, problems identified in intrapartum care can be addressed leading to improved care of all women in labour.
Acknowledgments
We would like to thank Professor Suzanne Delport for giving us access to the neonatal database and for confirming the diagnosis of hypoxic ischaemic encephalopathy in those babies affected.
Contributor Information
A. De Knijf, Registrar, Department of Obstetrics and Gynaecology, KULeuven, Belgium
R.C. Pattinson, MRC Maternal and Infant Health Care Strategies Research Unit, Department of Obstetrics and Gynaecology, University of Pretoria, Kalafong Hospital, Pretoria, South Africa
References
- Avenant T. ‘Neonatal near miss : a measure of the quality of obstetric care’. Best Pract Res Clin Obstet Gynaecol. 2009;23:369–374. doi: 10.1016/j.bpobgyn.2008.12.005. [DOI] [PubMed] [Google Scholar]
- Buchmann EJ, Pattinson RC, Nyathikazi N. Intrapartum-related birth asphyxia in South Africa – lessons from the first national perinatal care survey. S Afr Med J. 2002;92:897–901. [PubMed] [Google Scholar]
- Buchman JE, Pattinson RC. Babies who die from labour related intrapartum hypoxia: a confidential enquiry in South African public hospitals. Intrapartum care in South Africa: review and guidelines. 2005. pp. 37–41. [DOI] [PubMed] [Google Scholar]
- Buchmann EJ, Velaphi S. Confidential enquiries into hypoxic ischaemic encephalopathy. Best Pract Res Clin Obstet Gynaecol. 2009;23:357–368. doi: 10.1016/j.bpobgyn.2008.12.004. [DOI] [PubMed] [Google Scholar]
- Confidential Enquiry into Maternal and Child Health. Perinatal Mortality 2006: England, Wales and Northern Ireland. London: CEMACH; 2008. [Google Scholar]
- Draycott T, Sibanda T, Owen L, et al. Does training in obstetric emergencies improve neonatal outcome? BJOG. 2006;113:177–182. doi: 10.1111/j.1471-0528.2006.00800.x. [DOI] [PubMed] [Google Scholar]
- Draycott TJ, Crofts JF, Wilson LV, et al. Improving neonatal outcome through practical shoulder dystocia training. Obstet Gyneco. 2008;112:14–20. doi: 10.1097/AOG.0b013e31817bbc61. [DOI] [PubMed] [Google Scholar]
- Kernaghan D, Penney G, Adamson L. Scotland-wide Learning from Intrapartum Critical Events: Final Report Covering events in 2005. Scottish Programme for Clinical Effectiveness in Reproductive Health. 2006;(publication number 28)
- Lawn JE, Cousens S, Zupan J. Lancet Neonatal Survival Steering Team. 4 million neonatal deaths: When? Where? Why? Lancet. 2005;365:891–900. doi: 10.1016/S0140-6736(05)71048-5. [DOI] [PubMed] [Google Scholar]
- Nelson KB. Is it HIE? And why that matters. Acta Paediatr. 2007;96:1113–1114. doi: 10.1111/j.1651-2227.2007.00364.x. [DOI] [PubMed] [Google Scholar]
- Pattinson RC. Why babies die--a perinatal care survey of South Africa, 2000-2002. S Afr Med J. 2003;93:445–450. [PubMed] [Google Scholar]
- Pattinson RC. Challenges in saving babies – avoidable factors, missed opportunities and substandard care in perinatal deaths in South Africa. S Afr Med J. 93:450–455. [PubMed] [Google Scholar]
- Pattinson RC, Hulsbergen MH, Van Hoorick L. The effect of maternal HIV infection on maternal conditions and perinatal deaths in southwest Tshwane. FV&V in ObGyn. 2010;2:227–231. [PMC free article] [PubMed] [Google Scholar]
- Pearson GA. Why children die: a pilot study 2006; England (South West, North East and West Midlands), Wales and Northern Ireland. London: CEMACH; 2008. [Google Scholar]
- Siassakos D, Crofts JF, Winter C, et al. The active components of effective training in obstetric emergencies. BJOG. 2009;116:1028–1032. doi: 10.1111/j.1471-0528.2009.02178.x. [DOI] [PubMed] [Google Scholar]
- Velaphi S, Pattinson R. Avoidable factors and causes of neonatal deaths from perinatal asphyxia-hypoxia in South Africa: national perinatal survey. Ann Trop Paediatr. 2007;27:99–106. doi: 10.1179/146532807X192462. [DOI] [PubMed] [Google Scholar]
- Ward HR, Howarth GR, Jennings OJ, et al. Audit incorporating avoidability and appropriate intervention can significantly decrease perinatal mortality. S Afr Med J. 1995;85:147–150. [PubMed] [Google Scholar]