

Abstract
There is growing awareness of the need for methodologies that can be used retrospectively to provide the biodosimetry needed to carry out screening and triage immediately after an event in which large numbers of people have potentially received clinically significant doses of ionizing radiation. The general approach to developing such methodologies has been a technology centric one, often ignoring the system integrations considerations that are key to their effective use. In this study an integrative approach for the evaluation and development of a physical biodosimetry technology was applied based on in vivo electron paramagnetic resonance (EPR) dosimetry. The EPR measurements are based on physical changes in tissues whose magnitudes are not affected by the factors that can confound biologically-based assessments. In this study the use of a pilot simulation exercise to evaluate an experimental EPR system and gather stakeholders’ feedback early on in the development process is described. The exercise involved: ten non-irradiated participants, representatives from a local fire department; Department of Homeland Security certified exercise evaluators, EPR experts, physicians; and a human factors engineer. Stakeholders were in agreement that the EPR technology in its current state of development could be deployed for the screening of mass casualties. Furthermore, stakeholders’ recommendations will be prioritized and incorporated in future developments of the EPR technique. While the results of this exercise were aimed specifically at providing feedback for the development of EPR dosimetry for screening mass casualties, the methods and lessons learned are likely to be applicable to other biodosimetric methods.
Keywords: dose assessment, dose, population, emergencies, radiological, emergency planning
INTRODUCTION
In the field of emergency response for radiological events, there is growing awareness of the need for methodologies that can be used retrospectively to provide the biodosimetry needed to carry out triage immediately after an event in which large numbers of people have potentially received clinically significant doses of ionizing radiation (Alexander et al. 2007; González 2007; Simon et al. 2007) as described in the companion paper (Gougelet et al. 2010). In an event such as the one described by the U.S. Department of Homeland Security in their planning scenarios, the detonation of a 10 kiloton improvised nuclear device (IND) in Washington, DC, would potentially involve hundreds of thousands of fatalities due to the blast itself and would lead to the potential exposure of hundreds of thousands of additional people to varying levels of ionizing radiation (U.S. DHS 2005; Meade and Molander 2006). In such a catastrophic event, the number of people included among the “worried-well” would exceed the number of truly affected people by a factor of 5 to 10 (IAEA 1998; Okumura et al. 1998a and b), leading to the potential paralysis of the emergency response and medical systems. Furthermore, the current guidelines and response systems do not address this problem (Gougelet et al. 2010; Rea et al. 2010).
In response to the need for improved capabilities for triage for a large event, the biodosimetry community has responded through active development of several methodologies. These include physical methods such as electron paramagnetic resonance (EPR), optically stimulated luminescence (OSL) and thermoluminescence characterization; biologically-based methods such as semiautomated cytogenetic methodologies (including FISH, micronuclei, and dicentric assays); metabolomic approaches, gene expression signature assays, and proteomic analyses. However, in the design of technologies and procedures for emergency preparedness and response, developers must avoid taking a technology-centric approach in which the technology is proposed as the one alternative to address the problem and often ignores the real needs in a catastrophic event and the system issues that will be present in such an event. Such methods use accuracy expectations and processes that would accommodate a relatively small number of patients. As proposed in this paper, it is important that the emergency response community is involved in the evaluation and development process of these technologies.
The current environment for the development of biodosimetry methodologies had contributed to a disconnected process in which research labs develop the different technologies with little consideration for the system in which they would ultimately be used. The research labs often concentrate on the technology itself, rather than thinking about the problem or needed capability to respond to the catastrophic event and the system integration issues for the individual technologies. The need in such events is the capability to perform rapid and effective after-the-fact biodosimetry to screen the large numbers of patients seen after such events. The development process must address the fact that a combination of technologies appropriately applied by the end-user(s) of the system, who have often been left out of the development process, is likely to be more effective than the exclusive use of only one technology. Problems with this general approach have been well documented. One example is the communication breakdown for the first responders during the 11 September 2001, terrorist attacks in New York city (Kean and Hamilton 2004). In this example the technology itself, the radio systems, worked as expected. However, the failure to integrate these radio systems across the multiple first-response organizations such as fire department, police, and search and rescue led to the reported ineffectiveness of the communication system as a whole. Likewise, a compounding problem of the current environment for the development of biodosimetric technologies is the apparent disconnect between the funding and regulatory mechanisms and the development process itself. The federal plans for emergency response also contribute to this problem due to complexity and the large number of organizations that have been given the responsibility to plan and respond to emergencies. Flood et al. (2007) have described this problem in more detail.
This paper will focus on describing a methodology for the integrative evaluation and development of in vivo EPR dosimetry as one of the methods for the after-the-fact measurement of radiation exposure following a catastrophic nuclear event. Details regarding the in vivo EPR dosimetry technique and its associated safety, reliability and accuracy have been reported elsewhere (Salikhov and Swartz 2005; Swartz et al. 2005, 2006, 2007; Williams et al. 2007, 2010). The methodology described here is based on a participatory-design approach that involves key stakeholders early in the development phase of the technology through the use of a simulation exercise. The approach of using a simulated nuclear device detonation as the scenario and in vivo EPR dosimetry screening for the exercise resembles the Department of Homeland Security (DHS) Target Capability List development process that starts with the creation of planning scenarios followed by the generation of tasks that would need to be performed to respond to the event, leading to the identification of capabilities that need to be in place to accomplish the response and mitigation tasks (U.S. DHS 2007).
Objectives
The main objectives of this study were twofold: 1) to demonstrate the use of a simulation exercise for the integrative evaluation and development of in vivo EPR dosimetry for its use in screening mass casualties after a catastrophic nuclear event, and 2) to gather baseline characteristics of the in vivo EPR dosimetry technology to guide future developments that take into account system integration issues.
To satisfy these objectives, the following specific aims were accomplished:
Capture expert opinions about operational factors of the in vivo EPR dosimetry system;
Capture patients’ perspectives about the measurement method;
Capture baseline characteristics of the in vivo EPR dosimetry system;
Perform a detailed task analysis; and
Generate recommendations to be incorporated in the next version of the in vivo EPR dosimetry system.
METHODS
Participants
For this simulation exercise, 10 normal volunteers with no history of occupational or medical exposure to ionizing radiation were recruited to play the roles of people who may have been exposed to significant doses to ionizing radiation after a nuclear device detonation. The exercise did not include simulation of emotional stress or other environmental factors and did not include participants with implanted pre-irradiated teeth. The scope of this study was limited to identifying operational and system integration issues of the in vivo EPR dosimetry technology to be used as a screening tool after a catastrophic nuclear event involving large numbers of people.
Stakeholders
The stakeholders involved in this simulation exercise included representatives from a local fire department, Department of Homeland Security certified exercise evaluators, in vivo EPR dosimetry experts, physicians, and a human factors engineer. In vivo EPR dosimetry experts included engineers and scientists involved in the development of the technology. The human factors engineer conducted the post hoc task analysis, cycle time analysis, and conducted brainstorming sessions among designers and operators of the in vivo EPR dosimetry system using the video recordings as discussion generating tools. This wide range of exercise participants enabled cross-communication among all stakeholders.
EPR operators
Three experienced operators were involved in operating the in vivo EPR dosimetry system. One of them was solely in charge of patient handling and positioning the EPR detector on the teeth of interest in the patients’ mouths. The other two operated the electronics and computer interface. Operators were members of the research team and operated the in vivo EPR dosimetry system on a daily basis for the purpose of clinical studies, described elsewhere (Williams et al. 2007, 2010). One additional person was in charge of greeting patients and stakeholders, as well as handling consent forms and questionnaires.
The nuclear device detonation scenario
The scenario for this exercise was the nuclear detonation of a 10 kiloton improvised nuclear device in Washington, DC, one of the 15 planning scenarios described by the U.S. Department of Homeland Security (2005). The introduction of the scenario was important to set the context in which the exercise involving in vivo EPR dosimetry would take place.
Protocol
The simulation exercise took place at Dartmouth-Hitchcock Medical Center in the afternoon of 30 May 2008. The simulation exercise started at 11 am when stakeholders gathered and were briefed about the simulation exercise scenario. The first group of three participants arrived at the site 15 minutes before 12 pm. They were greeted and ushered to a conference room where they were briefed and introduced to the process and the overall goal of the simulation exercise using standard procedures and informative pamphlets.
Participants were asked to arrive in groups of three every 60 min to avoid crowding in the facility. However, it is worth noting that in a real event potentially-exposed people would come in larger batches. This has been described in more detail in a companion paper (Gougelet et al. 2010). Then stakeholders were asked to position themselves in the procedure room, after which participants were tested one by one. Fig. 1 shows the layout of the facility used for the simulation exercise. Fig. 2 is a flow chart of the simulation exercise protocol.
Fig. 1.

Layout of the simulation exercise facility.
Fig. 2.

Flow chart of the simulation exercise protocol.
Measuring process
The in vivo EPR tooth dosimetry measurement process has been described in more detail elsewhere (Williams et al. 2007, 2010). In summary, the measurements involved in the simulation exercise included:
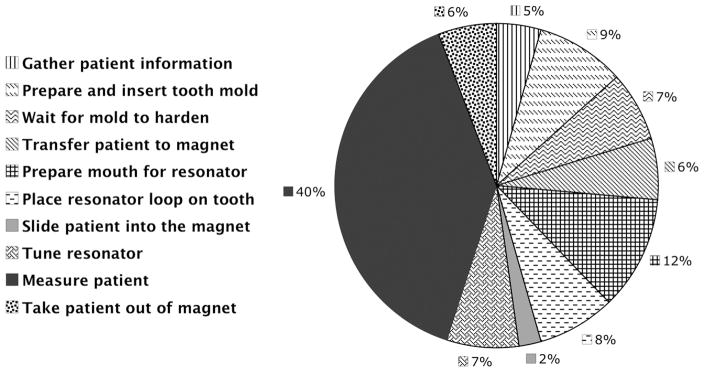
gathering the patient’s information, including history of radiation exposures, use of any life-supporting medical implant, and determining the tooth to be measured;
preparing and inserting the tooth mold, which facilitates the correct positioning of the EPR detector over the target tooth–this was accomplished in a chair positioned behind and diagonally to the EPR dosimeter as shown in Fig. 1;
waiting for tooth mold to harden;
transferring the patient to the EPR dosimeter, which involved asking the patient to lie down on a retractable bed attached to the spectrometer;
preparing the mouth, which involved the placement of a cheek retractor, dental cotton rolls and pads inside the patient’s mouth;
placing the resonator over the tooth, which included placing the previously created mold and the resonator itself;
sliding the patient inside the in vivo EPR dosimetry system magnet;
tuning the resonator, which involves setting the RF power to the operational level, frequency control and resonator coupling knob;
collecting the spectra; and
taking the patient out of the in vivo EPR dosimetry system magnet.
Patient debriefing
After patients were measured, they were asked to return to the conference room and to fill out a questionnaire. The questionnaire was aimed at gathering information regarding the patients’ physical comfort with the measuring process as well as inquiring about their anxiety level before, during and after the measurement.
Observers debriefing
Before observers left, they were asked to fill out a questionnaire that asked about their opinions regarding the measuring process and the applicability of the technology for immediate screening of mass casualties after a catastrophic nuclear event. The questionnaire included questions such as:
Do you feel that EPR could be used for triaging mass casualties in the case of a terrorist attack with an improvised nuclear device? Yes/No
What are some of the barriers to using EPR in a mass-casualty situation?
What are some of the positive aspects of using EPR in a mass-casualty situation?
Other measurements
For the duration of the simulation exercise, video recordings were taken with the goal of performing post hoc task analysis and cycle time analysis, and to use the recordings as discussion-generating and brainstorming tools among designers and operators of the in vivo EPR dosimetry system.
RESULTS
The results of this study can be divided into two categories: results regarding technical aspects of the in vivo EPR dosimetry technology and results regarding system integration aspects of the physical biodosimetry method for after-the-fact estimation of radiation exposures after a catastrophic nuclear event.
Technical results
Cycle time
Using the video recordings, analysis of the cycle time was performed post hoc, times were calculated for each of the steps described in the “Measuring process” section of the Methodology (above) for each patient, and descriptive statistics were calculated. The average cycle time was 17.4 min with a range of 15.3 to 19.4 min. Fig. 3 shows a break down analysis of the cycle time.
Fig. 3.
Cycle time analysis.
Patient questionnaire results
Every question on the patient’s questionnaire was in the form of a Likert scale. To summarize patients’ responses, an average rating for every question was calculated. Fig. 4 shows the summary results of the patients’ questionnaire.
Fig. 4.

Patients’ questionnaire summary results.
System integration results
Stakeholders’ opinions regarding the measuring process and the applicability of in vivo EPR dosimetry for the triage of large numbers of people that might be potentially exposed to radiation after a catastrophic nuclear event were considered as system integration factors for adopting in vivo EPR dosimetry for emergency response.
Table 1 shows a summary of the common comments among key stakeholders.
Table 1.
Summary of stakeholders’ comments.
| EPR dosimetry attributes | Summary of expert opinions |
|---|---|
| Measuring speed | The process was relatively quick, although some parallel processing could reduce the measuring time. |
| Resources need | Little waste and clean up was required for each patient. However the process required an extra person to tune the resonator. |
| Patient friendliness | The process was painless, and communication between patient and operators was effective and easy. However, patient comfort can be improved specially in regards to the dental- work-like procedure, and the size of the magnetic cavity. |
| User friendliness | The measuring process is complex enough that operators would need some training, and have some prior level of technical skills. |
| Size | The size of the machine can be reduce to improve portability. |
| Complexity | Complex system with multiple possible point of failure. |
| Tooth interrogating device | Placement of the tooth interrogating device (resonator) was dependant on operator’s experience, and its sensitivity was dependant on patient’s movement. The resonator holding arm seem unstable. |
| Deployability | The system could be deployed. However, significant man power, and storage capacity would be needed. |
Stakeholders were also asked to provide recommendations to improve the in vivo EPR dosimetry technology. Table 2 shows their recommendations.
Table 2.
Stakeholders’ recommendations.
| Recommendations |
|---|
| Automix cartridges could allow direct application of impression material to mouth tray to create tooth molds. |
| Improvements to the tooth interrogating device placement would guarantee reproducibility of positioning and measurement. |
| Measuring a sample of the population instead of measuring everyone would reduce the time to triage mass casualties. |
| One might want to have a rapid and reliable system that can be deployed in a tollbooth style along highways. |
| The measurement can take place in an assembly line fashion, in order to reduce the cycle time. |
| Data transmissions via wireless communications to clinicians and medical centers would facilitate the triaging process. |
| Information to patients should be provided in the form or multilingual pamphlets. |
| Upright sitting position will eliminate the need for cotton rolls and the gagging reflex on patients. |
| Faster measuring process could decrease the fear to the unknown in patients. |
DISCUSSION
In general, stakeholders were in agreement that the in vivo EPR dosimetry technology in its current state of development has the potential to be useful for the triage of mass casualties, if enough resources and physical space are allocated to the operation and storage of such equipment. One potentially useful approach for application with the existing instrumentation would be the sampling of the potentially-irradiated population rather than measuring every individual in such population. It is worth noting that the stakeholders’ comments pertain to operational aspects of the in vivo EPR dosimetry technique and do not address sensitivity and specificity aspects of the technique.
With regard to the technical aspects of the in vivo EPR dosimetry technique, the stakeholders recommended that performing some of the patient preparation steps in parallel could reduce the cycle time. Analysis of the cycle time from video recordings and the task analysis support this argument. About 50% of the time spent with each patient was preparation time, which could be performed in advance while other patients are in the in vivo EPR dosimetry system, thus potentially reducing the cycle time to 8 to 10 min.
Another important aspect that stakeholders brought up is the reproducibility of the positioning of the resonator in the patient’s mouth. They argued that, as it is, it depends on the operator’s experience and the patient’s ability to be immobilized. They recommended the possibility of performing the measurement in a seated position to minimize the need for cotton rolls and to improve reproducibility.
Finally, the patient questionnaire showed that patients were generally moderately comfortable with the measuring process, and they showed minimal levels of anxiety before, during, and after the measuring procedure.
From this study several next steps can be delineated for the improvement of the in vivo EPR dosimetry technique as well as for the use this new integrative approach to evaluate and develop a biodosimetric capability for the triage of mass casualties after a catastrophic nuclear event. First, the prioritization and appropriate implementation of the stakeholders’ recommendations regarding the technical aspects of the in vivo EPR dosimetry technology should help guide future versions of the in vivo EPR dosimetry system. Second, a larger simulation exercise should be planned and conducted that would simulate to a greater level of detail the conditions after a nuclear catastrophic event and the needed triage capabilities using a new version of the in vivo EPR dosimetry technology. Finally, an integrated system should be designed, developed, and assessed that would support the deployment of the in vivo EPR dosimetry technology based on adapting current systems for emergency response; the need for this system has been described in more detail in a companion paper in this issue (Gougelet et al. 2010).
CONCLUSION
An early-stage simulation exercise was useful as a tool for integrating stakeholders’ feedback in the design, development, and evaluation process of a new biodosi-metric technology based on a physical method for measuring radiation dose in vivo. This approach simulated the needs and conditions of a biodosimetric technique for the after-the-fact determination of radiation dose in potentially exposed victims of a catastrophic nuclear event, and used the in vivo EPR dosimetry methodology to provide the needed capability. From this approach, important recommendations were gathered from stakeholders that would lead to improvements in the current technology and methods to perform in vivo EPR dosimetry for the purpose of triaging mass casualties after a nuclear catastrophic event. This approach is likely to be useful for the optimal development of all types of after-the-fact dosimetric technologies and to generate information needed for modeling the emergency response system for radiological events, taking into consideration all the complementary methods’ strengths and weaknesses, so that thorough cost-benefit/effectiveness can be evaluated. This in turn can guide policy-making at the local and federal levels regarding preparedness and funding for catastrophic nuclear events.
Acknowledgments
Research supported by the National Institutes of Health (NIH) award number U19AI067733, and Defense Advanced Research Project Agency (DARPA) award number HR0011-08-C-0023.
Footnotes
Disclaimer: The views, opinions, and/or findings contained in this article are those of the author and should not be interpreted as representing the official policies, either expressed or implied, of the Defense Advanced Research Projects Agency or the Department of Defense.
References
- Alexander GA, Swartz HM, Amundson SA, Blakely WF, Buddemeier B, Gallez B, Dainiak N, Goans RE, Hayes RB, Lowry PC. BiodosEPR-2006 Meeting: acute dosimetry consensus committee recommendations on biodosimetry applications in events involving uses of radiation by terrorists and radiation accidents. Radiat Meas. 2007;42:972–996. [Google Scholar]
- Flood AB, Bhattacharyya S, Nicolalde RJ, Swartz HM. Implementing EPR dosimetry for life-threatening incidents: factors beyond technical performance. Radiat Meas. 2007;42:1099–1109. doi: 10.1016/j.radmeas.2007.05.042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- González AJ. An international perspective on radiological threats and the need for retrospective biological dosimetry of acute radiation overexposures. Radiat Meas. 2007;42:1053–1062. [Google Scholar]
- Gougelet RM, Nicolalde RJ, Rea M, Swartz HM. The view from the trenches: part 1—emergency medical response plans and the need for EPR screening. Health Phys. 2010;98:118–127. doi: 10.1097/HP.0b013e3181a6de7d. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ikeya M, Miki T, Kai A, Hoshi M. ESR dosimetry of A-bomb radiation using tooth enamel and granite rocks. Radiat Protect Dosim. 1986;17:181–184. [Google Scholar]
- International Atomic Energy Agency. The radiological accident in Goiania. Vienna: IAEA; 1998. [Google Scholar]
- Kean TH, Hamilton L. The 9/11 Commission Report: Final Report of the National Commission on Terrorist Attacks Upon the United States. New York: WW Norton & Co Inc; 2004. [Google Scholar]
- Meade C, Molander RC. Technical Report of the RAND Center for Terrorism Risk Management Policy. Santa Monica: RAND Corporation; 2006. Considering the effects of a catastrophic terrorist attack. [Google Scholar]
- Okumura T, Suzuki K, Fukuda A, Kohama A, Takasu N, Ishimatsu S, Hinohara S. The Tokyo subway sarin attack: disaster management, part 1: community emergency response. Acad Emerg Med. 1998a;5:613–617. doi: 10.1111/j.1553-2712.1998.tb02470.x. [DOI] [PubMed] [Google Scholar]
- Okumura T, Suzuki K, Fukuda A, Kohama A, Takasu N, Ishimatsu S, Hinohara S. The Tokyo subway sarin attack: disaster management, part 2: hospital response. Acad Emerg Med. 1998b;5:618–624. doi: 10.1111/j.1553-2712.1998.tb02471.x. [DOI] [PubMed] [Google Scholar]
- Rea M, Gougelet RM, Nicolalde RJ, Swartz HM. Triaging categories and medical guidelines for the acute radiation syndrome. Health Phys. 2010;98:136–144. doi: 10.1097/HP.0b013e3181b2840b. [DOI] [PubMed] [Google Scholar]
- Salikhov I, Swartz H. Measurement of specific absorption rate for clinical EPR at 1200 MHz. Appl Magn Reson. 2005;28:287–291. [Google Scholar]
- Simon SL, Bailiff I, Bouville A, Fattibene P, Kleinerman RA, Lloyd DC, McKeever SWS, Romanyukha A, Sevan’kaev AV, Tucker JD. BiodosEPR-2006 consensus committee report on biodosimetric methods to evaluate radiation doses at long times after exposure. Radiat Meas. 2007;42:948–971. [Google Scholar]
- Swartz HM, Burke G, Coey M, Demidenko E, Dong R, Grinberg O, Hilton J, Iwasaki A, Lesniewski P, Kmiec M, Lo K, Javier Nicolalde R, Ruuge A, Sakata Y, Sucheta A, Walczak T, Williams BB, Mitchell CA, Romanyukha A, Schauer DA. In vivo EPR for dosimetry. Radiat Meas. 2007;42:1075–1084. doi: 10.1016/j.radmeas.2007.05.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Swartz HM, Iwasaki A, Walczak T, Demidenko E, Salikhov I, Khan N, Lesniewski P, Thomas J, Romanyukha A, Schauer D, Starewicz P. In vivo EPR dosimetry to quantify exposures to clinically significant doses of ionising radiation. Radiat Protect Dosim. 2006;120:163–170. doi: 10.1093/rpd/nci554. [DOI] [PubMed] [Google Scholar]
- Swartz HM, Iwasaki A, Walczak T, Demidenko E, Salikov I, Lesniewski P, Starewicz P, Schauer D, Romanyukha A. Measurements of clinically significant doses of ionizing radiation using non-invasive in vivo EPR spectroscopy of teeth in situ. Appl Radiat Isot. 2005;62:293–299. doi: 10.1016/j.apradiso.2004.08.016. [DOI] [PubMed] [Google Scholar]
- U.S. Department of Homeland Security. Target capabilities list. Washington: U.S. DHS; 2007. [Google Scholar]
- U.S. Department of Homeland Security. Created for use in national, federal, state, and local homeland security preparedness activities. Washington, DC: U.S. DHS; 2005. [Accessed 31 October 2008]. National planning scenarios. (draft). Available at media.washingtonpost.com/wpsrv/nation/nationalsecurity/earlywarning/NationalPlanningScenariosApril2005.pdf. [Google Scholar]
- Williams BB, Sucheta A, Dong R, Sakata Y, Iwasaki A, Burke G, Grinberg O, Lesniewski P, Kmiec M, Swartz HM. Experimental procedures for sensitive and reproducible in situ EPR tooth dosimetry. Radiat Meas. 2007;42:1094–1098. doi: 10.1016/j.radmeas.2007.05.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams BB, Dong R, Kmiec M, Burke G, Corliss B, Demidenko E, Gladstone D, Grinberg O, Nicolalde J, Pollack J, Raynolds T, Salikhov I, Sucheta A, Lesniewski P, Swartz HM. Radiation dose estimation from EPR tooth measurements. Health Phys. 2010;98:327–338. doi: 10.1097/HP.0b013e3181a6de5d. [DOI] [PMC free article] [PubMed] [Google Scholar]