

Abstract
Background: The role of reproductive surgery is declining due to the widespread availability of assisted reproductive technology, but an evidence-based fundament for this decline is lacking. We therefore performed a systematic review of the literature.
Methods: We searched MEDLINE, EMBASE and the Cochrane Library for randomised trials evaluating laparoscopic or hysteroscopic interventions in subfertile women, studying pregnancy or live birth rates. We present an overview of the results and quality of the detected studies.
Results: The methodological quality of the 63 detected studies was mediocre. The laparoscopic treatment of minimal/ mild endometriosis might increase the pregnancy rate but the two major studies report conflicting results. Excision of the endometriotic cyst wall increases the spontaneous conception rate (RR 2.8, 95% CI 1.4-5.5). Laparoscopic ovarian drilling results at least in equal pregnancy rates as gonadotropin treatment (RR 1.0, 95% CI 0.83-1.2) but decreases the multiple pregnancy rate (RR 0.16, 95% CI 0.04-0.58). Laparoscopic tubal surgery for hydrosalpinx prior to IVF increases the pregnancy rate (RR 1.9, 95% CI 1.4-2.7). Removal of polyps prior to IUI increases the pregnancy rate (RR 2.2, 95% CI 1.6-3.1). Myomectomy for submucosal fibroids results in higher pregnancy rates (RR 2.2, 95% CI 1.6-2.9). The removal of intramural/ subserosal fibroids shows a beneficial trend, albeit not statistically significant (RR 1.2, 95% CI 0.75-1.9). Hysteroscopy in patients with recurrent IVF failure increases the pregnancy rates even in the absence of pathology (RR 1.6, 95% CI 1.3-1.9).
Conclusions: Although the limited evidence indicates a positive role for some surgical reproductive interventions, we should be very cautious in providing guidelines for clinical practice in reproductive surgery since more research is needed.
Keywords: Laparoscopy, hysteroscopy, reproductive surgery, effectiveness, pregnancy rate, live birth rate
Abbreviations
ART: assisted reproductive technology
CDSR: Cochrane Database of Systematic Reviews
CENTRAL: Cochrane Central Register of Controlled Trials
CI: confidence interval
DARE: Database of Abstracts of Reviews of Effects
HTA: Health Technology Assessment Database
IVF: in vitro fertilisation
IUI: intrauterine insemination
MH-F: Mantel-Haenszel, fixed effects model
mRCT: metaRegister of Controlled Trials
PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
RR: risk ratio
RCT: randomised controlled trial
Introduction
Worldwide ART has replaced reproductive surgery for tubal factor infertility, limiting its role as first-line treatment (Bosteels et al., 2007). It is not clear whether this change in clinical practice is due to the higher cost-effectiveness of ART compared to reproductive surgery or caused by other factors such as a lack of surgical expertise, patient’s desires to achieve results rapidly or the concern to protect patients from procedure-related complications. In moderate and severe endometriosis radical laparoscopic surgery is often delayed until several ART cycles have failed (Littman et al., 2005). Its surgical treatment necessitates a high level of expertise (Kennedy et al., 2005).
As a consequence, laparoscopy is increasingly bypassed in the diagnostic work-up of infertility (Fatum et al., 2002). Some authors report that the exploration by diagnostic laparoscopy in an infertile population either did not reveal any pathology or only minimal or mild endometriosis in 40-70% of cases (Forman et al., 1993). From a prognostic point of view, the test ‘diagnostic laparoscopy’ fails to be an ideal predictor for infertility (Collins et al., 1995; Mol et al., 1999). However, the shift away from reproductive laparoscopic surgery favoring ART is not supported by solid evidence.
The position of hysteroscopy in current fertility practice is similarly unclear. Used on an outpatient basis with small calibre hysteroscopes, its technical feasibility and high patient compliance in general gynaecological practice are demonstrated by numerous RCTs (Kremer et al., 2000; Soriano et al., 2000; Unfried et al., 2001; De Angelis et al., 2003; Guida et al., 2003; Litta et al., 2003; Pellicano et al., 2003; Marsh et al., 2004; Shankar et al., 2004; Campo et al., 2005; Sharma et al., 2005; Garbin et al., 2006; Guida et al., 2006; Sagiv et al., 2006; De Placido et al., 2007; Kabli and Tulandi, 2008). However, neither the ease of use nor the low costs should by themselves justify the widespread application of a surgical procedure. Indeed, the number of RCTs demonstrating the effectiveness of hysteroscopy in treating female infertility is limited (Bosteels et al., 2010).
Our aim is to study the effectiveness of reproductive surgery in treating female subfertility, by giving an overview of all published randomised trials measuring pregnancy or live birth rates.
Methods
Literature search methodology
For the current systematic review no written protocol was registered.
We aimed to identify randomised clinical trials (RCTs) or systematic reviews of such trials on reproductive surgery in infertile women with pregnancy or live birth rate as the primary outcome. To do so, we searched the Cochrane Library (1970 to June 1st 2010) for relevant trials in the CDSR, DARE, CENTRAL or HTA databases. We also searched the National Library of Medicine’s MEDLINE using a combination of textwords and MeSH terms for “laparoscopy”, “hysteroscopy” ,“infertility”, “pregnancy rate” and “live birth rate” (1966-June 1st 2010) and Excerpta Medica EMBASE (1974 to June 1st 2010). The search strategies in the appropriate thesaurus for each database were developed by a librarian at the University Biomedical Library Campus Gasthuisberg, Katholieke Universiteit Leuven and are described in the addendum. The search strategy included the filters from the Cochrane Collaboration website (Haynes et al., 1994; Dickersin et al., 1994), developed for the detection of randomised controlled trials with reported sensitivities of 95 and 99% (Shojania and Bero, 2001; Robinson and Dickersin, 2002; Glanville et al., 2006). We also searched the Current Controlled Trials (metaRegister) at http://www.controlled-trials.com/ for registered relevant trials. The last up-dated search was done on June 1st 2010.
Language restrictions were not applied, and the searches were done simultaneously and independently by two authors (JB and TD).The reference lists of all known primary articles were examined independently by the same two authors (JB and TD). We also used the ‘related articles’ function of PubMed, as well as the reference lists of detected articles to look for relevant studies.
Study selection
We included RCTs reporting on pregnancy or live birth rates, but excluded non-randomised trials, studies not reporting on reproductive outcome or done in a population with gynaecological problems other than infertility as well as trials on diagnostic accuracy, technical feasibility, patient compliance and cost-effectiveness. Study selection was done by two authors independently based on reviewing the full text article (JB and TD). The κ-value of inter-reviewer agreement on the final inclusion of the relevant RCTs was 0.82. In case of disagreement, the opinion of a third author was asked (SW) until consensus was reached.
Data extraction and critical appraisal
For data extraction and critical appraisal of the methodology, the PRISMA Statement was followed (Moher et al., 2009). The characteristics of the different study populations, the control and study intervention as well as other relevant study characteristics were extracted from the full text articles. The corresponding authors were contacted in case of unclear study methodology or to obtain missing data. Two authors (JB and TD) independently extracted relevant study data. The critical appraisal based on the internal validity, the magnitude of the treatment effect and the general applicability was done by using standardised work sheets for quality assessment of randomised controlled trials from the website of the Dutch Cochrane Centre (http://dcc.cochrane.org/sites/dcc.cochrane.org/files/uploads/RCT.pdf). The internal validity was based on the description of the randomisation sequence generation, allocation concealment, blinding of physicians/patients and outcome assessors, the assessment of incomplete data and whether selective reporting or other forms of bias were likely or not.
Data synthesis and statistical analysis
Statistical analysis was done using the latest updated software provided by the Cochrane Collaboration (Rev Man 5 version 5.0.24, April 16th 2010). Dichotomous data were extracted in 2x2 tables. After consulting with a biostatistician we decided to express the results of individual trials and of the meta-analyses as risk ratios (RR) with 95% confidence limits (95% CI) using a fixed effects model (Mantel- Haenszel method). A sensitivity analysis comparing the use of odds ratios (OR) to risk ratios did not yield differences in the direction of the observed treatment effect, but in general the estimations of the treatment effect were more conservative with the use of RR. To facilitate clinical interpretation, results were re-expressed as numbers needed-to-treat (NNT) with 95% confidence intervals (CI). The NNTs were calculated from the RR in the meta-analyses using appropriate mathemical formulae available from the Cochrane Handbook for Systematic Reviews of Interventions. Statistical heterogeneity was assessed with the Chi-square test and the I² test.
We estimated the risk of bias at the study level and across studies using the risk of bias tool provided by the Cochrane Collaboration based on the randomisation sequence generation, concealment of allocation, blinding of patients/ physicians and outcome assessors, selective reporting of outcomes, whether or not incomplete data were addressed and the probability of other forms of bias.
We assessed the quality of the included trials by providing levels of evidence using the software provided by the Cochrane Collaboration (GRADE profiler version 3.2.2.20090501). An alternative grading system was used by allocating a ‘level E’ for ‘evidence of an effect’ when there was evidence of a significant difference between the interventions studied for the pregnancy or live birth rate or a’level G’ for ‘gap in evidence’ when there was insufficient evidence of effectiveness or harm. A label ‘E&G’ was allocated when there was some evidence of a significant effect along with some gaps for the primary outcomes.
Results
The process of literature search and selection is described in Figure 1. We retrieved 106 possibly relevant articles in MEDLINE, 334 possibly relevant articles in EMBASE and 170 relevant reviews, clinical trials and abstracts of reviews from the Cochrane Library. We identified 37 possibly relevant trials in the Current Controlled Trials Register. After screening of the abstracts or titles of non duplicate 592 possibly relevant publications, 97 full text articles were assessed for eligibility. Finally, we included 63 randomised trials on reproductive surgical techniques and pregnancy outcome. An overview of these trials and a summary of their findings grouped according to the specific pathology or clinical setting are presented in table 1.
1. PRISMA 2009 Flow Diagram: Systematic Review of benefit after reproductive surgery.

Table 1. Summary of findings of included studies.
| reference | population | intervention | comparison | outcome | RR (95%CI) |
|---|---|---|---|---|---|
| Laparoscopic treatment of minimal and mild endometriosis in women with otherwise unexplained infertility | |||||
| Gruppo Italiano 1999 | 101 women aged 20-39 y with unexplained infertility > 12m and r-AFS I endometriosis | resection/ ablation (n = 54) | diagnostic laparoscopy only (n = 47) | TDR PR (unclear) |
0.88 (0.40, 1.9) 0.81 (0.41, 1.6) |
| Marcoux 1997 | 341 women < 37 y with unexplained infertility > 2 y and r-AFS I endometriosis | excision/ ablation and adhesiolysis (n = 172) | diagnostic laparoscopy only (n = 169) | CPR 9 m FR |
1.7 (1.1, 2.5) 1.9 (1.2, 3.1) |
| Laparoscopic treatment of endometriotic cysts in infertile women | |||||
| Alborzi 2004 | 100 women with a mean age of 28 y and the presence of an endometrioma > 3 cm on US | excision (n = 32) | drainage and ablation (n = 30) | CPR 12 m | 2.5 (1.2, 5.2) |
| Beretta 1998 | 64 women aged 20-40 y with endometrioma > 3 cm on US | excision (n = 9) | bipolar ablation (n = 17) | CPR 24 m | 5.7 (0.68, 47) |
| Demirol 2006 | 99 women with mean age 35 y and endomtriomas ≥ 3 and < 6 cm on TVUS | drainage and dissection of the pseudocapsule (n = 49) | ICSI (n = 50) | PR/P | 0.91 (0.54, 1.5) |
| Laparoscopic ovarian drilling for ovulation induction in infertile women with PCOS | |||||
| Al-Mizyen 2007 | 21 women aged 20-38 ywith CC-resistant PCOS | bilateral LOD +/- CC (n = 10) | unilateral LOD +/- CC (n = 10) | PR/P? unclear |
0.83 (0.37, 1.8) |
| Amer 2009 | 72 anovulatory women aged 18-39 y with PCOS | LOD (+/_ CC) (n = 33) | clomiphene citrate 12 c (+/-LOD) (n = 32) | PR LBR/P | 0.87 (0.59, 1.3) 0.81 (0.50, 1.3) |
| Balen 1994 | 10 patients mean age 29.5 y with refractory PCOS | unilateral LOD (n = 4) | bilateral LOD (n = 6) | PR/P? unclear | not estimable |
| Bayram 2004 | 168 women mean age 29 y with CC-resistant PCOS | LOD +/-CC - rFSH (n = 83) | gonadotropin (rFSH) max 6 c (n = 85) | OPR/P LBR/P |
1.01 (0.81, 1.2) 1.04 (0.82, 1.3) |
| Farquhar 2002 | 50 women aged 20-38 y with CC-resistant PCOS | LOD (n = 29) | gonadotropin (HMG or rFSH) 3 cycles (n = 21) | OPR/P LBR/P |
0.72 (0.24, 2.2) 0.72 (0.20, 2.6) |
| Ghafarnegad 2010 | 100 women with CC-resistant PCOS | LOD (n = 50) | gonadotropin (n = 50) | OPR/P | 0.80 (0.34, 1.9) |
| Hamed 2010 | 110 women aged 20-35 y with CC- and insuline- resistant PCOS | diagnostic laparoscopy + metformin (n = 55) | LOD (n = 55) | PR/C PR/P | 2.1 (1.02, 4.2) 1.9 (1.02, 3.6) |
| Kaya 2005 | 35 women with CC-resistant PCOS | bilateral LOD (n = 17) | 3 cycles of gonadotropin + IUI (n = 18) | PR/P | 1.1 (0.42, 1.6) |
| Lazoviz 1998 | 57 women with CC-resistant PCOS | LOD (n = 29) | 6 cycles of gonadotropin (n = 28) | PR/P | 1.8 (0.98, 3.4) |
| Palomba 2010 | 50 infertile women with CC-resistant PCOS | LOD + observation (n = 25) | CC + metformin (n = 25) | LBR/C | 1.1 (0.62, 1.9) |
| Roy 2009 | 44 women mean age 29 y with CC-resistant PCOS | bilateral LOD +/- CC (n = 22) | unilateral LOD +/- CC (n = 22) | PR THBR |
1.0 (0.52, 1.9) 0.89 (0.42, 1.9) |
| Roy 2010 | 43 women aged 20-40 y with CC-resistant PCOS | rosiglitazone 4 mg bd + CC (n = 22) | unilateral LOD with multivitamins bd + CC (n = 21) | CPR 6m | 0.82 (0.43, 1.6) |
| Sharma 2006 | 20 women with CC-res. PCO | bipolar LOD (n = 10) | unipolar LOD (n = 10) | PR/P | 0.75 (0.41, 1.4) |
| Vegetti 1998 | 29 women with CC-res. PCO | LOD (n = 16) | gonadotropin (FSH) 6 c (n = 13) | PR/P | 0.33 (0.07, 1.4) |
| Youssef 2007 | 87 women with PCOS | uni.LOD +/-CC (n = 43) | bil.LOD +/-CC (n = 44) | PR/P | 1.1 (0.75, 1.5) |
| Zakherah 2010 | 150 women with CC-resistant PCOS | clomiphene + tamoxifen (n = 75) | LOD without ovulation induction (n = 75) | LBR/P | 0.89 (0.63, 1.3) |
| Pre and postoperative medical therapy for endometriosis surgery | |||||
| Alborzi 2007 | 88 infertile women with endometriosis all stages | pentoxifylline 800 mg (n = 43) | placebo (n = 45) | PR/P | 1.1 (0.65, 1.9) |
| Balasch 1997 | 60 infertile women with r-AFS I/ II endometriosis | pentoxifylline 800 mg (n = 30) | placebo (n = 30) | CPR 12 m | 1.7 (0.64, 4.4 |
| Batioglu 1997 | 25 women with uni- or bilateral endometriomas > 3 cm | postsurgical treatment with triptorelin 3.75 mg im x 4 weekly 6 m (n = 13) | presurgical treatment with triptorelin 3.75 mg im x 4 weekly 6 m (n = 13) | CPR 12 m | 0.46 (0.15, 1.4) |
| Bianchi 1999 | 77 women < 40 y with advanced endometriosis | danazol 600 mg/d during 3 months (n = 36) | no treatment (n = 41) | PR/P | 1.1 (0.53, 2.3) |
| Busacca 2001 | women < 40 y with r-AFS III/ IV endometriosis | GnRHa (n = 15) | no treatment (n = 15) | CPR 18 m | 0.83 (0.32, 2.1) |
| Creus 2008 | 104 women with r-AFS I/II endometriosis | pentoxifylline 800 mg (n = 51) | placebo (n = 53) | CPR 6 m | 2.02 (0.88, 4.6) |
| Loverro 2001 | 62 women with r-AFS III/IV endometriosis | GnRHa (n = 33) | no treatment (n = 29) | PR/P | 0.73 (0.25, 2.1) |
| Parazzini 1994 | 75 women < 38 y with r-AFS III/ IV endometriosis | nafarelin nasal 400 µg daily during 3 months (n = 36) | placebo (n = 39) | PR/P | 1.1 (0.42, 2.8) |
| Telimaa 1987 | 60 women with advanced endometriosis | danazol 600 mg daily (n = 20) or MPA 100 mg dialy (n = 20) | placebo (n = 20) | PR/P | 0.89 (0.09, 8.4) |
| Vercellini 1999 | 269 premenopausal women with endometriosis | score ≥ 4 goserelin sc 3.6 mg /4w 6m (n = 133) | no treatment (n = 134) | PR/P | 0.63 (0.28, 1.4) |
| Surgical treatment for tubal disease in women due to undergo in vitro fertilisation | |||||
| Dechaud 1998 | 60 women mean age with tubal infertility only | bilateral salpingectomy (n = 30) | laparoscopic adhesiolysis (n = 30) | LBR/P | 2.2 (0.95, 4.9) |
| Goldstein 1998 | 35 infertile women aged 22-38 y | salpingostomy/ -ectomy (n = 15) | no surgery (n = 16) | LBR /P | 4.3 (0.54, 33) |
| Hammadieh 2008 | 66 women with uni- or bilateral hydrosalpinx | aspiration (n = 32) | no aspiration (n = 34) | CPR/P | 1.7 (0.69, 4.0) |
| Kontoravdis 2006 | 115 women with uni- or bilateral tubal block | tubal occlusion (n = 50) | salpingectomy (n = 50) | OPR/P | 0.77 (0.48, 1.2) |
| Moshin 2006 | 204 women with ultrasound visible hydrosalpinges | 1. salpingectomy (n = 60) 2. tubal occlusion (n = 78) |
1. no treatment (n = 66) 2. no treatment (n = 66) |
CPR/P CPR/P |
3.2 (1.5, 6.5) 3.3 (1.6, 6.7) |
| Strandell 1999 | 204 infertile women < 39 y prior to first IVF treatment; no fibroids present. | salpingectomy (n = 116) | no surgery (n = 88) | LBR/P | 1.6 (0.90, 2.7) |
| Laparoscopic treatment of fibroids for subfertility | |||||
| Campo 1999 | 60 women mean aged 25-42 y with intramural/subserosal fibroids | surgery preceded by GnRHa (n = 30) | surgery without GnRHa (n = 30) | PR/P | 1.4 (0.66, 2.9) |
| Casini 2005 | 87 women < 35 y with unexplained infertility and one intramural/subserosal fibroid < 4 cm | surgery (n = 40) | no surgery (n = 47) | PR/P | 1.2 (0.75, 1.9) |
| Palomba 2007 | 136 women with symptomatic fibroids or unexplained infertility | laparoscopic myomectomy (n = 68) | myomectomy by minilaparotomy (n = 68) | LBR/P | 1.4 (0.95, 2.2) |
| Seracchioli 2000 | 131 infertile women with at least 2 myomas ≥ 5 cm | abdominal myomectomy (n = 65) | laparoscopic myomectomy (n = 66) | LBR/P | 1.1 (0.80, 1.5) |
| Hysteroscopic treatment of fibroids for subfertility | |||||
| Casini 2005 | 181 women < 35 y with unexplained infertility and one submucosal with or without intramural fibroid < 4 cm | hysteroscopy and/or laparotomy (n = 52) | no surgery (n = 42) | PR/P | 1.9 (0.97, 3.7) |
| Shokeir 2009 | 215 women with otherwise unexplained primary infertility and US diagnosed submucosal fibroids | hysteroscopic myomectomy (n = 101) | diagnostic hysteroscopy and myoma biopsy (n = 103) | PR/P | 2.2 (1.6, 3.2) |
| Surgery by laparoscopy or hysteroscopy prior to IUI or IVF | |||||
| Demirol 2004 | 421 patients with primary infertility and at least 2 failed IVF attempts | 5 mm hysteroscopy (n = 210) | no hysteroscopy (n = 211) | CPR/P | 1.5 (1.1, 2.1) |
| Pérez-Medina 2005 | 215 infertile women planned for IUI with polyps on TVUS | hysteroscopic polypectomy (n = 107) | diagnostic hysteroscopy (n = 108) | CPR | 6 c2.2 (1.6, 3.1) |
| Rama Raju 2006 | 520 patients with primary infertility and at least 2 failed IVF attempts | 5 mm hysteroscopy (n = 265) | no hysteroscopy (n = 255) | CPR/P | 1.6 (1.3, 1.9) |
| Tanahatoe 2005 | 154 infertile women with medical ground for IUI | laparoscopy prior to IUI (n = 77) | IUI first (n = 77) | OPR/P | 0.89 (0.64, 1.2) |
| Hysteroscopic septoplasty | |||||
| Colacurci 2007 | 160 patients with infertility and/ or recurrent pregnancy loss | hysteroscopic septoplasty with the Versapoint needle (n = 80) | hysteroscopic septoplasty with the resectoscope (n = 80) | PR/P | 0.71 (0.54, 0.93) |
| Techniques for pelvic surgery in subfertility | |||||
| Chong 1991 | 37 women with bilateral proximal tubal occlusion needing surgical treatment | Bruhat technique (n = 15) | cuff technique (n = 19) | TPR/P | 1.1 (0.26, 4.6) |
| Comninos 1977 | 30 women with bilateral proximal tubal occlusion undergoing salpingostomy | 1.hydrotubation (n = 15) 2. prosthesis use (n = 15) |
1.no hydrotubation (n = 15) 2. no prosthesis (n = 15) |
TPR/P TPR/P |
0.60 (0.17, 2.1) 2.00 (0.20, 19) |
| Kamel 1999 | 240 women with bilateral tubo-ovarian adhesions and patency | thermocoagulation (n = 120) | electrocoagulation (n = 120) | PR/P | 0.91 (0.66, 1.3) |
| Rock 1984b | 72 patients requesting reversal of sterilisation | operating microscope (n = 36) | loupe (n = 36) | TPR/P | 0.83 (0.56, 1.2) |
| Soihet 1974 | 258 women with tubal infertility needing tubal surgery | 1. early hydrotubation (n = 67) 2. antibiotic (n = 91) 3. tubal stent (n = 100) |
1. late hydrotubation(n = 100) 2. no antibiotic (n = 100) 3. no tubal stent (n = 67) |
TDR/P TDR/P TDR/P |
0.95 (0.39, 2.3) 2.1 (1.1, 4.1) 1.0 (0.43, 2.6) |
| Tulandi 1985 | 67 infertile women with bilateral distal tubal occlusion | salpingostomy by laser (n = 37) | unipolar needle (n = 30) | TPR/P | 1.3 (0.56, 2.9) |
| Tulandi 1986 | 63 infertile women with peri-adnexal adhesion | sadhesiolysis by laser (n = 30) | unipolar needle (n = 33) | TPR/P | 1.0 (0.65, 1.7) |
| Postoperative procedures for improving fertility following pelvic reproductive surgery | |||||
| Comninos 1977 | 30 women with bilateral proximal tubal occlusion undergoing salpingostomy | 1.hydrotubation (n = 15) 2. prosthesis use (n = 15) |
1.no hydrotubation (n = 15) 2. no prosthesis (n = 15) |
TPR/P TPR/P |
0.60 (0.17, 2.1) 2.0 (0.20, 20) |
| Gurgan 1992 | 40 women with CC-resistant PCOS undergoing LOD | second-look (n = 20) | no second-look (n = 20) | LBR/P | 0.78 (0.36, 1.7) |
| Rock 1984a | 206 women with tubal infertility treated with neosalpingostomy or fimbrioplasty | hydrotubation with steroids (n = 86) | hydrotubation without steroids (n = 86) | LBR/P | 1.1 (0.64, 1.9) |
| Soihet 1974 | 258 women with tubal infertility needing tubal surgery | 1. early hydrotubation (n = 67) 2. antibiotic (n = 91) 3. tubal stent (n = 100) |
1. late hydrotubation (n = 100) 2. no antibiotic (n = 100) 3. no tubal stent (n = 67) |
TDR/P TDR/P TDR/P |
0.95 (0.39, 2.3) 2.1 (1.1, 4.1) 1.0 (0.43, 2.6) |
| Tulandi 1989 | 74 women with failure to conceive within 1 year after tubal microsurgery | laparoscopic tubal patency testing +/- adhesiolysis (n = 36) | no laparoscopy (n = 38) | TPR/P | 1.1 (0.66, 1.9) |
| Techniques for adhesion prevention in pelvic reproductive surgery | |||||
| Adhesion SG 1983 | 277 infertile women undergoing open pelvic surgery | dextran (n = 55) | normal saline (n = 47) | PR/P unclear |
0.49 (0.15, 1.6) |
| Jansen 1985 | 103 infertile women undergoing open pelvic microsurgery | dextran (n = 50) | Hartmann solution (n = 53) | CPR/P LBR/P |
0.87 (0.39, 1.9) 0.53 (0.17, 1.6) |
| Larsson 1985 | 109 infertile women undergoing open pelvic surgery | dextran (n = 51) | saline (n = 54) | CPR/P LBR/P |
0.71 (0.38, 1.3) 0.91 (0.33, 2.5) |
| Querleu 1989 | 131 infertile women treated by open pelvic microsurgery | noxytioline (n = 63) | no treatment (n = 63) | PR/P unclear |
0.74 (0.41, 1.3) |
| Rock 1984a | 206 women with tubal infertility treated with neosalpingostomy or fimbrioplasty | hydrotubation with steroids (n = 86) | hydrotubation without steroids (n = 86) | LBR/P | 1.1 (0.64, 1.9) |
| Pellicano 2005 | 36 infertile women with not more than 4 fibroids > 3cm but < 10 cm | hyaluronic acid gel after lap.myomectomy (n = 18) | no hyaluronic acid gel after lap. myomectomy (n = 18) | PR/P | 2.0 (1.1, 3.7) |
DR: delivery rate
FR: fecundity rate
PR: pregnancy rate
c: cycles
m: months
CPR: cumulative pregnancy rate
LBR: live-birth rate
OPR: ongoing pregnancy rate
THBR: take home baby rate
TPR: total pregnancy rate
TDR: term delivery rate
PR/P: pregnancy rate per patient
PR/C: pregnancy rate per cycle
CPR/P: clinical pregnancy rate per patient
LBR/C: live-birth rate per cycle
LBR/P: live-birth rate per patient
How effective is reproductive surgery by laparoscopy in subfertile women compared to alternative treatments?
Minimal and mild endometriosis
There are two RCTs on the effectiveness of laparoscopic surgery for minimal or mild endometriosis in women with otherwise unexplained subfertility (Marcoux et al., 1997; Gruppo Italiano, 1999). The larger Canadian trial (n = 341) showed a treatment effect of the laparoscopic excision/ablation of minimal or mild endometriosis for the ongoing pregnancy rate at 9 months compared to diagnostic laparoscopy (RR 1.7, 95% CI 1.1-2.5). For every eight women with unexplained subfertility and associated minimal or mild endometriosis treated by laparoscopic excision or ablation, it is expected that one additional person will have an ongoing pregnancy (NNT = 8, 95% CI 5 to 32). The beneficial treatment effect was still present in patients without endometriotic adhesions (n = 284) as demonstrated by a subgroup analysis (cumulative incidence ratio 1.6, 95% CI 1.2-2.5).
The smaller Italian study (n = 101) failed to demonstrate a statistically significant difference, but more important did not even show a trend to a higher number of pregnancies (RR 0.81, 95% CI 0.41-1.6) or an increase in the live-birth rate (OR 0.88, 95% CI 0.40-1.9). Despite the conflicting results, the data of both trials were pooled in a Cochrane review (Jacobson et al., 2010). The laparoscopic treatment of minimal or mild endometriosis shows a trend in increasing the ongoing pregnancy or live birth rate which is marginally significant (RR 1.5, 95% CI 1.0-2.1). By doing a re-analysis of the primary data of the Italian trial, we found that data from 5 women in the intervention group and 3 women in the control group were missing. This discrepancy could not be clarified after contacting the authors. A post hoc sensitivity analysis aimed at examining whether the missing data could have had an impact on the results, did not demonstrate statistically significant differences between the intervention and control groups in either a worst case (RR 0.74, 95% CI 0.35-1.5) or a best case scenario (RR 1.3, 95% CI 0.66-2.6), similar to the adjusted data from the available case analysis (RR 0.88, 95% CI 0.40-1.9). By consequence, this discrepancy would not have had implications for the results and conclusions in the meta-analysis.
Endometriotic cysts in moderate and severe endometriosis
We retrieved two randomised trials on the effectiveness of two different techniques for the treatment of endometriotic cysts (Alborzi et al., 2004; Beretta et al., 1998). The first trial (n = 62) demonstrated a treatment effect favoring the excision of the endometriotic cyst wall compared to drainage and ablation for the cumulative pregnancy rate at 12 months (RR 2.5, 95% CI 1.2-5.2) (Alborzi et al., 2004). A second smaller trial (n = 26) showed a trend in favor of the excision technique in increasing the cumulative pregnancy rate at 24 months, but the difference between both techniques in this underpowered trial was not statistically significant (RR 5.7, 95% CI 0.68-47) (Beretta et al., 1998). Meta-analysis of the results of these two trials, published in a Cochrane review (Hart et al., 2007) demonstrated an important treatment effect of the excision technique compared to the ablation technique for the chance of spontaneous conception at 12 months(RR 2.8, 95% CI 1.4-5.5). For every three infertile women with endometriotic cysts greater than 3 cm treated by laparoscopic excision, it is expected that one additional person will have a spontaneous conception at 12 months compared to fenestration and ablation (NNT = 3, 95% CI 2 to 3). There is no evidence of significant statistical heterogeneity (Chi² = 0.22, I² = 0%). Another randomised trial (n = 99) studied the effectiveness of drainage, followed by dissection of the pseudocapsule of ovarian endometriomas between 3 and 6 cm on transvaginal ultrasound prior to ICSI compared to starting ART without prior surgical treatment (Demirol, 2006). There was a trend in lower pregnancy rates after the removal of endometriotic cysts prior to IVF compared to starting ICSI immediately without surgery, but the difference is not statistically significant (RR 0.91, 95% CI 0.54-1.5).
Deeply infiltrative endometriosis
We did not find randomised trials on the effectiveness of the laparoscopic treatment of deeply infiltrative endometriosis in subfertile women with or without pain compared to expectant management or IUI/ IVF.
Laparoscopic ovarian diathermy in PCOS patients
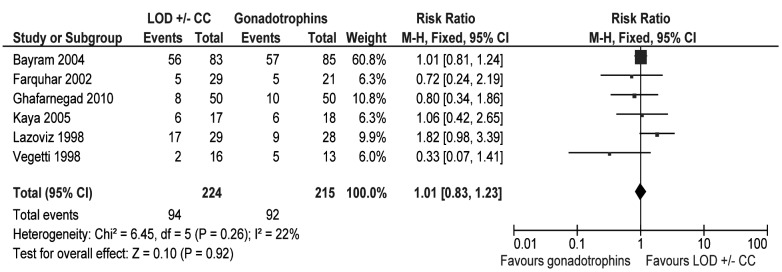
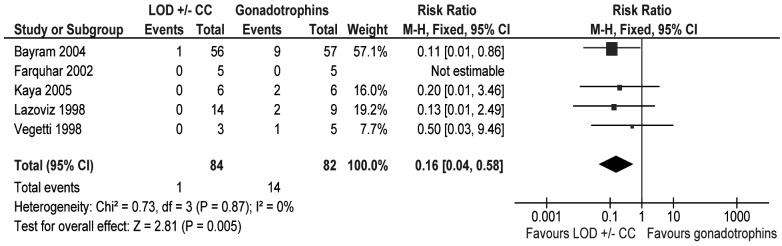
We detected six randomised trials with 439 patients on laparoscopic ovarian diathermy (LOD) with or without clomiphene citrate in clomiphene-resistant PCOS compared to gonadotropin treatment (Bayram et al., 2004; Farquhar et al., 2002; Ghafarnegad et al., 2010; Kaya et al., 2005; Lazoviz et al., 1998; Vegetti et al., 1998). There were no differences in ongoing pregnancy rate per couple between the two treatment strategies (RR 1.0, 95% CI 0.83-1.2) as presented in Figure 2. There were however less multiple pregnancies per ongoing pregnancy in the LOD group compared to the gonadotropin group (RR 0.16, 95% CI 0.04-0.58) as demonstrated by a meta-analysis of five randomised trials in 166 patients (Bayram et al., 2004; Farquhar et al., 2002; Kaya et al., 2005; Lazoviz et al., 1998; Vegetti et al., 1998) (Fig. 3). For every six infertile women with clomiphene-resistant PCOS treated by LOD, it is expected that one person less will have a multiple pregnancy compared to gonadotropin treatment (NNT = 6, 95% CI 4 to13). There is no evidence of significant statistical heterogeneity (Chi² = 0.41, I² = 0%).
2. LOD with or without clomiphene versus gonadotrophins. Outcome: ongoing pregnancy rate per couple.
3. LOD with or without clomiphene versus gonadotrophins. Outcome: multiple pregnancy rate per couple.
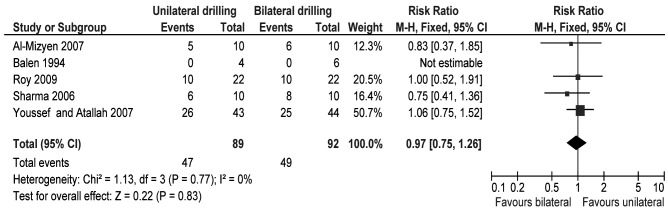
We retrieved five randomised trials (n = 181) comparing unilateral versus bilateral LOD in clomiphene resistant PCOS patients (Al-Mizyen and Grudzinskas, 2007; Balen and Jacobs, 1994; Roy et al., 2009, Sharma et al., 2006; Youssef and Atallah, 2007). Meta-analysis did not indicate a treatment effect of bilateral LOD for the clinical pregnancy rate compared to unilateral LOD (RR 0.97, 95% CI 0.75-1.3) as illustrated by the forest plot in Figure 4.
4. Unilateral versus bilateral laparoscopic ovarian diathermy in clomiphene-resistant PCOS patients. Outcome: clinical pregnancy rate per patient.
Tubal infertility
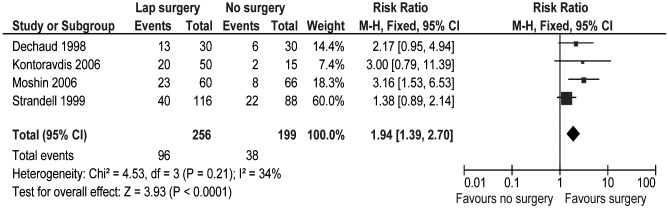
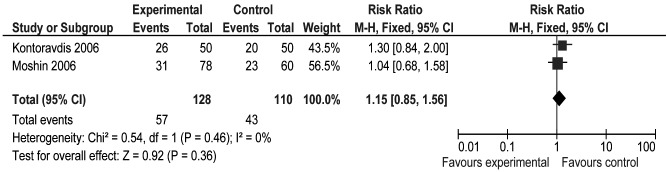
We found five randomised trials on the surgical treatment of hydrosalpinx prior to IVF (Dechaud et al., 1998; Hammadieh et al., 2008; Kontoravdis et al., 2006; Moshin and Hotineanu, 2006; Strandell et al., 1999). Meta-analysis of four trials (n = 455) (Dechaud et al., 1998; Kontoravdis et al., 2006; Moshin and Hotineanu, 2006; Strandell et al., 1999) showed a treatment effect of laparoscopic tubal surgery (any type) compared to no surgical treatment (any type) for the pregnancy rate (any definition) as presented in Figure 5 (RR 1.9, 95% CI 1.4-2.7). For every seven infertile women with hydrosalpinx treated surgically prior to IVF, it is expected that one additional person will have a pregnancy (any definition) compared to starting IVF immediately (NNT = 7, 95% CI 5 to11). There is no evidence of significant statistical heterogeneity (Chi² = 0.69; I² = 0%). Meta-analysis of two RCTs (n = 209) (Kontoravdis et al., 2006; Moshin and Hotineanu, 2006) comparing tubal occlusion versus no treatment demonstrated a treatment effect of tubal occlusion for the clinical pregnancy rate (RR 3.2, 95% CI 1.7-6.0).There is no evidence of significant statistical heterogeneity (Chi² = 0.01, I² = 0%). For every four women with hydrosalpinges treated by a tubal occlusion prior to IVF, it is expected that one additional person will have a clinical pregnancy (NNT = 4, 95% CI 3 to 6). The forest plot in Figure 6 graphically demonstrates that tubal occlusion is at least as effective as laparoscopic salpingectomy in improving the clinical pregnancy rate (RR 1.1, 95% CI 0.85-1.6). The transvaginal aspiration of fluid after oocyte pick-up (Hammadieh et al., 2008) showed a trend in increasing the clinical pregnancy rate compared to no treatment, but the difference was not statistically significant (RR 1.7, 95% CI 0.69- 4.0). We did not find randomised trials that compared the effectiveness of surgical reversal of tubal sterilisation with IVF in women with infertility due to sterilisation (Yossry et al., 2006). There are no randomised trials, to the best of our knowledge, comparing the effectiveness of reproductive surgery for tubal factor infertility to either expectant management or IVF treatment.
5. Laparoscopic surgery on the Fallopian tubes (all types) versus no surgery on the Fallopian tubes (all types). Outcome: pregnancy rate (any definition).
6. Tubal occlusion versus salpingectomy in subfertile women with hydrosalpinx prior to IVF. Outcome: clinical pregnancy rate.
Prevention of adhesions after reproductive surgery
With respect to peritubal adhesions, we found only one RCT (n = 74) on the effectiveness of salpingo-ovariolysis during a second-look laparoscopy after previous tubal microsurgery compared to no second-look procedure: there was a trend in increasing the cumulative probability of pregnancy (RR 1.1, 95% CI 0.66-1.9), albeit statistically not significant (Tulandi et al., 1989). We retrieved one small trial (n = 36) studying the effectiveness of hyaluronic acid gel application after laparoscopic myomectomy in infertile women with not more than 4 symptomatic fibroids larger than 3 but smaller than 10 cm (Pellicano et al., 2005). The chance of becoming pregnant was doubled in the group treated with hyaluronic acid gel application compared to no treatment with anti adhesion barrier (RR 2.0, 95% CI 1.1-3.7). Definitive conclusions cannot be made since this trial has several methodological flaws due to unclear methodology of allocation concealment and randomisation.
Intramural and subserosal fibroids
One randomised trial including 87 women with one intramural and/ or subserosal fibroid smaller than 4 cm and otherwise unexplained infertility studied the effectiveness of surgery by laparoscopy or laparotomy compared to no surgery (Casini et al., 2006). There was no statistically significant difference, although there was a trend in improving the pregnancy rate per patient at 12 months (RR 1.2, 95% CI 0.75-1.9).
Diagnostic and/or operative laparoscopy prior to IUI treatment
In a randomised trial including 154 infertile women with medical ground for IUI, there was no evidence of a treatment effect of laparoscopy prior to IUI for the ongoing pregnancy rate per patient (RR 0.89, 95% CI 0.64-1.2) compared to immediate treatment with IUI (Tanahatoe et al., 2005).
How effective is reproductive surgery by hysteroscopy in subfertile patients compared to alternative treatments?
Endometrial polyps
Hysteroscopic removal of endometrial polyps detected by ultrasound significantly doubles the clinical pregnancy rate when compared to diagnostic hysteroscopy and polyp biopsy according to one randomised trial including 215 subfertile women with uterine polyps undergoing IUI (RR 2.2, 95%CI 1.6-3.1) (Pérez-Medina et al., 2005). For every three subfertile women with uterine polyps treated by hysteroscopic polypectomy, it is expected that one additional person will have a clinical pregnancy (NNT = 3, 95%CI 2 to 5).
Submucosal fibroids
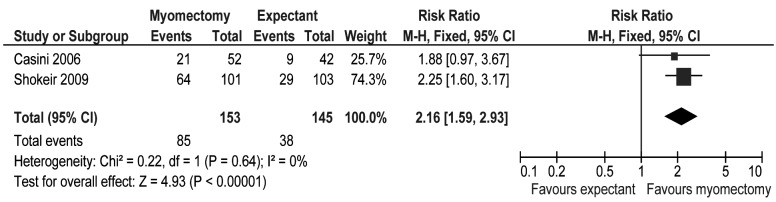
In patients with submucosal fibroids with or without intramural fibroids and otherwise unexplained subfertility, hysteroscopic myomectomy doubles the pregnancy rate compared to expectant management (RR 2.2, 95% CI 1.6- 2.9) (Fig. 7) as demonstrated by a meta-analysis of two randomised trials in 298 patients (Casini et al., 2006; Shokeir et al., 2009). For every three women with submucosal fibroids and otherwise unexplained infertility treated by hysteroscopic myomectomy, it is expected that one additional person will have a pregnancy compared to expectant management (NNT 3, 95%CI 2 to5). There is no evidence of significant statistical heterogeneity (Chi² = 0.22; I² = 0%).
7. Hysteroscopic myomectomy versus expectant management in women with ultrasonographically diagnosed submucosal myomas and otherwise unexplained infertility. Outcome: clinical pregnancy rates.
Intrauterine septa
We did not find RCTs on the effectiveness of hysteroscopic septum resection compared to expectant management or alternative treatments in patients with otherwise unexplained primary subfertility. One randomised trial compared the effectiveness of two methods of hysteroscopic treatment of uterine septa (resectoscopy versus Versapoint electrode) in a mixed population of 160 patients with subfertility and recurrent pregnancy loss (Colacurci et al., 2007) and found no differences in outcome between both techniques. A randomised trial (http://www.studies-obsgyn.nl/trust NTR 1676) studying the effectiveness of hysteroscopic metroplasty in patients with recurrent pregnancy loss is ongoing.
Intrauterine adhesions
There are no randomised trials on the effectiveness of hysteroscopic synechiolysis with pregnancy or live birth rates as primary outcome. We excluded one pseudo-randomised trial on the effectiveness of hysteroscopy in treating intrauterine adhesions (Pabuccu et al., 2008). Furthermore we excluded two randomised trials on the effectiveness of auto-cross linked hyaluronic acid gel in the prevention of intra-uterine adhesions after hysteroscopic adhesiolysis (Acunzo et al., 2003) and after hysteroscopic surgery (Guida et al., 2004) since data on reproductive outcome are lacking.
Hysteroscopy in patients with recurrent IVF failure
A systematic review (El-Toukhy et al., 2008) with a meta-analysis of two randomised trials (n = 941) (Demirol and Gurgan, 2004; Rama Raju et al., 2006) demonstrated that office hysteroscopy in the cycle preceding a next IVF attempt nearly doubles the clinical pregnancy rate in infertile patients with at least two failed IVF attempts compared to starting IVF immediately (RR 1.6, 95% CI 1.3-1.9). For every seven infertile women with at least two failed IVF attempts treated by office hysteroscopy prior to a subsequent IVF cycle, it is expected that one additional person will have a clinical pregnancy compared to starting IVF immediately (NNT = 7, 95%CI 5 to12). There is no evidence of significant statistical heterogeneity (Chi² = 0.16; I² = 0%). A subgroup analysis in the patients undergoing office hysteroscopy demonstrated no difference in clinical pregnancy rates irrespective whether pathology was detected and treated or not (RR 0.91, 95% CI 0.71-1.2).
Discussion
The laparoscopic treatment of all visible implants of minimal-mild endometriosis in women with otherwise unexplained subfertility is likely to be beneficial since it might increase the chance of a live birth or ongoing pregnancy. The two major trials do however report conflicting results. A beneficial effect of treating minimal-mild endometriosis is in accordance with the pooled data (Hughes et al., 1993; Adamson and Pasta, 1994) from one pseudo-randomised trial (Nowroozi et al., 1987) and two cohort studies (Fayez et al., 1988; Paulson et al., 1991) but is not confirmed by other observational studies (Seiler et al., 1986; Levinson, 1989; Chong et al., 1990). It should be noted that atypical endometriotic lesions have not been included in the earlier studies. The wider eligibility criteria in the Italian study, namely the longer duration of subfertility and the higher prevalence of more advanced endometriosis could have led to the unintentional inclusion of more patients with a less favourable prognosis, explaining the absent treatment effect in the Italian trial. The results of the Italian trial are more correctly interpreted if one accepts its division into two different subgroups based on whether co-treatment with GnRH agonists was given or not. A type II error due to low statistical power may therefore be responsible for the absence of statistically significant differences between the intervention and control groups. The wider eligibility criteria and the co-treatment with GnRH agonists have caused the substantial statistical heterogeneity in the meta-analysis of the two major trials. The underlying pathophysiological mechanism linking minimal-mild endometriosis to subfertility is still largely unknown. Therefore, controversy still exists whether there is a causal link between these lesions and subfertility (Olive and Schwartz, 1993; Vercellini and Crosignani, 1993). The excision of endometriotic cysts is superior to simple drainage and ablation for increasing the spontaneous conception rate. Some authors have observed that ovarian tissue may be inadvertently excised together with the endometrioma wall in the majority of patients (Muzii et al., 2005), which could lead to a reduction in ovarian volume (Exacoustos et al., 2004). There are many observational studies reporting conflicting results concerning the impact of ovarian cystectomy on the ovarian responsiveness (Yazbeck et al., 2006; Nargund et al., 1996; Loh et al., 1999, Ho et al., 2002; Marconi et al., 2002; Alborzi et al., 2007; Horikawa et al., 2008; Canis et al., 2001; Donnez et al., 2001; Wyns and Donnez, 2003). As a consequence there is uncertainty whether ovarian cystectomy of endometriotic cysts despite its favourable effect in the short term, could have a deleterious impact on the ovarian reserve in the longer term. The absence of a treatment effect in favour of the excision of endometriotic cysts smaller than 6 cm prior to IVF on the pregnancy rates compared to starting IVF immediately is in accordance with the results of an earlier observational study (Garcia-Velasco et al., 2004). In the randomised trial (Demirol, 2006) the trend of lower pregnancy rates after ICSI in the patients who were treated with cystectomy could be explained by the longer stimulation period, a higher gonadotropin requirement and a lower oocyte number: the absence of statistically significant differences due to the low number of included patients cannot enable at the present time to draw definitive conclusions on the need to perform an ovarian cystectomy prior to IVF.
Laparoscopic ovarian diathermy as a second-line treatment in women with clomiphene-resistant PCOS results at least in equal pregnancy rates and decreases the risk for multiple pregnancy compared to gonadotropin treatment, irrespective whether the technique is used uni- or bilaterally . The underlying physiological mechanism of action might be due to both local and systemic effects, resulting in follicular recruitment, maturation and ovulation (Aakvaag 1985; Armar et al., 1990; Balen et al., 1993; Greenblatt and Casper, 1987). It is however unknown how long the treatment effect of LOD lasts, although repeated spontaneous ovulations and subsequent pregnancies after a first pregnancy or miscarriage have been reported (Farquhar et al., 2002). Ovarian adhesions after the LOD procedure have been described, but their clinical relevance is unclear (Greenblatt and Casper, 1993). The theoretical risk of inducing premature ovarian failure needs to be addressed since some observational studies have described a significant reduction of the ovarian reserve after LOD (Weerakiet et al., 2007).
Prior to IVF treatment, the laparoscopic removal of an ultrasonographically visible hydrosalpinx doubles the live birth rate compared to starting IVF immediately. This supports the observed negative impact of tubal infertility due to hydrosalpinx on the implantation rates in IVF treatment (Camus et al., 1999). At the present, there is no evidence to support performing bilateral salpingectomy whether or not bilateral hydrosalpinges are present. The pooled data from two RCTs (Dechaud et al., 1998; Strandell et al., 1999) confirm that salpingectomy for hydrosalpinx prior to IVF is effective before a first IVF treatment cycle. Some observational studies have studied the effect of salpingectomy on the ovarian reserve. One clinical controlled trial demonstrated significantly higher baseline FSH levels after salpingectomy as well as a lower ovarian response to stimulation but the pregnancy rates were similar in both groups (Gelbaya et al., 2006). Another clinical controlled trial equally found higher baseline FSH levels after laparoscopic salpingectomy compared to proximal tubal division but pregnancy rates per patient did not differ between both groups (Nakagawa et al., 2008). The possible long term negative impact of salpingectomy on female fertility should be addressed by future RCTs. Alternatively, the occlusion of a hydrosalpinx is as effective as salpingectomy (Kontoravdis et al., 2006; Moshin and Hotineanu, 2006) whereas the ultrasound-guided transvaginal needle aspiration shows a trend in doubling the clinical pregnancy rate (Hammadieh et al., 2008) but its effect was statistically not significant. The negative impact of a hydrosalpinx on the outcome of IVF is hypothetically explained by the intermittent bathing of the uterine cavity with toxic fluid within the hydrosalpinx, which may lower the endometrial receptivity (Akman et al., 1996; Fleming and Hull, 1996; Freeman et al., 1996; Katz et al., 1996; Strandell et al., 1994) possibly by reducing the endometrial expression of β- integrin (Meyer et al., 1997). Alternative hypothetical mechanisms of action include direct embryo toxicity as demonstrated in a murine model (Mukherjee et al., 1996) or a negative impact on oocyte growth and development during early follicular recruitment (Freeman et al., 1996). Randomised trials studying the effectiveness of tubal surgery compared to expectant management and IVF in terms of livebirth rates are lacking, as has been reported by other authors (Pandian et al., 2008).
The impact of fibroids on fertility remains controversial (Pritts, 2001; Lefebvre et al., 2003; Vilos, 2003; Griffiths et al., 2006; Somigliana et al., 2007; Vimercati et al., 2007; Somigliana et al., 2008; Klatsky et al., 2008; Pritts et al., 2009) despite an abundancy of observational studies (Seoud et al., 1992; Narayan and Goswamy, 1994; Farhi et al., 1995; Lumbiganon et al., 1996; Eldar-Geva et al., 1998; Marshall et al., 1998; Ramzy et al., 1998; Stovall et al., 1998; Bulletti et al., 1999; Bajekal and Li, 2000; Dietterich et al., 2000; Healy, 2000; Hart et al, 2001; Jun et al., 2001; Surrey et al., 2001; Wang et al., 2001; Check et al., 2002; Donnez and Jadoul, 2002; Ng and Ho, 2002; Yarali and Bukulmez, 2002; Bulletti et al., 2004; Manyonda et al., 2004; Oliveira et al., 2004; Parazzini et al., 2004; Wang and Check, 2004; Wise et al., 2004; Benecke et al., 2005; Gianaroli et al., 2005; Ng et al., 2005; Rackow and Arici, 2005; Surrey et al., 2005; Khalaf et al., 2006; Klatsky et al., 2007). Some observational data suggest that submucosal, intramural and subserosal fibroids interfere with female fertility in decreasing order of importance (Somigliana et al., 2007) whereas other non-controlled studies have suggested that the number, size and distorsion effect of fibroids on the uterine cavity may be more important (Bulletti et al., 1999; Varasteh et al., 1999; Bernard et al., 2000; Fernandez et al., 2001; Oliveira et al., 2005, Khalaf et al., 2006; Mukhopadhaya et al., 2007). Fibroids are believed to interfere with sperm migration, ovum transport and embryo implantation (Richards et al., 1998), which may explain why the hysteroscopic removal of submucosal fibroids doubles the clinical pregnancy rates compared to expectant management in women with otherwise unexplained subfertility. Many hypothetical mechanisms have been put forward such as altered contours of the uterine cavity resulting in altered mechanical pressure or abnormal uterine contractility (Bettocchi et al., 2002; Farrugia et al., 2002; Oliveira et al., 2004), local inflammation, focal endometrial vascular disturbances, chronic endometritis, secretion of vasoactive substances or an enhanced intrauterine androgen environment(Richards et al., 1998).
Hysteroscopic polypectomy prior to IUI doubles the pregnancy rates but at the present we cannot recommend the systematic removal of all polyps in subfertile women based on one RCT. Observational studies have suggested a possibly higher impact of tubocornual polyps on female fertility (Venturini et al., 1987; Brooks et al., 1990; Lee et al., 1997; Shokeir et al., 2004; Yanaihara et al., 2008). The effect of the size, number and the localisation of endometrial polyps on fertility should be examined as well as possible association between endometrial polyps and endometriosis (Mc Bean et al., 1996; Kim et al., 2003).
Two randomised trials have confirmed the effectiveness of auto-cross linked hyaluronic acid gel in the prevention of intra-uterine adhesions after hysteroscopic adhesiolysis (Acunzo et al, 2003) and after hysteroscopic surgery (Guida et al., 2004) but have unfortunately failed to present data on the fertility outcome.
The higher pregnancy rates after hysteroscopy even in the absence of intrauterine pathology in women with recurrent IVF failure is an unexpected observation which nevertheless could be explained by the cervical dilatation and/or direct hysteroscopic visualisation of the uterine cavity facilitating embryo transfer (Mc Manus et al., 2000; Mansour and Aboulghar, 2002) or alternatively by an immunological mechanism triggered by the hysteroscopic manipulation or by the effect of the distension medium on the endometrium. The hypothecical immunological mechanism which may similarly explain the increased odds of spontaneous pregnancy after hysterosalpingography (Luttjeboer et al., 2007) is currently under study in an ongoing randomised trial (NCT 00367367) (Geslevich et al., 2006). The results of a registered randomised trial on the effectiveness of hysteroscopy before a first ICSI treatment cycle have not been published yet to the best of our knowledge (NCT 00830401).
We included only randomised trials in this systematic review because this provides the least biased measure of the effectiveness of interventions (Benson and Hartz, 2000; Britton et al., 1998; Concato et al., 2000; McKee et al., 1999; Kunz et al., 2001; Johnson et al., 2008). A recent systematic review of Cochrane reviews on gynaecological surgery demonstrated that the treatment effects tended to be overestimated systematically in trials without allocation concealment, although the difference was not statistically significant (Selman et al., 2008). This finding is consistent with the current understanding of the mechanisms of allocation concealment bias (Kunz and Oxman, 1998). A graphical presentation of the risk of bias of all the included studies is presented in Figure 8. A summary of the risk of bias of all the individual trials included in this systematic review is given in Figure 9. Nearly 75% of all studies have an adequate randomisation sequence generation, while nearly 50% have adequate allocation concealment and less than 20% have adequate blinding. The overall quality of the included trials in the present systematic review is by consequence mediocre. Therefore, we should be cautious in making definitive conclusions. At the present we should refrain from providing guidelines for clinical practice in reproductive surgery. It seems more appropriate to present levels of evidence for the different clinical interventions as illustrated in the summary of the effectiveness of the interventions in Table 2.
8. Risk of bias graph of all included studies.

9. Summary of the risk of bias of individual studies.
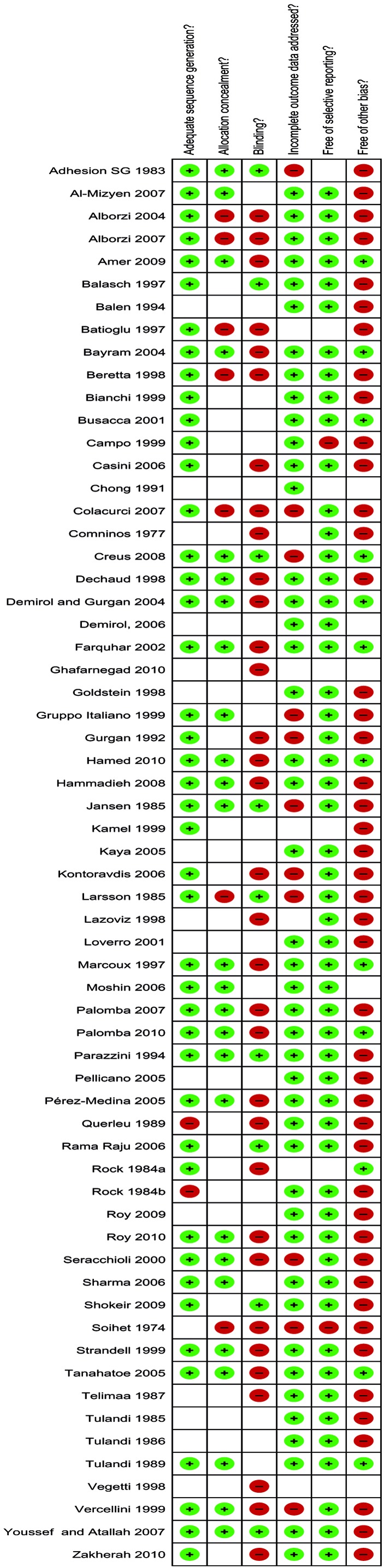
Table 2. Review of the effectiveness of reproductive surgery: levels of evidence.
| topic under review | RCTs | number of participants | conclusions for primary outcomes (evidence category) |
|---|---|---|---|
| Laparoscopic treatment for subfertility associated with rAFS I/II endometriosis |
2 | 437 | Laparoscopic excision/ ablation and adhesiolysis improves the chance for live birth and ongoing pregnancy (E). |
| Treatment of endometriomata by excision or ablation |
2 | 88 | The excision of endometriotic cysts significantly improves the chance for spontaneous conception at 12 months (EG). |
| Treatment of endometriomata prior to IVF |
1 | 99 | There is no evidence of an effect in favor of removing endometriomata prior to IVF (G). |
| Laparoscopic drilling for induction of ovulation in PCOS |
6 | 439 | There is no evidence of a treatment effect of LOD (6-12 months follow-up) versus gonadotropin injections (3-6 cycles) for the ongoing pregnancy rates (EG). |
| 5 | 166 | There are significantly fewer multiple pregnancies with LOD (E). |
|
| 5 | 181 | There is no evidence of an effect of bilateral compared to unilateral LOD (EG). |
|
| Surgical treatment for tubal disease in women with hydrosalpinx due to undergo IVF |
4 | 455 | Laparoscopic salpingectomy for hydrosalpinges prior to IVF significantly improves the chances for pregnancy (all definitions) (E). |
| 2 | 209 | Tubal occlusion is at least as effective as an alternative (EG) | |
| Prevention of adhesions after previous reproductive surgery |
1 | 74 | There is no evidence of a treatment effect for second-look laparoscopy with adhesiolysis in improving pregnancy rates after failed tubal microsurgery(E). |
| 1 | 36 | There is some benefit for the use of hyaluronic acid gel after laparoscopic myomectomy (G). |
|
| Surgical treatment of fibroids for sub-fertility |
2 | 309 | Hysteroscopic myomectomy doubles the pregnancy rate compared to expectant management in subfertile women with submucosal fibroids (EG). |
| 1 | 87 | The removal of intramural or subserosal fibroids tends to increase the pregnancy rate, but the effect is not statistically significant (G). |
|
| Laparoscopy prior to IUI | 1 | 154 | There is no evidence of a treatment effect of laparoscopy prior to IUI (E). |
| Hysteroscopic removal of polyps | 1 | 215 | Hysteroscopic removal of polyps visible on ultrasound increases the pregnancy rates in women undergoing IUI (E). |
| Hysteroscopy in women with IVF failure |
2 | 941 | Hysteroscopy prior to IVF doubles the clinical pregnancy rates in patients with 2 failed IVF attempts (E). |
Most surgical trials will inevitably be at high risk for performance bias resulting from the difficulties with blinding surgeons and patients. Moreover, variation in expertise of surgeons with different surgical procedures is an almost unavoidable confounding variable (Johnson et al., 2008), as well as variation in techniques such as the routine use of anti-adhesive barriers. Nevertheless the future holds promise since gynaecological surgery, in contrast to other surgical specialities is being exposed to the scrutiny of RCTs, following the pioneering pathway of reproductive medicine (Johnson et al., 2003, 2008; Vandekerckhove et al., 1993). Despite the difficulty with the methodology and conduct of RCTs in reproductive surgery, we need to set up adequately powered and pragmatic multicentre randomised trials studying the effectiveness of reproductive surgery versus no treatment or alternative treatment.
Two possible sources of bias in this systematic review should be addressed. Firstly, the filters for the systematic literature search did not include textwords or MeSH terms for endometriosis, fibroids, polyps and tubal pathology. This might have decreased the sensitivity of our search due to the unintentional omission of smaller trials. A second possible source of detection bias is the fact that our group has already published a narrative review on laparoscopy and a systematic review on hysteroscopy in the treatment of infertility (Bosteels et al., 2007, 2010).
An important limitation in the majority of the included trials concerns the choice by the authors to use pregnancy and live birth rates as outcome measures. This is a crude way to assess fertility compared to other parameters such as monthly fecundity rate, cumulative pregnancy rate and time to pregnancy by life table analysis. Future randomised trials on reproductive surgery should not neglect the importance of the time factor in the choice of the most appropriate outcome measure. Moreover, in some clinical settings an ‘expectant management’ group should be used as a control to study the effectiveness of a surgical procedure as proposed by some authors (Hull et al., 1987; Olive et al., 1985).
Summary conclusions and future perspectives
Compared to IVF, reproductive surgery has the potential to restore the natural procreation of the subfertile couple leading to several conceptions after one successful intervention. Repeated success can however only be achieved by effective interventions. A randomised controlled trial is the current gold standard of examining the effectiveness of interventions By consequence, clinical research in the field of reproductive surgery should ideally be guided by high quality randomised trials whenever there is uncertainty about effectiveness of a specific surgical intervention.
The evidence provided by the meta-analysis on treating minimal or mild endometriosis in women with unexplained infertility shows a beneficial effect in favour of the excision/ ablation and adhesiolysis, despite the fact that the two major trials show different results. The long term risks versus benefits ratio in treating infertile patients with endometriotic cysts by the excision technique should be addressed, whether or not in the IVF setting.
The use of IVF for tubal pathology at the expense of reproductive surgery should not be continued without adequate randomised trials studying the harms and benefits of both treatments head-to-head.
We need randomised trials studying the effectiveness of the laparoscopic and/ or hysteroscopic removal of intramural fibroids close to the junctional layer of the myometrium or with impression on the uterine cavity in patients with unexplained subfertility and prior to IUI or IVF treatment.
A trial on the effectiveness of hysteroscopic removal of uterine septa in patients with recurrent pregnancy loss is currently ongoing.
The effectiveness of the anti-adhesion barriers in restoring the normal fertility potential in patients with severe intra-uterine adhesions should be studied by randomised trials.
Before promoting hysteroscopy as a screening tool in the infertile population undergoing ART, we should wait for the results of the randomised trial on the effectiveness of hysteroscopy before a first IVF or IUI attempt.
All future RCTs should focus not only on the beneficial short term effects of the intervention, but should address the possible detrimental long term effects on female fertility. This is the only sound way to measure the ‘true’ effectiveness of a reproductive surgical intervention.
Acknowledgments
The authors are grateful to Jens De Groot from the Biomedical Library Campus Gasthuisberg, Katholieke Universiteit Leuven for his valuable help in the literature search. They acknowledge the assistance of Filip Cools of CEBAM (the Belgian Branch of the Cochrane Collaboration) and of Kris Bogaerts from the Interuniversity Institute for Biostatistics and Statistical Bioinformatics of the Katholieke Universiteit Leuven and Universiteit Hasselt. Language correction was performed by Amanda Sue Mc Phail. Sofie De Wit, Imelda hospital Bonheiden, was responsible for editing the manuscript.
Contributions of the authors
Jan Bosteels was responsible for coordinating research and writing of this manuscript.
Steven Weyers and Thomas D’Hooghe were involved in the selection of studies and the data extraction process.
Chantal Mathieu, Steven Weyers, Thomas D’Hooghe and Ben Willem Mol critically reviewed this systematic review.
No conflict of interest exists for any of the authors. The current work was not funded by any company involved in the manufacture of endoscopes or endoscopic instruments or by a pharmaceutical company.
References
- Aakvaag A. Hormonal response to electrocautery of the ovary in patients with polycystic ovarian disease. Br J Obstet Gynaecol. 1985;92:1258–1264. doi: 10.1111/j.1471-0528.1985.tb04872.x. [DOI] [PubMed] [Google Scholar]
- Acunzo G, Guida M, Pellicano M, et al. Effectiveness of auto-cross linked hyaluronic acid gel in the prevention of intra-uterine adhesions after hysteroscopic adhesiolysis: a prospective, randomised, controlled study. Hum Reprod. 2003;18:1918–1921. doi: 10.1093/humrep/deg368. [DOI] [PubMed] [Google Scholar]
- Adamson GD, Pasta DJ. Surgical treatment of endometriosis- associated infertility: meta-analysis compared with survival analysis. Am J Obstet Gynecol. 1994;171:1488–1505. doi: 10.1016/0002-9378(94)90392-1. [DOI] [PubMed] [Google Scholar]
- Adhesion Study Group , Malinak R, Cleary R. Reduction of postoperative pelvic adhesions with intraperitoneal 32% dextran 70: a prospective, randomised clinical trial. Fertil Steril. 1983;40:612–619. doi: 10.1016/s0015-0282(16)47419-4. [DOI] [PubMed] [Google Scholar]
- Ahmad G, Watson A, Vanderkerckhove P, et al. Techniques for pelvic surgery in subfertility. Cochrane Database Syst Rev. 2009;(issue 1: CD 000221) doi: 10.1002/14651858.CD000221.pub3. [DOI] [PubMed] [Google Scholar]
- Akman MA, Garcia JE, Damewood MD, et al. Hydrosalpinx affects the implantation of previously cryopreserved embryos. Hum Reprod. 1996;11:1013–1014. doi: 10.1093/oxfordjournals.humrep.a019287. [DOI] [PubMed] [Google Scholar]
- Alborzi S, Momtahan M, Parsanezhad ME, et al. A prospective randomised study comparing laparoscopic ovarian cystectomy versus fenestration and coagulation in patients with endometriomas. Fertil Steril. 2004;82:1633–1637. doi: 10.1016/j.fertnstert.2004.04.067. [DOI] [PubMed] [Google Scholar]
- Alborzi S, Ghotbi S, Parsanezhad ME, et al. Pentoxifylline therapy after laparoscopic surgery for different stages of endometriosis: a prospective, double-blind, randomised, placebo-controlled study. J Minim Invasive Gynecol. 2007;14:54–58. doi: 10.1016/j.jmig.2006.06.024. [DOI] [PubMed] [Google Scholar]
- Alborzi S, Ravanbahksh R, Parsanezhad ME, et al. A comparison of follicular response of ovaries to ovulation induction after laparoscopic ovarian cystectomy or fenestration and coagulation versus normal ovaries in patients with endometrioma. Fertil Steril. 2007;88:507–509. doi: 10.1016/j.fertnstert.2006.11.134. [DOI] [PubMed] [Google Scholar]
- Al-Mizyen E, Grudzinskas JG. Unilateral laparoscopic ovarian diathermy in infertile women with clomiphene citrate-resistant polycystic ovary syndrome. Fertil Steril. 2007;88:1678–1680. doi: 10.1016/j.fertnstert.2007.01.060. [DOI] [PubMed] [Google Scholar]
- Amer SA, Li TC, Metwally M, et al. Randomised controlled trial comparing laparoscopic ovarian diathermy with clomiphene citrate as a first-line method of ovulation induction in women with polycystic ovary syndrome. Hum Reprod. 2009;24:219–225. doi: 10.1093/humrep/den325. [DOI] [PubMed] [Google Scholar]
- Ankum WM. Hysteroscopic removal of endometrial polyps more than doubled the pregnancy rate after intrauterine insemination. Evidence-based Obstet Gynecol. 2005;7:193–194. [Google Scholar]
- Armar N, Mc Garrigle H, Honour J, et al. Laparoscopic ovarian diathermy in the management of anovulatory infertility in women with polycystic ovaries: endocrine changes and clinical outcomes. Feril Steril. 1990;53:45–49. doi: 10.1016/s0015-0282(16)53214-2. [DOI] [PubMed] [Google Scholar]
- Bajekal N, Li TC. Fibroids, infertility and pregnancy wastage. Hum Reprod Update. 2000;6:614–620. doi: 10.1093/humupd/6.6.614. [DOI] [PubMed] [Google Scholar]
- Balasch J, Creus M, Fábregues F, et al. Pentoxifylline versus placebo in the treatment of infertility associated with minimal or mild endometriosis: a pilot randomised clinical trial. Hum Reprod. 1997;12:2046–2050. doi: 10.1093/humrep/12.9.2046. [DOI] [PubMed] [Google Scholar]
- Balen A, Tan SL, Jacobs H. Hypersecretion of luteinising hormone. A significant cause of infertility and miscarriage. Br J Obstet Gynecol. 1993;100:1082–1089. doi: 10.1111/j.1471-0528.1993.tb15170.x. [DOI] [PubMed] [Google Scholar]
- Balen A, Jacobs H. A prospective study comparing unilateral and bilateral laparoscopic ovarian diathermy in women with the polycystic ovary syndrome (PCOS) Fertil Steril. 1994;62:921–925. doi: 10.1016/s0015-0282(16)57051-4. [DOI] [PubMed] [Google Scholar]
- Batioglu S, Haberai A, Celikkanat H. Comparison of GnRH agonist administration before and after laparoscopic drainage of endometriomas. J Gynecol Surg. 1997;13:17–21. [Google Scholar]
- Bayram N, van Wely M, Bossuyt P, et al. Abstract 0-148 . 17th Annual Meeting of the ESHRE. Lausanne: Switzerland; 2001. Randomised clinical trial of laparoscopic electrocoagulation of the ovaries versus recombinant FSH for ovulation induction in subfertility associated with polycystic ovary syndrome. [Google Scholar]
- Benecke C, Kruger TF, Siebert TI, et al. Effect of fibroids on fertility in patients undergoing assisted reproduction. A structured literature review. Gynecol Obstet Invest. 2005;59:230. doi: 10.1159/000084513. [DOI] [PubMed] [Google Scholar]
- Benson K, Hartz AJ. A comparison of observational studies and randomised, controlled trials. New Engl J Med. 2000;342:1878–1886. doi: 10.1056/NEJM200006223422506. [DOI] [PubMed] [Google Scholar]
- Beretta P, Franchi M, Ghezzi F, et al. Randomised clinical trial of two laparoscopic treatments of endometriomas: cystectomy versus drainage and coagulation. Fertil Steril. 1998;70:1176–1180. doi: 10.1016/s0015-0282(98)00385-9. [DOI] [PubMed] [Google Scholar]
- Bernard G, Darai E, Poncelet C, et al. Fertility after hysteroscopic myomectomy: effect of intramural fibroids associated. Eur J Obstet Gynecol Reprod Biol. 2000;88:85–90. doi: 10.1016/s0301-2115(99)00123-2. [DOI] [PubMed] [Google Scholar]
- Bettocchi S, Ceci O, Di Venere R, et al. Advanced operative office hysteroscopy without anaesthesia: analysis of 501 cases treated with a 5 Fr bipolar electrode. Hum Reprod. 2002;17:2435–2438. doi: 10.1093/humrep/17.9.2435. [DOI] [PubMed] [Google Scholar]
- Bianchi S, Busacca M, Agnoli B, et al. Effects of 3 month therapy with danazol after laparoscopic surgery for stage III-IV endometriosis: a randomised study. Hum Reprod. 1999;14:1335–1337. doi: 10.1093/humrep/14.5.1335. [DOI] [PubMed] [Google Scholar]
- Bosteels J, van Herendael B, Weyers S, et al. The position of diagnostic laparoscopy in current fertility practice. Hum Reprod Update. 2007;13:477–485. doi: 10.1093/humupd/dmm014. [DOI] [PubMed] [Google Scholar]
- Bosteels J, Weyers S, Puttemans P, et al. The effectiveness of hysteroscopy in improving pregnancy rates in subfertile women without other gynaecological symptoms: a systematic review. Hum Reprod Update. 2010;16(Review):1–11. doi: 10.1093/humupd/dmp033. [DOI] [PubMed] [Google Scholar]
- Britton A, McKee M, Black N, et al. Choosing between randomised and non-randomised studies: a systematic review. Health Technol Asses. 1998;2:13. [PubMed] [Google Scholar]
- Brooks PG, Kerin JF, Daykhovsky L. Removal of cornual polyps with flexible hysteroscopy and a wire basket: a case report. J Reprod Med Obstet Gynecol. 1990;35:613–615. [PubMed] [Google Scholar]
- Bulletti C, De Ziegler D, Polli V, et al. The role of leiomyomas in infertility. J Am Assoc Gynecol Laparosc. 1999;6:441–445. doi: 10.1016/s1074-3804(99)80008-5. [DOI] [PubMed] [Google Scholar]
- Bulletti C, De Ziegler D, Setti PL, et al. Myomas, pregnancy outcome, and in vitro fertilisation. Ann N Y Acad Sci. 2004:84–92. doi: 10.1196/annals.1335.010. [DOI] [PubMed] [Google Scholar]
- Busacca M, Somigliani E, Bianchi S, et al. Postoperative GnRH analogue treatment after conservative surgery for symptomatic endometriosis stage III-IV: a randomised controlled trial. Hum Reprod. 2001;16:2399–2402. doi: 10.1093/humrep/16.11.2399. [DOI] [PubMed] [Google Scholar]
- Campo R, Molinas CR, Rombauts L, et al. Prospective multicentre randomised controlled trial to evaluate factors influencing the success rate of office diagnostic hysteroscopy. Hum Reprod. 2005;20:258–263. doi: 10.1093/humrep/deh559. [DOI] [PubMed] [Google Scholar]
- Campo S, Garcea N. Laparoscopic myomectomy in premenopausal women with and without preoperative treatment using gonadotrophin-releasing hormone analogues. Hum Reprod. 1999;14 doi: 10.1093/humrep/14.1.44. [DOI] [PubMed] [Google Scholar]
- Camus E, Poncelet C, Goffinet F, et al. Pregnancy rates after in- vitro fertilisation in cases of tubal infertility with and without hydrosalpinx: a meta-analysis of published comparative studies. Hum Reprod. 1999;14:1243–1249. doi: 10.1093/humrep/14.5.1243. [DOI] [PubMed] [Google Scholar]
- Canis M, Pouly JL, Tamburro S, et al. Ovarian response during IVF-embryo transfer cycles after laparoscopic ovarian cystectomy for endometriotic cysts of > 3 cm in diameter. Hum Reprod. 2001;16 doi: 10.1093/humrep/16.12.2583. [DOI] [PubMed] [Google Scholar]
- Casini ML, Rossi F, Agostini R, et al. Effect of the position of fibroids on fertility. Gynecol Endocrinol. 2006;22:106–109. doi: 10.1080/09513590600604673. [DOI] [PubMed] [Google Scholar]
- Check JH, Chloe JK, Lee G, et al. The effect on IVF outcome of small intramural fibroids not compressing the uterine cavity as determined by a prospective matched control study. Hum Reprod. 2002;17 doi: 10.1093/humrep/17.5.1244. [DOI] [PubMed] [Google Scholar]
- Chong AP, Keene ME, Thornton NL. Comparison of three modes of treatment for infertility patients with minimal pelvic endometriosis. Fertil Steril. 1990;53:407–410. doi: 10.1016/s0015-0282(16)53331-7. [DOI] [PubMed] [Google Scholar]
- Chong AP. Pregnancy outcome in neosalpingostomy by the cuff vs Bruhat technique using the carbon dioxide laser. J Gynecol Surg. 1991;7:207–210. doi: 10.1089/gyn.1991.7.207. [DOI] [PubMed] [Google Scholar]
- Colacurci N, De Franciscis P, Mollo A, et al. Small-diameter hysteroscopy with Versapoint versus resectoscopy with a unipolar knife for the treatment of septate uterus: a prospective randomised study. J Minim Invas Gynecol. 2007;14:622–627. doi: 10.1016/j.jmig.2007.04.010. [DOI] [PubMed] [Google Scholar]
- Collins A, Burrows EA, Willan AR. The prognosis for live birth among untreated infertile couples. Fertil Steril. 1995;64:22–28. [PubMed] [Google Scholar]
- Comninos AC. Salpingostomy: results of two different methods of treatment. Fertil Steril. 1977;28:1211–1214. [PubMed] [Google Scholar]
- Concato J, Shah N, Horwitz RI. Randomised, controlled trials, observational studies, and the hierarchy of research designs. New Engl J Med. 2000;342:1887–1892. doi: 10.1056/NEJM200006223422507. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Creus M, Fábregues F, Carmona F, et al. Combined laparoscopic surgery and pentoxifylline therapy for treatment of endometriosis-associated infertility: a preliminary trial. Hum Reprod. 2008;23:1910–1916. doi: 10.1093/humrep/den167. [DOI] [PubMed] [Google Scholar]
- De Angelis C, Santoro G, Re ME, et al. Office hysteroscopy and compliance: mini- hysteroscopy versus traditional hysteroscopy in a randomised trial. Hum Reprod. 2003;18:2441–2445. doi: 10.1093/humrep/deg463. [DOI] [PubMed] [Google Scholar]
- Dechaud H, Daures JP, Arnal F, et al. Does previous salpingectomy improve implantation and pregnancy rates in patients with severe tubal factor infertility who are undergoing in vitro fertilization? A pilot prospective randomized study. Fertil Steril. 1998;69:1020–1025. doi: 10.1016/s0015-0282(98)00077-6. [DOI] [PubMed] [Google Scholar]
- Demirol A. Effect of endometrioma cystectomy on IVF outcome: a prospective randomised study. Reprod Biomed Online. 2006;12:639–643. doi: 10.1016/s1472-6483(10)61192-3. [DOI] [PubMed] [Google Scholar]
- Demirol A, Gurgan T. Effect of treatment of intrauterine pathologies with office hysteroscopy in patients with recurrent IVF failure. Reprod Biomed Online. 2004;8:590–594. doi: 10.1016/s1472-6483(10)61108-x. [DOI] [PubMed] [Google Scholar]
- De Placido G, Clarizia R, Cadente C, et al. Compliance and diagnostic efficacy of mini-hysteroscopy versus traditional hysteroscopy in infertility investigation. Eur J Obstet Gynecol. 2007;135:83–87. doi: 10.1016/j.ejogrb.2007.02.028. [DOI] [PubMed] [Google Scholar]
- Dickersin K, Scherer R, Lefebvre C. Identifying relevant studies for systematic reviews. BMJ. 1994;309:1286–1291. doi: 10.1136/bmj.309.6964.1286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dietterich C, Check JH, Choe JK, et al. The presence of small uterine fibroids not distorting the endometrial cavity does not adversely affect conception outcome following embryo transfer in older recipients. Clin Exp Obstet Gynecol. 2000;27:168–170. [PubMed] [Google Scholar]
- Donnez J, Wyns C, Nisolle M. Does ovarian surgery for endometriomas impair the ovarian response to gonadotropins? Fertil Steril. 2001;76:662–665. doi: 10.1016/s0015-0282(01)02011-8. [DOI] [PubMed] [Google Scholar]
- Donnez J, Jadoul P. What are the implications of myomas in fertility? A need for a debate? Hum Reprod. 2002;17 doi: 10.1093/humrep/17.6.1424. [DOI] [PubMed] [Google Scholar]
- Duffy JMN, Johnson N, Ahmad G, et al. Postoperative procedures for improving fertility following pelvic reproductive surgery. Cochrane Database Syst Rev. 2009;(issue 2:CD 001897) doi: 10.1002/14651858.CD001897.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Geva T, Meagher S, Healy DL, et al. Effect of intramural, subserosal, and submucosal uterine fibroids on the outcome of assisted reproductive technology treatment. Fertil Steril. 1998;70:687–691. doi: 10.1016/s0015-0282(98)00265-9. [DOI] [PubMed] [Google Scholar]
- Toukhy T, Sunkara SK, Coomarasamy A, et al. Outpatient hysteroscopy and subsequent IVF cycle outcome: a systematic review and meta-analysis. RBM Online. 2008;16:712–719. doi: 10.1016/s1472-6483(10)60486-5. [DOI] [PubMed] [Google Scholar]
- Exacoustos C, Zupi E, Amadio A, et al. Laparoscopic removal of endometriomas: sonographic evaluation of residual functioning ovarian tissue. Am J Obstet Gynecol. 2004;191:68–72. doi: 10.1016/j.ajog.2004.01.010. [DOI] [PubMed] [Google Scholar]
- Farhi J, Ashkenazi J, Feldberg D, et al. Effect of uterine leiomyomata on the results of in-vitro fertilisation treatment. Hum Reprod. 1995;10:2576–2578. doi: 10.1093/oxfordjournals.humrep.a135748. [DOI] [PubMed] [Google Scholar]
- Farrugia M, McGurgan P, McMillan DL, et al. London: Greenwich Medical Media; 2002. Recent advances in electrosurgery (Chap 18) [Google Scholar]
- Farquhar CM, Williamson K, Gudex G, et al. A randomised controlled trial of laparoscopic ovarian diathermy versus gonadotrophin therapy for women with clomiphene-resistant polycystic ovarian syndrome. Fertil Steril. 2002;78:404–411. doi: 10.1016/s0015-0282(02)03225-9. [DOI] [PubMed] [Google Scholar]
- Farquhar C, Lilford R, Marjoribanks J, et al. Laparoscopic ‘drilling’ by diathermy or laser for ovulation induction in anovulatory polycystic ovary syndrome. Cochrane Database Syst Rev. 2009;(issue 1:CD 001122) [Google Scholar]
- Fatum M, Laufer N, Simon A. Investigation of the infertile couple: should diagnostic laparoscopy be performed after normal hysterosalpingography in treating infertility suspected to be of unknown origin? Hum Reprod. 2002;17 doi: 10.1093/humrep/17.1.1. [DOI] [PubMed] [Google Scholar]
- Fayez JA, Collazo LM, Vernon C. Comparison of different modalities of treatment for minimal and mild endometriosis. Am J Obstet Gynecol. 1988;159:927–932. doi: 10.1016/s0002-9378(88)80173-x. [DOI] [PubMed] [Google Scholar]
- Fernandez H, Sefrioui O, Virelizier C, et al. Hysteroscopic resection of submucosal fibroids in patients with infertility. Hum Reprod. 2001;16:1489–1492. doi: 10.1093/humrep/16.7.1489. [DOI] [PubMed] [Google Scholar]
- Forman RG, Robinson JN, Mehta Z, et al. Patient history as a simple predictor of pelvic pathology in subfertile women. Hum Reprod. 8:53–55. doi: 10.1093/oxfordjournals.humrep.a137873. [DOI] [PubMed] [Google Scholar]
- Freeman MR, Withworth CM, Hill GA, et al. Hydrosalpinx reduces in vitro fertilisation/ embryo transfer rates and in vitro blastocyst development. 52nd Annual Meeting of the American Fertility Society. 1996:S211. [Google Scholar]
- Garbin O, Kutnahorsky R, Göllner JL, et al. Vaginoscopic versus conventional approaches to outpatient diagnostic hysteroscopy: a two-centre randomised prospective study. Hum Reprod. 2006;21:996–3000. doi: 10.1093/humrep/del276. [DOI] [PubMed] [Google Scholar]
- GArcia-Velasco JA, Mahutte NG, Corona J, et al. Removal of endometriomas before in vitro fertilization does not improve fertility outcomes: a matched, case-control study. Fertil Steril. 2004;81:1194–1197. doi: 10.1016/j.fertnstert.2003.04.006. [DOI] [PubMed] [Google Scholar]
- Gelbaya TA, Nardo LG, Fitzgerald CT, et al. Ovarian response to gonadotropins after laparoscopic salpingectomy or the division of fallopian tubes for hydrosalpinges. Fertil Steril. 2006;85:1464–1468. doi: 10.1016/j.fertnstert.2005.10.036. [DOI] [PubMed] [Google Scholar]
- Geslevich J, Weiss A, Romano S, et al. Endometrial curettage before embryotransfer. http://www.controlled-trials.com/mrct/trial/185361/ hysteroscopy 2006;( NCT00367367) [Google Scholar]
- Ghafarnegad M, Arjmand N, Khazaeipour Z. Pregnancy rate of gonadotrophin therapy and laparoscopic ovarian electrocautery in polycystic ovary syndrome resistant to clomiphene citrate: A comparative study. Tehran Uni Med J. 2010;67:712–717. [Google Scholar]
- Gianaroli L, Gordts S, Angelo A, et al. Effect of inner myometrium fibroid on reproductive outcome after IVF. Reprod Biomed Online. 2005;10:473–477. doi: 10.1016/s1472-6483(10)60823-1. [DOI] [PubMed] [Google Scholar]
- Glanville JM, Lefebvre C, Miles JN, et al. How to identify randomised controlled trials in MEDLINE: ten years on. J Med Libr Assoc. 2006;94:130–136. [PMC free article] [PubMed] [Google Scholar]
- Goldstein DB, Sasaran LH, Stadtmauer L, et al. Selective salpingostomy- salpingectomy (SSS) and medical treatment prior to IVF in patients with hydrosalpinx. Fertil Steril. 1998;70:S320. [Google Scholar]
- Greenblatt E, Casper RF. Endocrine changes after laparoscopic ovarian cautery in polycystic ovarian syndrome. Am J Obstet Gynecol. 1987;156:279–285. doi: 10.1016/0002-9378(87)90268-7. [DOI] [PubMed] [Google Scholar]
- Greenblatt E, Casper RF. Adhesion formation after laparoscopic ovarian cautery for polycystic ovarian syndrome: lack of correlation with pregnancy rate. Fertil Steril. 1993;60:766–770. [PubMed] [Google Scholar]
- Griffiths AN, Angelo A, Amso NN. Surgical treatment of fibroids for subfertility. Cochrane Database Syst Rev. 2009;(issue 1:CD 003857) doi: 10.1002/14651858.CD003857.pub2. [DOI] [PubMed] [Google Scholar]
- Gruppo Italiano per lo Studio dell'Endometriosi'. Ablation of lesions or no treatment in minimal-mild endometriosis in infertile women: a randomised trial. Hum Reprod. 1999;14:1332–1334. doi: 10.1093/humrep/14.5.1332. [DOI] [PubMed] [Google Scholar]
- Guida M, Pellicano M, Zullo F, et al. Outpatient operative hysteroscopy with bipolar electrode: a prospective multicentre randomised study between local anaesthesia and conscious sedation. Hum Reprod. 2003;18:840–843. doi: 10.1093/humrep/deg075. [DOI] [PubMed] [Google Scholar]
- Guida M, Acunzo G, Di Spiezio Sardo A, et al. Effectiveness of auto-cross linked hyaluronic acid gel in the prevention of intra-uterine adhesions after hysteroscopic surgery: a prospective, randomised, controlled study. Hum Reprod. 2004;19:1461–1464. doi: 10.1093/humrep/deh238. [DOI] [PubMed] [Google Scholar]
- Guida M, Di Spiezio Sardo A, Acunzo G, et al. Vaginoscopic versus traditional office hysteroscopy: a randomised controlled study. Hum Reprod. 2006;21:3253–3257. doi: 10.1093/humrep/del298. [DOI] [PubMed] [Google Scholar]
- Gurgan T, Urman B, Aksu T, et al. The effect of short-interval laparoscopic lysis of adhesions on pregnancy rates following Nd-YAG laser photocoagulation of polycystic ovaries. Obstet Gynecol. 1992;80:45–47. [PubMed] [Google Scholar]
- Hamed HO, Hasan AF, Ahmed OG, et al. Metformin versus laparoscopic ovarian drilling in clomiphene- and insulin-resistant women with polycystic ovary syndrome. Int J Gynecol Obstet. 2010;108:143–147. doi: 10.1016/j.ijgo.2009.08.033. [DOI] [PubMed] [Google Scholar]
- Hammadieh N, Coomarasamy Y, Ola B, et al. Ultrasound-guided hydrosalpinx aspiration during oocyte collection improves pregnancy outcome in IVF: a randomized controlled trial. Hum Reprod. 2008;23:1113–1117. doi: 10.1093/humrep/den071. [DOI] [PubMed] [Google Scholar]
- Hart R, Khalaf Y, Yeong CT, et al. A prospective controlled study of the effect of intramural uterine fibroids on the outcome of assisted conception. Hum Reprod. 2001;16:2411–2417. doi: 10.1093/humrep/16.11.2411. [DOI] [PubMed] [Google Scholar]
- Hart RJ, Hickey M, Maouris P, et al. Excisional surgery versus ablative surgery for ovarian endometriomata. Cochrane Database Syst Rev. 2005 doi: 10.1002/14651858.CD004992.pub2. [DOI] [PubMed] [Google Scholar]
- Haynes RB, Wilczynski N, Mc Kibbon KA, et al. Developing optimal search strategies for detecting clinically sound studies in MEDLINE. J Am Med Inform Assoc. 1994;1:447–458. doi: 10.1136/jamia.1994.95153434. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Healy DL. Impact of uterine fibroids on ART outcome. Environ Health Perspect. 2000;108:845–847. doi: 10.1289/ehp.00108s5845. [DOI] [PubMed] [Google Scholar]
- Ho HY, Lee RK, Hwu YM, et al. Poor response of ovaries with endometrioma previously treated with cystectomy. J Assist Reprod Genet. :507–511. doi: 10.1023/A:1020970417778. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Horikawa T, Nakagawa K, Ohgi S, et al. The frequency of ovulation from the affected ovary decreases following laparoscopic cystectomy in infertile women with unilateral endometrioma during a natural cycle. J Assist Reprod Genet. 2008:239–244. doi: 10.1007/s10815-008-9229-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hughes EG, Fedorkow DM, Collins JA. A quantitative overview of controlled trials in endometriosis- associated infertility. Fertil Steril. 1993;59:963–970. [PubMed] [Google Scholar]
- Hull ME, Moghissi KS, Magyar DF, et al. Comparison of different treatment modalities of endometriosis in infertile women. Fertil Steril. 1987;47:40–44. [PubMed] [Google Scholar]
- Jacobson TZ, Duffy JMN, Barlow D, et al. Laparoscopic surgery for subfertility associated with endometriosis. Cochrane Database Syst Rev. 2010;(issue 1:CD001398) doi: 10.1002/14651858.CD001398.pub2. [DOI] [PubMed] [Google Scholar]
- Jansen RPS. Failure of intraperitoneal adjuncts to improve the outcome of pelvic operations in young women. Am J Obstet Gynecol. 1985;153:363–371. doi: 10.1016/0002-9378(85)90072-9. [DOI] [PubMed] [Google Scholar]
- Johnson N, Proctor M, Farquhar C. Gaps in the evidence for fertility treatment-an analysis of the Cochrane Menstrual Disorders and Subfertility Group database. Hum Reprod. 2003;18:947–954. [PubMed] [Google Scholar]
- Johnson N, Selman T, Zamora J, et al. Gynaecologic surgery from uncertainty to science: evidence-based surgery is no passing fad. Hum Reprod. 2008;23:832–839. doi: 10.1093/humrep/dem423. [DOI] [PubMed] [Google Scholar]
- Johnson N, van Voorst S, Sowter MC, et al. Surgical treatment for tubal disease in women due to undergo in vitro fertilisation. Cochrane Database Syst Rev. 2010;(issue 1:CD 002125) doi: 10.1002/14651858.CD002125.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jun SH, Ginsburg ES, Racowsky C, et al. Uterine leiomyomas and their effect on in vitro fertilisation outcome: a retrospective study. J Assist Reprod Genet. 2001;18:139–143. doi: 10.1023/A:1009403819377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kabli N, Tulandi T. A randomised trial of outpatient hysteroscopy with and without intrauterine anaesthesia. 2008;15:308–310. doi: 10.1016/j.jmig.2008.01.013. [DOI] [PubMed] [Google Scholar]
- Kamel MA, Amin AF. Using thermocoagulation versus electrocoagulation in laparoscopic adhesiolysis in infertility treatment. Hum Reprod. 1999;14(Abstract Book I, Abstract of 15th Annual Meeting of ESHRE, Tours, France):276–277. [Google Scholar]
- Katz E, Akman MA, Damewood MD, et al. Deleterious effect of the presence of hydrosalpinx on implantation and pregnancy rates with in vitro fertilisation. Fertil Steril. 1996;66:122–125. doi: 10.1016/s0015-0282(16)58398-8. [DOI] [PubMed] [Google Scholar]
- Kaya H, Sezik M, Ozkaya O. Evaluation of a new surgical approach for the treatment of clomiphene citrate-resistant infertility in polycystic ovary syndrome: Laparoscopic ovarian multi-needle intervention. J Minim Invasive Gynaecol. 2005;12:355–358. doi: 10.1016/j.jmig.2005.05.017. [DOI] [PubMed] [Google Scholar]
- Kennedy S, Bergqvist A, Chapron C, et al. ESHRE guidelines for the diagnosis and treatment of endometriosis. Hum Reprod. 2005;20:2698–2704. doi: 10.1093/humrep/dei135. [DOI] [PubMed] [Google Scholar]
- Khalaf Y, Ross C, Toukhy T, et al. The effect of small intramural uterine fibroids on the cumulative outcome of assisted conception. Hum Reprod. 2006;21:2640–2644. doi: 10.1093/humrep/del218. [DOI] [PubMed] [Google Scholar]
- Kim MR, Kim YA, Jo MY, et al. High frequency of endometrial polyps in endometriosis. J Am Assoc Gynecol Laparosc. 2003;10:46–48. doi: 10.1016/s1074-3804(05)60233-2. [DOI] [PubMed] [Google Scholar]
- Klatsky PC, Lane DE, Ryan IP, et al. The effect of fibroids without cavity involvement on ART outcomes independent of ovarian age. Hum Reprod. 2007;22:521–526. doi: 10.1093/humrep/del370. [DOI] [PubMed] [Google Scholar]
- Klatsky PC, Tran ND, Caughey AB, et al. Fibroids and reproductive outcomes: a systematic literature review from conception to delivery. Am J Obstet Gynecol. 2008;198:357–366. doi: 10.1016/j.ajog.2007.12.039. [DOI] [PubMed] [Google Scholar]
- Kontoravdis A, Makrakis E, Pantos K, et al. Proximal tubal occlusion and salpingectomy result in similar improvement in in vitro fertilization outcome in patients with hydrosalpinx. Fertil Steril. 2006;86:1642–1649. doi: 10.1016/j.fertnstert.2006.05.032. [DOI] [PubMed] [Google Scholar]
- Kremer C, Duffy S, Moroney M. Patient satisfaction with outpatient hysteroscopy versus day case hysteroscopy: randomised controlled trial. BMJ. 2000;320:279–282. [PMC free article] [PubMed] [Google Scholar]
- Kunz R, Vist G, Oxman AD. The Cochrane Library, issue 3. Chichester, UK: John Wiley & Sons; 2004. Randomisation to protect against selection bias in health care trials (Cochrane Methodology Review). Updated 22 Aug. 2001. [Google Scholar]
- Kunz R, Oxman A. The unpredictability paradox: review of empirical comparisons of randomised and non-randomised clinical trials. 1998;317:1185–1190. doi: 10.1136/bmj.317.7167.1185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Larsson B, Lalos O, Marsk L, et al. Effect of intraperitoneal instillation of 32% dextran 70 on postoperative adhesion formation after tubal surgery. Acta Obstet Gynecol Scand. 1985;64:437–441. doi: 10.3109/00016348509155163. [DOI] [PubMed] [Google Scholar]
- Lazovic G, Milacic D, Terzic M, et al. Medicaments or surgical therapy of PCOS. Fertil Steril. 1998;70:472. [Google Scholar]
- Lee A, Ying YK, Novy MJ. Hysteroscopy, hysterosalpingography and tubal ostial polyps in infertility patients. J Reprod Med Obstet Gynecol. 1997;42:337–341. [PubMed] [Google Scholar]
- Lefebvre G, Vilos G, Allaire C, Jeffrey J. The management of uterine leiomyomas. J Obstet Gynecol Can. 2003;25:396–405. [PubMed] [Google Scholar]
- Levinson CJ. Endometriosis therapy: rationale for expectant or minimal therapy in minimal/ mild cases (AFSI) Proceedings of the Second World Congress on Gynecologic Endoscopy, Clermont-Ferrand, France. 1989;(abstract) [Google Scholar]
- Litta P, Bonora M, Pozzan C, et al. Carbon dioxide versus normal saline in outpatient hysteroscopy. Hum Reprod. 2003;18:2446–2449. doi: 10.1093/humrep/deg465. [DOI] [PubMed] [Google Scholar]
- Littman E, Giudice L, Lathi R, et al. Role of laparoscopic treatment of endometriosis in patients with failed in vitro fertilization cycles. Fertil Steril. 2005;84:1574–1578. doi: 10.1016/j.fertnstert.2005.02.059. [DOI] [PubMed] [Google Scholar]
- Loh FH, Tan AT, Kumar J, et al. Ovarian response after laparoscopic ovarian cystectomy for endometrotic cysts in 132 monitored cycles. Fertil Steril. 1999;72:316–321. doi: 10.1016/s0015-0282(99)00207-1. [DOI] [PubMed] [Google Scholar]
- Loverro G, Santillo V, Pansini MV, et al. Are GnRH agonists helpful in the therapy of endometriosis after surgical treatment? 2001;16:96. [Google Scholar]
- Lumbiganon P, Rugpao S, fung S, et al. Protective effect of depot-medroxyprogesterone acetate on surgically treated uterine leiomyomas: a multicentre case-control study. Br J Obstet Gynaecol. 1996;103 doi: 10.1111/j.1471-0528.1996.tb09911.x. [DOI] [PubMed] [Google Scholar]
- Luttjeboer F, Harada T, Hughes E, et al. Tubal flushing for subfertility. Cochrane Database Syst Rev. 2007;(CD 003718) doi: 10.1002/14651858.CD003718.pub3. [DOI] [PubMed] [Google Scholar]
- Mansour R, Aboulghar M. Optimizing the embryotransfer technique. Hum Reprod. 2002;17:1149–1153. doi: 10.1093/humrep/17.5.1149. [DOI] [PubMed] [Google Scholar]
- Manyonda I, Sinthamoney E, Belli M. Controversies and challenges in the modern management of uterine fibroids. BJOG. 2004;111:95. doi: 10.1046/j.1471-0528.2003.00002.x. [DOI] [PubMed] [Google Scholar]
- Marconi G, Vilela M, Quintana R, et al. Laparoscopic ovarian cystectomy of endometrioma does not affect the ovarian response to gonadotropin stimulation. Fertil Steril. 2002;78:876–878. doi: 10.1016/s0015-0282(02)03326-5. [DOI] [PubMed] [Google Scholar]
- Marcoux S, Maheux R, Bérubé S, et al. Laparoscopic surgery in infertile women with minimal or mild endometriosis. N Engl J Med. 1997;337:217–222. doi: 10.1056/NEJM199707243370401. [DOI] [PubMed] [Google Scholar]
- Marsh F, Kremer C, Duffy S. Delivering an effective outpatient service in gynaecology. A randomised controlled trial analysing the cost of outpatient versus daycase hysteroscopy. 2004;111:243–248. doi: 10.1111/j.1471-0528.2004.00064.x. [DOI] [PubMed] [Google Scholar]
- Marshall LM, Spiegelman D, Goldman MB, et al. A prospective study of reproductive factors and oral contraceptive use in relation to the risk of uterine leiomyomata. Fertil Steril. 1998;70:432–439. doi: 10.1016/s0015-0282(98)00208-8. [DOI] [PubMed] [Google Scholar]
- McBean JH, Gibson M, Brumsted JR. The association of intrauterine filling defects on hysterosalpingogram with endometriosis. Fertil Steril. 1996;66:522–526. doi: 10.1016/s0015-0282(16)58562-8. [DOI] [PubMed] [Google Scholar]
- McKee M, Britton A, Black N, et al. Methods in health services research. Interpreting the evidence: choosing between randomised and non-randomised studies. BMJ. 1999;319:312–315. doi: 10.1136/bmj.319.7205.312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McManus J, McClure N, Traub AI. The effect of cervical dilatation in patients with previous difficult embryo transfer. Fertil Steril. 2000;74:159. [Google Scholar]
- Metwally M, Watson A, Lilford R, et al. Fluid and pharmacological agents for adhesion prevention after gynaecological surgery. Cochrane Database Syst Rev. 2006;(issue 2:CD 001298) doi: 10.1002/14651858.CD001298.pub3. [DOI] [PubMed] [Google Scholar]
- Meyer WR, Castelbaum AJ, Somkuti S, et al. Hydrosalpinges adversely affect markers of endometrial receptivity. Hum Reprod. 1997;12:1393–1398. doi: 10.1093/humrep/12.7.1393. [DOI] [PubMed] [Google Scholar]
- Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339(doi: 10.1136/bmj.b2535):b2535. doi: 10.1136/bmj.b2535. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mol BW, Collins JA, Burrows EA, et al. Comparison of hysterosalpingography and laparoscopy in predicting fertility outcome. 1999;14:1237–1242. doi: 10.1093/humrep/14.5.1237. [DOI] [PubMed] [Google Scholar]
- Moshin V, Hotineanu A. Reproductive outcome of the proximal occlusion prior to IVF in patients with hydrosalpinx. Hum Reprod. 2006;21 [Google Scholar]
- Mukherjee T, Copperman AB, McCaffrey C, et al. Hydrosalpinx fluid has direct embryotoxic effects on murine embryogenesis: a case for prophylactic salpingectomy. Fertil Steril. 1996;66:851–853. doi: 10.1016/s0015-0282(16)58652-x. [DOI] [PubMed] [Google Scholar]
- Mukhopadhaya N, Pokuah Asante G, Manyonda IT. Uterine fibroids: impact on fertility and pregnancy loss. Obstet Gynecol Reprod Med. 2007;17:311–317. [Google Scholar]
- Muzii L, Bellati F, Bianchi A, et al. Laparoscopic stripping of endometriomas: a randomized trial on different surgical techniques. Part I: Clinical results. Hum Reprod. 2005;20:1981–1986. doi: 10.1093/humrep/dei007. [DOI] [PubMed] [Google Scholar]
- Muzii L, Bellati F, Bianchi A, et al. Laparoscopic stripping of endometriomas: a randomized trial on different surgical techniques. Part II: pathological results. Hum Reprod. 2005;20:1987–1992. doi: 10.1093/humrep/deh851. [DOI] [PubMed] [Google Scholar]
- Nakagawa K, Ohgi S, Nakashima A, et al. Laparoscopic proximal tubal division can preserve ovarian reserve for infertility patients with hydrosalpinges. J Obstet Gynaecol Res. 2008;34:1037–1042. doi: 10.1111/j.1447-0756.2008.00801.x. [DOI] [PubMed] [Google Scholar]
- Narayan R, Goswamy RK. Treatment of submucous fibroids, and outcome of assisted reproduction. J Am Assoc Gynecol Laparosc. 1994;1:307–311. doi: 10.1016/s1074-3804(05)80793-5. [DOI] [PubMed] [Google Scholar]
- Nargund G, Cheng WC, Parsons J. The impact of ovarian cystectomy on ovarian response to stimulation during in-vitro fertilization cycles. Hum Reprod. 1996;11:81–83. doi: 10.1093/oxfordjournals.humrep.a019043. [DOI] [PubMed] [Google Scholar]
- Ng EH, Ho PC. Doppler ultrasound examination of uterine arteries on the day of oocyte retrieval in patients with uterine fibroids undergoing IVF. Hum Reprod. 2002;17:765–770. doi: 10.1093/humrep/17.3.765. [DOI] [PubMed] [Google Scholar]
- Ng EH, Chan CC, Tang OS, et al. Endometrial and subendometrial blood flow measured by three-dimensional power Doppler ultrasound in patients with small intramural uterine fibroids during IVF treatment. Hum Reprod. 2005;20:501–506. doi: 10.1093/humrep/deh594. [DOI] [PubMed] [Google Scholar]
- Nowroozi K, Chase JS, Check JH, et al. The importance of laparoscopic coagulation of mild endometriosis in infertile women. Int J Fertil. 1987;32:442–444. [PubMed] [Google Scholar]
- Olive DL, Stohs GF, Metzger DA, et al. Expectant management and hydrotubations in the treatment of endometriosis-associated infertility. Fertil Steril. 1985;44:35–41. doi: 10.1016/s0015-0282(16)48674-7. [DOI] [PubMed] [Google Scholar]
- Olive DL, Schwartz LB. Endometriosis. N Engl J Med. 1993;328:1759–1769. doi: 10.1056/NEJM199306173282407. [DOI] [PubMed] [Google Scholar]
- Oliveira FG, Abdelmassih VG, Diamond MP, et al. Impact of subserosal and intramural uterine fibroids that do not distort the endometrial cavity on the outcome of in vitro fertilisation-intracytoplasmic sperm injection. Fertil Steril. 2004;81:582–587. doi: 10.1016/j.fertnstert.2003.08.034. [DOI] [PubMed] [Google Scholar]
- Oliveira FG, Abdelmassih VG, Diamond MP MP, et al. Small uterine fibroids did not negatively affect the success of infertility treatment with intracytoplasmic sperm injection. Evidence-based Obstet Gynecol. 2005;7:31–32. [Google Scholar]
- Pabuccu R, Onalan G, Kaya C, et al. Efficiency and pregnancy outcome of serial intra-uterine device-guided hysteroscopic adhesiolysis of intra-uterine synechia. Fertil Steril. 2008;90:1973–1977. doi: 10.1016/j.fertnstert.2007.06.074. [DOI] [PubMed] [Google Scholar]
- Palomba S, Zupi E, Falbo A, et al. A multicenter randomised, controlled study comparing laparoscopic versus minilaparotomic myomectomy: reproductive outcomes. Fertil Steril. 2007;88:933–941. doi: 10.1016/j.fertnstert.2006.12.047. [DOI] [PubMed] [Google Scholar]
- Palomba S, Falbo A, Battista L, et al. Laparoscopic ovarian diathermy vs clomiphene citrate plus metformin as second-line strategy for infertile anovulatory patients with polycystic ovary syndrome: a randomised controlled trial. Am J Obstet Gynecol. 2010;202(e1-8. Epub 2010 Jan 22):577. doi: 10.1016/j.ajog.2009.11.042. [DOI] [PubMed] [Google Scholar]
- Pandian Z, Akande VA, Harrild K, et al. Surgery for tubal infertility. Cochrane Database Syst Rev. 2008;(issue 3:CD 006415) doi: 10.1002/14651858.CD006415.pub2. [DOI] [PubMed] [Google Scholar]
- Parazzini F, Fedele L, Busacca M, et al. Postsurgical medical treatment of advanced endometriosis: Results of a randomised clinical trial. 1994;171:1205–1207. doi: 10.1016/0002-9378(94)90133-3. [DOI] [PubMed] [Google Scholar]
- Parazzini F, Chiaffarino F, Polverino G, et al. Uterine fibroids risk and history of selected medical conditions linked with female hormones. Eur J Epidemiol. 2004;19:249–253. doi: 10.1023/b:ejep.0000020448.43323.2a. [DOI] [PubMed] [Google Scholar]
- Paulson JD, Asmar P, Saffan DS. Mild and moderate endometriosis: comparison of treatment modalities for infertile couples. J Reprod Med. 1991;36:151–155. [PubMed] [Google Scholar]
- Pellicano M, Guida M, Zullo F, et al. Carbon dioxide versus normal saline as a uterine distension medium for diagnostic vaginoscopic hysteroscopy in infertile patients: a prospective, randomised, multicenter study. 2003;79:418–421. doi: 10.1016/s0015-0282(02)04681-2. [DOI] [PubMed] [Google Scholar]
- Pellicano M, Guida M, Bramante S, et al. Reproductive outcome after autocrosslinked hyaluronic acid gel application in infertile patients who underwent laparoscopic myomectomy. Fertil Steril. 2005;83:498–500. doi: 10.1016/j.fertnstert.2004.09.019. [DOI] [PubMed] [Google Scholar]
- Medina T, Arenas J, Salazar F, et al. Endometrial polyps and their implication in the pregnancy rates of patients undergoing intrauterine insemination: a prospective randomised study. Hum Reprod. 2005;20:1632–1635. doi: 10.1093/humrep/deh822. [DOI] [PubMed] [Google Scholar]
- Pritts EA. Fibroids and infertility: a systematic review of the evidence. Obstet Gynecol Surv. 2001;56:483–491. doi: 10.1097/00006254-200108000-00022. [DOI] [PubMed] [Google Scholar]
- Pritts EA, Parker WH, Olive DL. Fibroids and infertility: an updated systematic review of the evidence. Fertil Steril. 2009;91:1215–1223. doi: 10.1016/j.fertnstert.2008.01.051. [DOI] [PubMed] [Google Scholar]
- Querleu D, Deffense F, Bouteville C. The effect of noxytioline and systemic corticosteroids in infertility surgery. A prospective randomised study. J Gynecol Obstet Biol Reprod. 1989;18:935–940. [PubMed] [Google Scholar]
- Rackow BW, Arici A. Fibroids and in-vitro fertilisation: which comes first? Curr Opin Obstet Gynecol. 2005;15:225–231. doi: 10.1097/01.gco.0000169097.52848.ee. [DOI] [PubMed] [Google Scholar]
- Rama Raju GA, Shashi Kumari G, Krishna KM, et al. Assessment of uterine cavity by hysteroscopy in assisted reproduction programme and its influence on pregnancy outcome. Arch Gynecol Obstet. 2006;274:160–164. doi: 10.1007/s00404-006-0174-7. [DOI] [PubMed] [Google Scholar]
- Ramzy AM, Sattar M, Amin Y, et al. Uterine myomata and outcome of assisted reproduction. Hum Reprod. 1998;13:198–202. doi: 10.1093/humrep/13.1.198. [DOI] [PubMed] [Google Scholar]
- Richards PA, Richards PD, Tiltman AJ. The ultrastructure of fibromyomatous myometrium and its relationship to infertility. Hum Reprod Update. 1998;4:520–525. doi: 10.1093/humupd/4.5.520. [DOI] [PubMed] [Google Scholar]
- Robinson KA, Dickersin K. Development of a highly sensitive search strategy for the retrieval of reports of controlled trials using PubMed. Int J Epidemiol. 2002;31:150–153. doi: 10.1093/ije/31.1.150. [DOI] [PubMed] [Google Scholar]
- Rock JA, Siegler AM, Meisel M, et al. The efficacy of postoperative hydrotubation: a randomised prospective multicenter clinical trial. Fertil Steril. 1984;42:373–376. doi: 10.1016/s0015-0282(16)48075-1. [DOI] [PubMed] [Google Scholar]
- Rock JA, Bergquist CA, Kimball AW, et al. Comparison of the operating microscope and loupe for microsurgical tubal anastomosis: a randomised clinical trial. Fertil Steril. 1984;41:229–232. doi: 10.1016/s0015-0282(16)47595-3. [DOI] [PubMed] [Google Scholar]
- Roy KK, Baruah J, Moda N, et al. Evaluation of unilateral versus bilateral ovarian drilling in clomiphene citrate resistant cases of polycystic ovarian syndrome. Arch Gynecol Obstet. 2009;280:573–578. doi: 10.1007/s00404-009-0961-z. [DOI] [PubMed] [Google Scholar]
- Roy KK, Baruah J, Sharma A, et al. A prospective randomized trial comparing the clinical and endocrinological outcome with rosiglitazone versus laparoscopic drilling in patients with polycystic ovarian disease resistant to ovulation induction with clomiphene citrate. Arch Gynecol Obstet. 2010;281 doi: 10.1007/s00404-009-1305-8. [DOI] [PubMed] [Google Scholar]
- Sagiv R, Sadan O, Boaz M, et al. A new approach to office hysteroscopy compared with traditional hysteroscopy. Obstet Gynecol. 2006;108:387–392. doi: 10.1097/01.AOG.0000227750.93984.06. [DOI] [PubMed] [Google Scholar]
- Seiler JC, Gidwani G, Ballard L. Laparoscopic cauterization of endometriosis for fertility: a controlled study. Fertil Steril. 1986;46:1098–1100. doi: 10.1016/s0015-0282(16)49887-0. [DOI] [PubMed] [Google Scholar]
- Selman TJ, Johnson NP, Zamora J, et al. Gynaecologic surgery from uncertainty to science: evolution of randomised control trials. Hum Reprod. 2008;23:827–831. doi: 10.1093/humrep/dem422. [DOI] [PubMed] [Google Scholar]
- Seoud M, Patterson R, Muasher S, et al. Effects of myomas or prior myomectomy on in vitro fertilisation (IVF) programme. J Assist Reprod Genet. 1992;9:217–221. doi: 10.1007/BF01203816. [DOI] [PubMed] [Google Scholar]
- Seracchioli R, Rossi S, Govoni F, et al. Fertility and obstetric outcome after laparoscopic myomectomy of large myomata: a randomised comparison with abdominal myomectomy. Hum Reprod. 2000;15 doi: 10.1093/humrep/15.12.2663. [DOI] [PubMed] [Google Scholar]
- Shankar M, Davidson A, Taub N, et al. Randomised comparison of distension media for outpatient hysteroscopy. BJOG. 2004;111:57–62. doi: 10.1046/j.1471-0528.2003.00004.x. [DOI] [PubMed] [Google Scholar]
- Sharma M, Taylor A, Di Spiezio Sardo A, et al. Outpatient hysteroscopy: traditional versus the ‘no-touch’ technique. BJOG. 2005;112:963–967. doi: 10.1111/j.1471-0528.2005.00425.x. [DOI] [PubMed] [Google Scholar]
- Sharma M, Kriplani A, Agarwal N. Laparoscopic bipolar versus unipolar ovarian drilling in infertile women with resistant polycystic ovarian syndrome. J Gynaecol Surg. 2006;22:105–111. [Google Scholar]
- Shokeir TA, Shalan HM, Shafei MM. Significance of endometrial polyps detected hysteroscopically in eumenorrheic infertile women. J Obstet Gynaecol Res. 2004;30:84–89. doi: 10.1111/j.1447-0756.2003.00163.x. [DOI] [PubMed] [Google Scholar]
- Shokeir T, Shafei M, Yousef H, et al. Submucous myomas and their implications in the pregnancy rates of patients with otherwise unexplained primary infertility undergoing hysteroscopic myomectomy: a randomized matched control study. Fertil Steril. 2009;92:S44–S45. doi: 10.1016/j.fertnstert.2009.03.075. [DOI] [PubMed] [Google Scholar]
- Shojania KG, Bero LA. Taking advantage of the explosion of systematic reviews: an efficient MEDLINE search strategy. Eff Clin Pract. 2001;4:157–162. [PubMed] [Google Scholar]
- Soihet S. Three comparative techniques on tubo-plasty. Int J Fertil. 1974;19:111–115. [PubMed] [Google Scholar]
- Somigliana E, Vercellini P, Daguati R, et al. Fibroids and female reproduction: a critical analysis of the evidence. Hum Reprod Update. 2007;13:465–476. doi: 10.1093/humupd/dmm013. [DOI] [PubMed] [Google Scholar]
- Somigliana E, Vercellini P, Benaglia L, et al. The role of myomectomy in fertility enhancement. Curr Opin Obstet Gynecol. 2008;20:379–385. doi: 10.1097/GCO.0b013e3283073ac9. [DOI] [PubMed] [Google Scholar]
- Soriano D, Ajaj S, Chuong T, et al. Lidocaine spray and outpatient hysteroscopy: randomised placebo-controlled trial. Obstet Gynecol. 2000;96:661–664. doi: 10.1016/s0029-7844(00)00984-4. [DOI] [PubMed] [Google Scholar]
- Stovall DW, Parrish SB, Van Voorhis BJ, et al. Uterine leiomyomas reduce the efficacy of assisted reproduction cycles: results of a matched follow-up study. 1998;13:192–197. doi: 10.1093/humrep/13.1.192. [DOI] [PubMed] [Google Scholar]
- Strandell A, Lindhard A, Waldenström U, et al. Hydrosalpinx and IVF outcome: a prospective, randomized multicentre trial in Scandinavia on salpingectomy prior to IVF. Hum Reprod. 1999;14:2762–2769. doi: 10.1093/humrep/14.11.2762. [DOI] [PubMed] [Google Scholar]
- Surrey ES, Lietz AK, Schoolcraft WB. Impact of intramural leiomyomata in patients with a normal endometrial cavity on in vitro fertilisation-embryo transfer cycle outcome. Fertil Steril. 2001;75:405–410. doi: 10.1016/s0015-0282(00)01714-3. [DOI] [PubMed] [Google Scholar]
- Surrey ES, Minjarez DA, Stevens JM, et al. Effect of myomectomy on the outcome of assisted reproductive technologies. Fertil Steril. 2005;83:1473–1479. doi: 10.1016/j.fertnstert.2004.11.045. [DOI] [PubMed] [Google Scholar]
- Tanahatoe S, Lambalk CB, Hompes PGA. The role of laparoscopy in intrauterine insemination: a prospective ran-domized reallocation study. Hum Reprod. 2005;20:3225–3230. doi: 10.1093/humrep/dei201. [DOI] [PubMed] [Google Scholar]
- Telimaa S, Ronnberg L, Kauppila A. Placebo-controlled comparison of danazol and high-dose medroxyprogesterone acetate in the treatment of endometriosis after conservative surgery. Gynecol Endocrinol. 1987;1:363–371. doi: 10.3109/09513598709082709. [DOI] [PubMed] [Google Scholar]
- Tulandi T, Vilos GA. A comparison between laser surgery and electrosurgery for bilateral hydrosalpinx: a 2-year follow-up. Fertil Steril. 1985;44:846–847. doi: 10.1016/s0015-0282(16)49052-7. [DOI] [PubMed] [Google Scholar]
- Tulandi T. Salpingo-ovariolysis: a comparison between laser surgery and electrosurgery. Fertil Steril. 1986;45:489–491. doi: 10.1016/s0015-0282(16)49274-5. [DOI] [PubMed] [Google Scholar]
- Tulandi T, Falcone T, Kafka I. Second-look laparoscopy one year following reproductive surgery. Fertil Steril. 1989;52:421–424. doi: 10.1016/s0015-0282(16)60911-1. [DOI] [PubMed] [Google Scholar]
- Unfried G, Wieser F, Albrecht A, et al. Flexible versus rigid endoscopes for outpatient hysteroscopy: a prospective randomized clinical trial. Hum Reprod. 2001;16:168–171. doi: 10.1093/humrep/16.1.168. [DOI] [PubMed] [Google Scholar]
- Vandekerckhove P, Donovan P, Lilford R, et al. Treatment of infertility-from cookery to science. Br J Obstet Gynaecol. 1993;100:1005–1036. doi: 10.1111/j.1471-0528.1993.tb15142.x. [DOI] [PubMed] [Google Scholar]
- Varasteh NN, Neuwirth RS, Levin B, et al. Pregnancy rates after hysteroscopic polypectomy and myomectomy in infertile women. Obstet Gynecol. 1999;94:168–171. doi: 10.1016/s0029-7844(99)00278-1. [DOI] [PubMed] [Google Scholar]
- Vegetti W, Ragni G, Baroni E, et al. Laparoscopic ovarian drilling versus low-dose pure FSH in anovulatory clomiphene-resistant patients with polycystic ovarian syndrome: randomised prospective study. Hum Reprod. 1998;13:120. [Google Scholar]
- Venturini N, Tantini C, Bargilli G. Hysteroscopy for evaluation of tubal ostium pathology. Acta Europea Fertilitatis. 1987;18:61–62. [PubMed] [Google Scholar]
- Vercellini P, Crosignani PG. Minimal and mild endometriosis- is there anything new under the sun? J Reprod Med. 1993;38:49–52. [PubMed] [Google Scholar]
- Vercellini P, Crosignani P, Fadini R, et al. A gonadotrophin-releasing hormone agonist compared with expectant management after conservative surgery for symptomatic endometriosis. Br J Obstet Gynecol. 1999;106:672–677. doi: 10.1111/j.1471-0528.1999.tb08366.x. [DOI] [PubMed] [Google Scholar]
- Vilos G. Uterine fibroids: relationship to reproduction. Minerva Ginecol. 2003;55:417–423. [PubMed] [Google Scholar]
- Vimercati A, Scioscia M, Lorusso F, et al. Do uterine fibroids affect IVF outcomes? Reprod Biomed Online. 2007;15:686–691. doi: 10.1016/s1472-6483(10)60536-6. [DOI] [PubMed] [Google Scholar]
- Wang W, Check JH, Dietterich C, et al. Effect of fibroids on cumulative probability of pregnancy in women taking follicle maturing drugs without assisted reproductive technology. Clin Exp Obstet Gynecol. 2001;28:86–88. [PubMed] [Google Scholar]
- Wang W, Check JH. Effect of corporal fibroids on outcome following embryo transfer in donor-oocyte recipients. Clin Exp Obstet Gynecol. 2004;31:263–264. [PubMed] [Google Scholar]
- Weerakiet S, Lertvikool S, Tingthanatikul Y, et al. Ovarian reserve in women with polycystic ovary syndrome who underwent laparoscopic ovarian drilling. Gynecol Endocrinol. 2007;23:455–460. doi: 10.1080/09513590701485212. [DOI] [PubMed] [Google Scholar]
- Wise LA, Palmer JR, Harlow BL, et al. Reproductive factors, hormonal contraception, and risk of uterine leiomyomata in African-American women: a prospective study. Am J Epidemiol. 2004;159:113–123. doi: 10.1093/aje/kwh016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wyns C, Donnez J. Laser vaporization of ovarian endometriomas: the impact on the response to gonadotropin stimulation. Gynecol Obstet Fertil. 2003;31:337–342. doi: 10.1016/s1297-9589(03)00069-9. [DOI] [PubMed] [Google Scholar]
- Yanaihara A, Yorimitsu T, Motoyama H, et al. Location of endometrial polyp and pregnancy rate in infertility patients. Fertil Steril. 2008;90:180–182. doi: 10.1016/j.fertnstert.2007.05.072. [DOI] [PubMed] [Google Scholar]
- Yap C, Furness S, Farquhar C, et al. Pre and postoperative medical therapy for endometriosis surgery. Cochrane Database Syst Rev. 2009;(issue 1:CD 003678) doi: 10.1002/14651858.CD003678.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yarali H, Bukulmez O. The effect of intramural and subserous uterine fibroids on implantation and clinical pregnancy rates in patients having intracytoplasmic sperm injection. Arch Gynecol Obstet. 2002;266:30–33. doi: 10.1007/pl00007491. [DOI] [PubMed] [Google Scholar]
- Yazbeck C, Madelenat P, Sifer C, et al. Ovarian endometriomas: effect of laparoscopic cystectomy on ovarian response in IVF-ET cycles. Gynecol Obstet Fertil. 2006;34:808–812. doi: 10.1016/j.gyobfe.2006.07.003. [DOI] [PubMed] [Google Scholar]
- Yossry M, Aboulghar M, Angelo A, et al. In vitro fertilisation versus tubal reanastomosis (sterilisation reversal) for subfertility after tubal sterilisation. Cochrane Database Syst Rev. 2006;(issue 3:CD 004144) doi: 10.1002/14651858.CD004144.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Youssef H, Atallah MM. Unilateral ovarian drilling in polycystic ovarian syndrome: a prospective randomized study. Reprod Biomed Online. 2007;15:457–462. doi: 10.1016/s1472-6483(10)60373-2. [DOI] [PubMed] [Google Scholar]
- Zakherah MS, Nasr A, El Salman AM, et al. Clomiphene citrate plus tamoxifen versus laparoscopic drilling in women with clomiphene-resistant polycystic ovary syndrome. Int J Gynecol Obstet. 2010;108:240–243. doi: 10.1016/j.ijgo.2009.10.004. [DOI] [PubMed] [Google Scholar]