

Abstract
Background
HIV-infected patients may be at increased risk of cardiovascular (CV) events, and lipodystrophy is generally associated with proatherogenic metabolic disturbances. Carotid intima-media thickness (cIMT) has been used as a surrogate marker for atherosclerosis and it has been shown to be an independent risk factor for CV disease. Our objective was to evaluate cIMT in HIV-infected patients on combined anti-retroviral therapy (cART) with and without lipodystrophy defined by fat mass ratio (L-FMR), and to determine the association of lipodystrophy and visceral obesity [(visceral (VAT), subcutaneous adipose tissue (SAT) volume and VAT/SAT ratio, objectively evaluated by CT scan] with cIMT.
Methods
Cross-sectional study of 199 HIV-infected patients. Body composition by DXA and abdominal CT, lipids, blood pressure, inflammatory markers, and cIMT by ultrasonography were performed. L-FMR was defined as the ratio of the percentage of trunk fat mass to the percentage of lower limb fat mass by DXA. Categorical variables were compared using the chi-square or Fisher’s exact test. Spearman correlation coefficients were estimated to study the association between cIMT and clinical and metabolic characteristics. Means of cIMT, adjusted for age, were calculated, using generalized linear models.
Results
L-FMR was present in 41.2% of patients and cIMT was higher in these patients [0.81 (0.24) vs. 0.76 (0.25); p = 0.037)]. Lipodystrophic patients had higher VAT and VAT/SAT ratio and lower SAT. cIMT was associated with lipodystrophy evaluated by FMR, trunk fat, total abdominal fat, VAT and VAT/SAT ratio. No association was observed between cIMT and leg fat mass. Using generalized linear models, cIMT means were adjusted for age and no significant differences remained after this adjustment. The adjusted mean of cIMT was 0.787 (95% CI: 0.751-0.823) in patients without lipodystrophy, and 0.775 (95% CI: 0.732-0.817) in those with lipodystrophy (p = 0.671).
Conclusions
HIV-infected patients on cART with lipodystrophy defined by FMR, had a significantly higher cIMT. Carotid IMT was also associated with classical cardiovascular risk factors. In these patients, visceral adipose tissue had a significant impact on cIMT, although age was the strongest associated factor.
Keywords: Lipodystrophy, HIV, Carotid intima media thickness, Fat mass ratio, Body composition
Background
The development of atherosclerosis lesions is a slow and progressive process. The use of noninvasive surrogate markers of atherosclerosis may improve the prognostic stratification of HIV-infected patients with cardiovascular risk factors, and also clarify some of the pending issues related to this disease in HIV infection. Ultrasound is a safe, inexpensive and rapid technique, which allows an accurate evaluation of atherosclerosis [1]. Intima-media thickness (IMT) of the carotid arteries has been used as a surrogate marker for atherosclerosis and it has been shown to be an independent risk factor for cardiovascular disease. The role of age, prolonged survival, traditional and non-traditional risk factors, direct effect of HIV infection and cART, in relation to surrogate markers of atherosclerosis are under continuous debate [1]. Thus, due to the long-term survival associated with cART, harmful effects of the treatment emerge, as well as a chronic inflammatory state. However, HIV itself may also promote atherosclerosis by activating the vascular endothelium directly, or indirectly, by systemic cytokine stimulation by the virus [2]. Higher rates of sub-clinical atherosclerosis are seen in HIV-1-infected patients, and, controversially, these are usually attributed to classic cardiovascular risk factors and to the side effects of cART [3-5].
Although the disease can cause alterations in several metabolic pathways, such as lipid and glucose metabolism, lipodystrophic patients, per se, may also be at a higher risk of atherosclerosis, as fat redistribution is associated with the presence of several known metabolic risk factors for cardiovascular diseases [6]. Furthermore, patients with clinical lipodystrophy have a significantly higher risk of coronary heart disease at 10 years, measured by the Framingham risk score, than patients without clinical lipodystrophy and those with clinical lipodystrophy and metabolic syndrome were more often classified in moderate and high risk categories, than those without metabolic syndrome [7].
The objectives of this study were to evaluate cIMT in HIV-infected patients subject to cART, according to the presence of lipodystrophy, as objectively defined by FMR, and also to evaluate the association of lipodystrophy, visceral obesity [(visceral (VAT), subcutaneous adipose tissue volume (SAT) and VAT/SAT ratio objectively evaluated by CT scan] and other established cardiovascular risk factors, with cIMT.
Methods
Subjects
As part of a cross-sectional study, clinically stable, HIV-infected, non-institutionalized Caucasian adults who were receiving antiretroviral therapy were evaluated. These were all referred from the Infectious Diseases Outpatient Clinic and only patients subject to cART were included. This study was approved by the Ethics Committee for Health of the Hospital São João in Porto and each patient agreed to provide written, informed consent.
Clinical assessment
For each patient, the following information was collected, using a standardized protocol: age, gender, known duration of HIV infection and duration of cART exposure, HIV risk factor, characterization of the infection, smoking history (past, current, or never), family history of CV diseases, and use of anti-hypertensive, anti-diabetic, or lipid lowering drugs.
We used the “Centers for Disease Control and Prevention” (CDC) HIV staging classification [8]. Weight, height, circumferences of neck, waist, hip, thigh and arm were measured, as previously described [9]. All measurements were performed by the same observer, using standard techniques [10].
Resting blood pressure (BP) taken whilst in a supine position was measured in a standardized fashion, as previously described [7].
Evaluation of body composition
Body composition was assessed with whole-body, dual-energy X-ray absorptiometry (DXA) (DXA – Lunar Expert XL, 1999). DXA measurements were performed while the patient was in a supine position, with standard positioning of the arms and feet. Markers for the trunk and lower limbs that defined regions of interest were defined in accordance with the manufacturer’s instructions. Regional fat mass values were grouped and analyzed for the following anatomical regions: arms, legs, trunk and total body. The fat mass ratio (FMR) was calculated as the ratio between the percentage of trunk fat mass and the percentage of lower limb fat mass (FMR =% of the trunk fat mass/% of the lower limb fat mass) [11]. We used a cut-off value for lipodystrophy defined by FMR for men of 1.961, and 1.329 for women [12].
The quantification of total, visceral, and subcutaneous fat was performed with a 64-slice, abdominal computed tomography (CT) scanner (Siemens Sensation 64 Cardiac), with the same technique as previously described [13,14]. All values were expressed in cm2, rounded to the nearest centesimal.
Laboratory analysis
Biological and inflammatory parameters:
A venous blood sample was taken after a 12-hour overnight fast. All the samples were analyzed at the central laboratory of our hospital. The measurements of total cholesterol (TC), low density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol, triglycerides, apolipoprotein A1 (apo A1), apolipoprotein B (apo B), lipoprotein (a) [Lp (a)], fibrinogen, high sensitivity C-reactive protein (hsCRP), homocysteine, uric acid, lactates, NT-proBNP, glucose, insulin and A1c serum levels were determined using commercial kits. Non HDL-C was defined as TC-HDL. Microalbuminuria was determined in a 24 hour urine sample. Patients without a previous diagnosis of diabetes were submitted to an oral glucose tolerance test (OGTT). This test was performed as instructed by the World Health Organization [15].
The CD4+ cell count (×106 cell/L) was determined by flow cytometry and plasma HIV-1 RNA loads were measured by a quantitative reverse transcriptase polymerase chain reaction (Roche Diagnostic Systems, Inc., Branchburg, NJ, USA), which had a lower limit of detection of 50 copies/mL.
Measurements of insulin resistance
Insulin resistance was defined by the homeostasis model assessment of insulin resistance (HOMA), using the following formula:
HOMA ‒ IR index = (insulin 0 x glucose 0)/22.5 [16].
Carotid IMT measurement
High-resolution B-mode and Doppler ultrasonography of the carotid arteries was carried out with a Philips iU22 machine (Philips Medical, The Netherlands), equipped with a 17–5 MHz high-frequency linear-array transducer. Patients were examined in the supine position, with the head in a neutral position, or slightly turned away from the side that was being scanned. The left and right common carotid arteries (CCA) were examined in multiple directions and measurements were performed using the images with the best wall definition. IMT was measured 3 cm below the carotid bulb in a longitudinal image. Three measurements were obtained on each side, and the mean IMT of these values was calculated. All studies were performed by the same radiologist, who had 12 years of experience in vascular ultrasound, and were carried out using the same machine.
The presence of subclinical carotid atherosclerosis was defined as IMT > 0.80 mm (70th percentile of the IMT distribution), presence of plaque, or both [17-19].
Statistical analysis
Data was described as mean and standard deviation (SD) for quantitative variables, and was compared using Student-t or Mann–Whitney tests, as appropriate. Categorical variables were described as counts and proportions, and compared using the chi-square or Fisher’s exact test. To study the association between cIMT and clinical and metabolic characteristics, Spearman correlation coefficients were estimated. Means of cIMT, adjusted for age, were calculated, using generalized linear models.
Statistical analysis was performed using SPSS version 17.0 software (SPSS Inc., Chicago, Illinois, USA). All probabilities were two tailed and p values of <0.05 were regarded as significant.
Results
Patient characteristics
In this sample of 199 HIV-1 infected patients (132 men and 67 women) on cART, 41.2% presented lipodystrophy defined by FMR. Table 1 shows the characteristics of the study sample, according to the presence of lipodystrophy defined by FMR.
Table 1.
Sample characteristics according to the presence of lipodystrophy defined by FMR
| |
Without L |
With L |
P
|
|---|---|---|---|
| n (%) | 117 | 82 | - |
| Gender [n (%)] |
|
|
|
| Male |
71 (60.7) |
61 (74.4) |
0.063 |
| Female |
46 (39.3) |
21 (25.6) |
|
| Age [years, mean (sd)] |
44.8 (12.1) |
49.2 (10.2) |
0.002 |
| Duration of HIV infection [years, mean (sd)] |
7.2 (3.8) |
8.5 (3.5) |
0.005 |
| cART [years, mean (sd)] |
5.7 (3.7) |
7.9 (3.3) |
<0.001 |
| Weight [Kg, mean (sd)] |
68.0 (14.3) |
68.0 (10.6) |
0.805 |
| Height [m, mean (sd)] |
1.64 (0.09) |
1.64 (0.08) |
0.518 |
| BMI [(Kg/m2), mean (sd)] |
25.2 (5.0) |
25.3 (4.0) |
0.637 |
| Waist circumference [cm, mean (sd)] |
90.6 (12.7) |
92.6 (10.2) |
0.174 |
| Hip circumference [cm, mean (sd)] |
96.1 (9.4) |
92.5 (6.4) |
0.005 |
| Thigh circumference [cm, mean (sd)] |
48.5 (5.5) |
47.0 (4.9) |
0.025 |
| Arm circumference [cm, mean (sd)] |
26.7 (3.2) |
27.2 (2.6) |
0.285 |
| Neck circumference [cm, mean (sd)] |
36.6 (3.8) |
37.8 (3.8) |
0.045 |
| Waist/hip circumference ratio [mean (sd)] |
0.94 (0.09) |
1.00 (0.07) |
<0.001 |
| CD4 cell count [cells/mm3, mean (sd)] |
502.7 (265.0) |
631.8 (340.8) |
0.006 |
| HIV RNA (<50) [n (%)] |
102 (87.2) |
74 (90.2) |
0.660 |
| HIV risk factor [n (%)] |
|
|
|
| Injecting drug user |
32 (27.8) |
15 (18.3) |
0.050 |
| Homosexual contact |
7 (6.1) |
14 (17.1) |
|
| Heterosexual contact |
74 (64.3) |
51 (62.2) |
|
| Others |
2 (1.7) |
2 (2.4) |
|
| CDC [n (%)] |
|
|
|
| A |
63 (54.3) |
53 (64.6) |
0.209 |
| B |
1 (0.9) |
0 (0) |
|
| C |
52 (44.8) |
29 (35.4) |
|
| ART [n (%)] |
|
|
|
| PI |
59 (51.3) |
48 (58.5) |
0.390 |
| NNRTI |
58 (50.4) |
38 (46.3) |
0.673 |
| NRTI |
112 (97.4) |
79 (96.3) |
0.695 |
| Smoking history [n (%)] |
|
|
|
| Never |
44 (37.9) |
36 (43.9) |
|
| Current |
55 (47.4) |
27 (32.9) |
|
| Former |
17 (14.7) |
19 (23.2) |
0.092 |
| Familial history of CVD [n (%)] |
51 (43.6) |
40 (48.8) |
0.563 |
| Taking medications [n (%)] |
|
|
|
| Statins |
22 (19.0) |
25 (30.5) |
0.088 |
| Fibrates |
39 (33.6) |
39 (47.6) |
0.067 |
| Oral anti-diabetics |
13 (11.2) |
16 (19.5) |
0.154 |
| Insulin |
6 (5.2) |
4 (4.9) |
1.000 |
| Anti-hypertensive drugs |
21 (17.9) |
19 (23.5) |
0.442 |
| Fat mass [%, mean (sd)] DXA |
|
|
|
| Total |
24.8 (13.1) |
19.3 (8.5) |
0.003 |
| Trunk |
25.7 (13.3) |
24.3 (9.0) |
0.446 |
| Leg |
24.4 (14.7) |
11.1 (7.4) |
<0.001 |
| Arm |
27.2 (17.1) |
20.3 (13.6) |
0.007 |
| Fat mass [Kg, mean (sd)] DXA |
|
|
|
| Total |
17.3 (11.1) |
13.2 (7.3) |
0.013 |
| Trunk |
9.3 (6.0) |
9.0 (4.8) |
0.918 |
| Leg |
5.2 (3.6) |
2.1 (1.6) |
<0.001 |
| Arm |
2.1 (1.9) |
1.5 (1.2) |
0.019 |
| Body fat mass by quantitative CT |
|
|
|
| Total fat [cm2, mean (sd)] |
282.2 (174.5) |
276.6 (124.0) |
0.865 |
| VAT [cm2, mean (sd)] |
111.5 (85.8) |
158.2 (63.2) |
<0.001 |
| SAT [cm2, mean (sd)] |
170.8 (125.7) |
118.3 (93.1) |
0.002 |
| VAT/SAT ratio [cm2, mean (sd)] |
1.08 (1.46) |
2.43 (2.62) |
<0.001 |
| Systolic blood pressure [mmHg, mean (sd)] |
120.0 (18.9) |
124.6 (15.8) |
0.039 |
| Diastolic blood pressure [mmHg, mean (sd)] |
75.8 (11.9) |
78.0 (10.6) |
0.139 |
| Leukocytes [109/L, mean (sd)] |
5.66 (1.67) |
6.39 (1.88) |
0.007 |
| Glucose 0 min [mg/dL, mean (sd)] |
104.4 (45.1) |
114.7 (44.2) |
0.003 |
| Glucose 2 hours [mg/dL, mean (sd)] |
123.6 (42.9) |
139.2 (50.3) |
0.051 |
| Insulin 0 min [μU/mL, mean (sd)] |
9,49 (10.28) |
13.00 (10.68) |
0.002 |
| Insulin 2 hours [μU/mL, mean (sd)] |
52.43 (46.65) |
91.32 (147,24) |
0.007 |
| HOMA [mean (sd)] |
2,54 (2.90) |
3.73 (3.31) |
<0.001 |
| A1c [% mean (sd)] |
5.50 (1.06) |
5.77 (0.06) |
0.001 |
| Total cholesterol [mg/dL, mean (sd)] |
218.6 (53.2) |
233.6 (61.0) |
0.093 |
| LDL-cholesterol [mg/dL, mean (sd)] |
126.1 (47.1) |
132.3 (50.7) |
0.461 |
| HDL-cholesterol [mg/dL, mean (sd)] |
47.0 (14.4) |
44.3 (12.0) |
0.262 |
| Non-HDL cholesterol [mg/dL, mean (sd)] |
171.6 (48.9) |
189.3 (56.5) |
0.019 |
| Triglycerides[mg/dL, mean (sd)] |
247.5 (170.9) |
307.2 (198.5) |
0.006 |
| Apo A1 [mg/dL, mean (sd)] |
118.8 (25.8) |
114.3 (18.3) |
0.204 |
| Apo B [mg/dL, mean (sd)] |
104.7 (26.7) |
106.1 (25.4) |
0.827 |
| Ratio apo B/apo A1 [mean (sd)] |
0.91 (0.27) |
0.95 (0.25) |
0.297 |
| Lp (a) [mg/dL, mean (sd)] |
30.2 (31.2) |
31.1 (39.7) |
0.421 |
| Homocysteine [μmol/L, mean (sd)] |
9.6 (4.1) |
9.8 (3.7) |
0.435 |
| CRP [mg/L, mean (sd)] |
5.4 (12.9) |
4.0 (4.2) |
0.913 |
| hsCRP [mg/dL, mean (sd)] |
0.48 (0.91) |
0.37 (0.28) |
0.185 |
| Lactates [mmol/L, mean (sd)] |
1.12 (0.47) |
1.36 (0.58) |
0.001 |
| NT-ProBNP [pg/mL, mean (sd)] |
39.1 (67.3) |
28.6 (27.1) |
0.414 |
| Fibrinogen [mg/dL, mean (sd)] |
344.8 (98.3) |
336.2 (92.1) |
0.463 |
| Microalbumin [mg/L, mean (sd)] |
49.1 (150.6) |
26.0 (67.7) |
0.435 |
| Uric acid [mg/L, mean (sd)] |
44.4 (15.2) |
51.2 (15.4) |
<0.001 |
| Carotid IMT [mm, mean (sd)] | 0.76 (0.25) | 0.81 (0.24) | 0.037 |
(L – Lipodystrophy FMR defined; CDC – Centers for Disease Control and Prevention criteria for staging of HIV infection; cART – combined antiretroviral therapy; BMI – body mass index; FMR – fat mass ratio; CVD – cardiovascular disease; DXA – dual-energy X-ray absorptiometry; CT – computed tomography; PI – protease inhibitor; NNRTI – non-nucleoside reverse transcriptase inhibitor; NRTI – nucleoside reverse transcriptase inhibitor, VAT – visceral adipose tissue, SAT – subcutaneous adipose tissue, IMT – intima-media thickness).
Patients with lipodystrophy were older, had been infected with HIV for a longer time and had a greater length of cART. No differences in weight, height, BMI, waist and arm circumferences among patients with, or without lipodystrophy, were observed. Patients with lipodystrophy had lower hip and thigh circumferences, but higher neck circumference and a higher waist/hip circumference ratio than those without lipodystrophy. Furthermore, patients with lipodystrophy had a higher systolic blood pressure and leukocyte count and a mean CD4+ cell count.
No differences were observed between patients with, and without, lipodystrophy regarding viral suppression rate, HIV risk factor, CDC classification and ART regimens, smoking history, family history of CV disease and medication history (statins, fibrates, oral anti-diabetics, insulin and anti-hypertension drugs).
Body composition by DXA
In the evaluation of body composition by DXA, patients with lipodystrophy had a lower total, leg and arm fat mass, both in terms of % and Kg. No difference was observed in trunk fat mass (in % and Kg) between the two groups.
Patients with lipodystrophy had a higher VAT and VAT/SAT ratio, lower SAT and no significant difference in total fat at abdominal level.
Metabolic parameters
Patients with lipodystrophy had higher glucose and insulin at 0 minutes, and insulin at 120 minutes on OGTT, HOMA, non-HDL cholesterol, triglycerides, uric acid, and lactates, than patients without lipodystrophy. No significant differences were found in the 2-hour value of glucose on OGTT, total cholesterol, LDL-cholesterol, HDL-cholesterol, apo A1, apo B, ratio Apo B/Apo A1, Lp(a), homocysteine, CRP, hsCRP, NT-ProBNP, fibrinogen and microalbumin urinary excretion between the two groups.
Carotid IMT measurements
Carotid IMT was higher in patients with lipodystrophy, than in patients without lipodystrophy [mean (SD) 0.81 (0.24) vs. 0.76 (0.25); p = 0.037)] (Figure 1).
Figure 1.
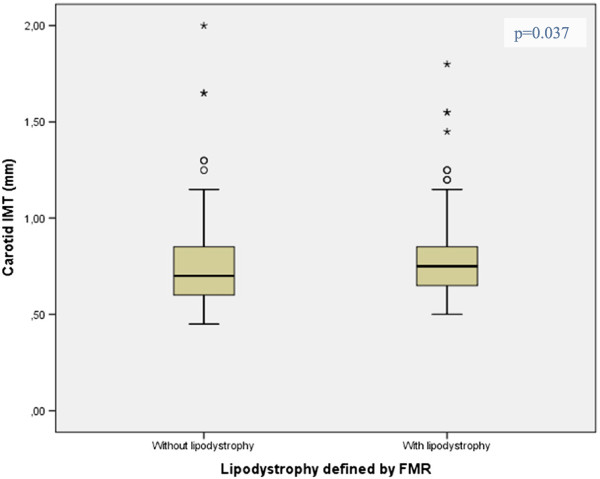
Mean differences of carotid IMT by the presence of lipodystrophy defined by FMR.
Carotid IMT correlated positively with lipodystrophy evaluated by FMR, age, waist/hip ratio, neck circumference, trunk fat mass evaluated by DXA, visceral obesity defined by total abdominal fat, VAT and VAT/SAT ratio, systolic blood pressure, glucose at 0 and 120 minutes on OGTT, A1c, non-HDL cholesterol, uric acid, CRP, hsCRP and homocysteine. No significant correlations were found between IMT and duration of HIV infection, length of cART, thigh circumference, total, leg and arm fat mass evaluated by DXA, CD4 cell count, leukocyte, insulin at 0 and 120 minutes on OGTT, HOMA, triglycerides, and lactates (Table 2).
Table 2.
Correlations between cIMT and body composition and metabolic parameters
| Correlations between cIMT and | R | P |
|---|---|---|
| Age |
0.709 |
<0.001 |
| Duration of HIV infection |
−0.019 |
0.779 |
| cART |
0.024 |
0.727 |
| Waist/hip ratio |
0.387 |
<0.001 |
| Thigh circumference |
−0.095 |
0.169 |
| Neck circumference |
0.202 |
0.007 |
| CD4 cell count |
−0.027 |
0.701 |
| Systolic blood pressure |
0.419 |
<0.001 |
| Leukocytes |
−0.049 |
0.478 |
| Glucose 0 min |
0.284 |
<0.001 |
| Glucose 2 hours OGTT |
0.220 |
0.006 |
| Insulin 0 min |
0.026 |
0.711 |
| Insulin 2 hours OGTT |
−0.089 |
0.271 |
| HOMA |
0.094 |
0.185 |
| A1c |
0.285 |
<0.001 |
| Triglycerides |
0.109 |
0.113 |
| Non-HDL cholesterol |
0.254 |
<0.001 |
| CRP |
0.196 |
0.005 |
| hsCRP |
0.334 |
0.003 |
| Homocysteine |
0.150 |
0.032 |
| Uric acid |
0.146 |
0.034 |
| Lactates |
0.081 |
0.253 |
| Fat mass total |
0.084 |
0.236 |
| Trunk |
0.168 |
0.018 |
| Leg |
−0.037 |
0.604 |
| Arm |
0.029 |
0.686 |
| Total fat on abdominal CT scan |
0.218 |
0.002 |
| VAT on abdominal CT scan |
0.418 |
<0.001 |
| SAT on abdominal CT scan |
−0.009 |
0.901 |
| VAT/SAT ratio on abdominal CT scan |
0.290 |
<0.001 |
| FMR | 0.250 | p < 0.001 |
(IMT – intima-media thickness; cART – combined antiretroviral therapy; CDC – Centers for Disease Control and Prevention criteria for staging of HIV infection; cART – combined antiretroviral therapy; OGTT – oral glucose tolerance test; HOMA – the homeostasis model assessment of insulin resistance; HDL-high density cholesterol; CPR –C protein reactive; VAT – visceral adipose tissue; SAT – subcutaneous adipose tissue; CT – computed tomography; FMR – fat mass ratio).
p = 0.037.
Using generalized linear models, cIMT means were adjusted for age, and no significant differences remained after this adjustment when patients with, and without, lipodystrophy were compared. The age adjusted mean of cIMT was 0.787 (95% CI: 0.751-0.823) in patients without lipodystrophy, and 0.775 (95% CI: 0.732-0.817) in patients with lipodystrophy (p = 0.671).
Discussion
Our aim was to evaluate the association between objectively defined lipodystrophy and cIMT. Prior studies that had evaluated the effect of lipodystrophy on cIMT, had conflicting results [20-22]. We found that cIMT was higher in patients with lipodystrophy defined by FMR, than in patients without lipodystrophy [0.81 (0.24) vs. 0.76 (0.25); p = 0.037)]. Coll et al. showed that the presence of lipodystrophy defined by clinical parameters increased by 3-fold the risk of sub-clinical carotid atherosclerosis in patients with HIV-infection [21]. On the other hand, Mercié et al. showed a significant association between cIMT and lipodystrophy in a univariate analysis, but the effect disappeared in the multivariate model [20]. Coll et al. suggested that this discrepancy of results was due to the younger and healthier population of the latter, since the mean cIMT was 0.54 mm (range 0.50-0.60), while in the Coll’s samples, the mean cIMT was 0.80 (range 0.40-1.80). In Coll’s study, the mean age of the patients with lipodystrophy was 42.38 (1.09) years while in Mercié’s it was 43.7 (8.3) years. The mean age of Coll’s patients without lipodystrophy was 40.59 (0.75), while in the Mercié et al’s study, it was 39.4 (8.7) years. Our patients, either with lipodystrophy [49.2 (10.2) years], or without lipodystrophy [44.8 (12.1) years], were older than those of these previous published studies. Despite being older than those of Coll et al., our patients had a mean cIMT identical to Coll’s patients [with lipodystrophy cIMT 0.88 (0.04) vs. without lipodystrophy 0.76 (0.02) mm; p = 0.007], but similar to Mercié’s study, no significant differences remained after adjustment for age.
Visceral obesity is another independent risk factor for CVD in the background population [23] and independent associations of obesity and abdominal adiposity with cIMT were observed [24]. We also found that cIMT was positively correlated with waist/hip ratio, neck circumference, and trunk fat mass evaluated by DXA and visceral obesity defined by total abdominal fat, VAT and VAT/SAT ratio by CT scan. However, the mechanisms by which obesity is linked to early carotid atherosclerosis are not clearly established, even though the role of metabolic factors, such as insulin resistance and altered plasma adiponectin levels, has been proposed. Yet body composition and fat distribution may influence systemic hemodynamics - both systemic blood pressure and total blood volume [25].
Insulin resistance has been independently associated with vascular disease and accelerated CV disease in HIV-infected adults [26]. In our sample, patients with lipodystrophy had higher glucose and insulin at 0 and 120 minutes on OGTT, and greater HOMA than patients without lipodystrophy. Carotid IMT correlated positively with glucose at 0 and at 120 minutes on OGTT and A1c. Despite the higher insulin resistance evaluated by HOMA, no significant correlations were observed between cIMT and HOMA.
Some studies have demonstrated that traditional CV risk factors overshadow the role of HIV infection and/or cART, and that they are the major determinants of cIMT progression [4,27-30]. Sankatsing et al. have shown that HIV infection and/or cART were associated with increased cIMT independent of traditional CV risk factors [31], and Lekakis et al. pointed to the combination of all parameters [32]. Older age is a traditional CV risk factor, associated with higher mean cIMT and a higher prevalence of carotid lesions [30,33]. We also found that cIMT correlated positively with age. As with Mercié’s study, cIMT was significantly associated with age and also with waist- to-hip ratio, systolic BP, non-HDL cholesterol, glucose disorders and homocysteine.
Adverse lipid and metabolic changes associated with HIV infection or cART exposure may be important pro-inflammatory factors [34], and plasma lipid alterations have been associated with an increased cIMT [35]. We found that cIMT was positively correlated with non-HDL cholesterol and was also positively correlated with systolic blood pressure. Similar to Mercié et al., we also observed an association between total plasma homocysteine and cIMT in HIV-infected patients subject to cART, as was previously demonstrated in non-infected patients [20].
It should be noted that certain “classical” vascular risk factors are over-represented in the HIV-infected population, e.g. smoking. However, we observed no differences between patients with, and without, lipodystrophy, with regards to smoking history. Also, no differences were observed between patients with, and without, lipodystrophy, with regards to viral suppression rate, HIV risk factor, CDC classification and ART regimens, family history of cardiovascular disease, and also medications taken (oral anti-diabetic drugs, insulin and anti-hypertension drugs). Statins are known to have beneficial effects on the arterial wall [36], but, once again, no differences were observed with those taking statins and fibrates.
In HIV-negative patients, both leukocyte count and CRP and hsCRP have been linked to endothelial dysfunction and future CV events [37,38]. Similar to Hsue, we found that hsCRP was associated with cIMT. However, in Hsue’s study, after adjusting for all traditional risk factors, the association between hsCRP and cIMT was no longer significant [39].
Study limitations
The limitations of this study are mainly related to the observational design and the cross-sectional nature of our analyses, which preclude any conclusions regarding causality. Subclinical atherosclerosis evaluated by carotid IMT, reflects the cumulative effects of risk factors acting over many years, whereas we measured risk factors at only one point in time. Thus, blood lipid concentrations, blood pressure, smoking habits and other CV risks estimated at one point in time, may not accurately represent lifetime exposure. On the other hand, we only used a qualitative assessment of smoking habits and not a quantitative one. Moreover, cART, CD4 + T-cell count, HIV viral load, and CVD risk mediators are dynamic variables which change over time.
Some aspects of our study need to be highlighted. Firstly, we only used objective methods for the evaluation of body composition: the presence of lipodystrophy was defined by FMR by DXA and visceral obesity by a CT scan. Secondly, this is one of the first reports in which cIMT was used as an outcome. And thirdly, we emphasize that increased cIMT could be a predictor of clinical cardiovascular endpoints, namely, coronary and cerebrovascular ones [18].
Conclusions
HIV-infected patients under cART with FMR defined lipodystrophy had a significantly higher cIMT when compared with patients without lipodystrophy. Carotid IMT in a univariate analyses was positively associated with lipodystrophy defined by FMR, VAT, VAT/SAT ratio, age and other classical cardiovascular risk factors. Visceral adipose tissue had an impact on cIMT in HIV-patients subject to cART, but no significant associations remained when this was adjusted for age.
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
PF conceived the study, participated in its design, in the acquisition of data, and drafted the manuscript; DC conceived the study, participated in its design, and drafted the manuscript; ACS performed the statistical analysis and critically revised the manuscript; AJM performed the CT scans and reviewed the data; JP performed DXA scans and reviewed the data; EM and AS critically revised the manuscript; JLM revised the study design. All authors read and approved the final manuscript.
Pre-publication history
The pre-publication history for this paper can be accessed here:
Contributor Information
Paula Freitas, Email: paula_freitas@sapo.pt.
Davide Carvalho, Email: davideccarvalho@netcabo.pt.
Ana Cristina Santos, Email: acsantos@med.up.pt.
António José Madureira, Email: ajbmadureira@gmail.com.
Esteban Martinez, Email: esteban@fundsoriano.es.
Jorge Pereira, Email: jorgepgpereira@gmail.com.
António Sarmento, Email: antonio.sarmento@hsjoao.min-saude.pt.
José Luís Medina, Email: jlmedina40@gmail.com.
Acknowledgements
We thank Alberto Santos for performing the DXA measurements.
Funding
Research Fellowship Dr. Manuel Almeida Ruas, Portuguese Society of Diabetology. Research Fellowship from the Portuguese Association for Clinical Study of AIDS. Research Grant to support doctoral studies in the area of HIV/AIDS, GlaxoSmithKline Foundation of Health Sciences.
References
- Mangili A, Gerrior J, Tang AM, O’Leary DH, Polak JK, Schaefer EJ, Gorbach SL, Wanke CA. Risk of cardiovascular disease in a cohort of HIV-infected adults: a study using carotid intima-media thickness and coronary artery calcium score. Clin Infect Dis. 2006;14(11):1482–1489. doi: 10.1086/509575. [DOI] [PubMed] [Google Scholar]
- Lewis W. Atherosclerosis in AIDS: potential pathogenetic roles of antiretroviral therapy and HIV. J Mol Cell Cardiol. 2000;14(12):2115–2129. doi: 10.1006/jmcc.2000.1271. [DOI] [PubMed] [Google Scholar]
- Maggi P, Serio G, Epifani G, Fiorentino G, Saracino A, Fico C, Perilli F, Lillo A, Ferraro S, Gargiulo M, Maggi P, Serio G, Epifani G, Fiorentino G, Saracino A, Fico C, Perilli F, Lillo A, Ferraro S, Gargiulo M, Chirianni A, Angarano G, Regina G, Pastore G. Premature lesions of the carotid vessels in HIV-1-infected patients treated with protease inhibitors. AIDS. 2000;14(16):F123–128. doi: 10.1097/00002030-200011100-00001. [DOI] [PubMed] [Google Scholar]
- de Saint ML, Vandhuick O, Guillo P, Bellein V, Bressollette L, Roudaut N, Amaral A, Pasquier E. Premature atherosclerosis in HIV positive patients and cumulated time of exposure to antiretroviral therapy (SHIVA study) Atherosclerosis. 2006;14(2):361–367. doi: 10.1016/j.atherosclerosis.2005.06.049. [DOI] [PubMed] [Google Scholar]
- Currier JS, Kendall MA, Zackin R, Henry WK, Alston-Smith B, Torriani FJ, Schouten J, Mickelberg K, Li Y, Hodis HN. Carotid artery intima-media thickness and HIV infection: traditional risk factors overshadow impact of protease inhibitor exposure. AIDS. 2005;14(9):927–933. doi: 10.1097/01.aids.0000171406.53737.f9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Friis-Moller N, Weber R, Reiss P, Thiebaut R, Kirk O, d’Arminio Monforte A, Pradier C, Morfeldt L, Mateu S, Law M, Friis-Moller N, Weber R, Reiss P, Thiebaut R, Kirk O, D'Arminio Monforte A, Pradier C, Morfeldt L, Mateu S, Law M, El-Sadr W, De Wit S, Sabin CA, Phillips AN, Lundgren JD. DAD study group. Cardiovascular disease risk factors in HIV patients-association with antiretroviral therapy. Results from the DAD study. AIDS. 2003;14(8):1179–1193. doi: 10.1097/01.aids.0000060358.78202.c1. [DOI] [PubMed] [Google Scholar]
- Freitas P, Carvalho D, Souto S, Santos AC, Xerinda S, Marques R, Martinez E, Sarmento A, Medina JL. Impact of lipodystrophy on the prevalence and components of metabolic syndrome in HIV-infected patients. BMC Infect Dis. 2011;14(1):246. doi: 10.1186/1471-2334-11-246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Castro KG, Ward JW, Slutsker L, Buehler JW, Jaffe HW, Berkelman RL. National Center for Infectious Diseases Division of HIV/AIDS. 1993 Revised Classification System for HIV Infection and Expanded Surveillance Case Definition for AIDS Among Adolescents and Adults. Morb Mortal Wkly Rep. 1992;14:1–19. [PubMed] [Google Scholar]
- Freitas P, Carvalho D, Santos AC, Mesquita J, Correia F, Xerinda S, Marques R, Martinez E, Sarmento A, Medina JL. Assessment of body fat composition disturbances by bioimpedance analysis in HIV-infected adults. J Endocrinol Invest. 2011;14(10):e321–9. doi: 10.3275/7841. [DOI] [PubMed] [Google Scholar]
- WHO. Report of a WHO Expert Committe. Geneva: World Health Organization; 1995. Physical Status: The Use And Interpretation Of Anthropometry. [PubMed] [Google Scholar]
- Bonnet E, Delpierre C, Sommet A, Marion-Latard F, Herve R, Aquilina C, Labau E, Obadia M, Marchou B, Massip P, Bonnet E, Delpierre C, Sommet A, Marion-Latard F, Herve R, Aquilina C, Labau E, Obadia M, Marchou B, Massip P, Perret B, Bernard J. Total body composition by DXA of 241 HIV-negative men and 162 HIV-infected men: proposal of reference values for defining lipodystrophy. J Clin Densitom. 2005;14(3):287–292. doi: 10.1385/jcd:8:3:287. [DOI] [PubMed] [Google Scholar]
- Freitas P, Santos AC, Carvalho D, Pereira J, Marques R, Martinez E, Sarmento A, Medina JL. Fat mass ratio: an objective tool to define lipodystrophy in HIV-infected patients under antiretroviral therapy. J Clin Densitom. 2010;14(2):197–203. doi: 10.1016/j.jocd.2010.01.005. [DOI] [PubMed] [Google Scholar]
- Yoshizumi T, Nakamura T, Yamane M, Islam AH, Menju M, Yamasaki K, Arai T, Kotani K, Funahashi T, Yamashita S, Yoshizumi T, Nakamura T, Yamane M, Islam AH, Menju M, Yamasaki K, Arai T, Kotani K, Funahashi T, Yamashita S, Matsuzawa Y. Abdominal fat: standardized technique for measurement at CT. Radiology. 1999;14(1):283–286. doi: 10.1148/radiology.211.1.r99ap15283. [DOI] [PubMed] [Google Scholar]
- van der Kooy K, Seidell JC. Techniques for the measurement of visceral fat: a practical guide. Int J Obes Relat Metab Disord. 1993;14(4):187–196. [PubMed] [Google Scholar]
- World Health Organization. Report of WHO Consultation. Geneva; 1999. Definition, Diagnosis And Classification Of Diabetes Mellitus And Its Complications. [Google Scholar]
- Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia. 1985;14(7):412–419. doi: 10.1007/BF00280883. [DOI] [PubMed] [Google Scholar]
- Polak JF, O’Leary DH, Kronmal RA, Wolfson SK, Bond MG, Tracy RP, Gardin JM, Kittner SJ, Price TR, Savage PJ. Sonographic evaluation of carotid artery atherosclerosis in the elderly: relationship of disease severity to stroke and transient ischemic attack. Radiology. 1993;14(2):363–370. doi: 10.1148/radiology.188.2.8327679. [DOI] [PubMed] [Google Scholar]
- O’Leary DH, Polak JF, Kronmal RA, Manolio TA, Burke GL, Wolfson SK Jr. Carotid-artery intima and media thickness as a risk factor for myocardial infarction and stroke in older adults. Cardiovascular Health Study Collaborative Research Group. N Engl J Med. 1999;14(1):14–22. doi: 10.1056/NEJM199901073400103. [DOI] [PubMed] [Google Scholar]
- Mangili A, Jacobson DL, Gerrior J, Polak JF, Gorbach SL, Wanke CA. Metabolic syndrome and subclinical atherosclerosis in patients infected with HIV. Clin Infect Dis. 2007;14(10):1368–1374. doi: 10.1086/516616. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mercie P, Thiebaut R, Lavignolle V, Pellegrin JL, Yvorra-Vives MC, Morlat P, Ragnaud JM, Dupon M, Malvy D, Bellet H, Mercie P, Thiebaut R, Lavignolle V, Pellegrin JL, Yvorra-Vives MC, Morlat P, Ragnaud JM, Dupon M, Malvy D, Bellet H, Lawson-Ayayi S, Roudaut R, Dabis F. Evaluation of cardiovascular risk factors in HIV-1 infected patients using carotid intima-media thickness measurement. Ann Med. 2002;14(1):55–63. doi: 10.1080/078538902317338652. [DOI] [PubMed] [Google Scholar]
- Coll B, Parra S, Alonso-Villaverde C, de Groot E, Aragones G, Montero M, Tous M, Camps J, Joven J, Masana L. HIV-infected patients with lipodystrophy have higher rates of carotid atherosclerosis: the role of monocyte chemoattractant protein-1. Cytokine. 2006;14(1–2):51–55. doi: 10.1016/j.cyto.2006.03.013. [DOI] [PubMed] [Google Scholar]
- van Vonderen MG, Smulders YM, Stehouwer CD, Danner SA, Gundy CM, Vos F, Reiss P, Agtmael MA. Carotid intima-media thickness and arterial stiffness in HIV-infected patients: the role of HIV, antiretroviral therapy, and lipodystrophy. J Acquir Immune Defic Syndr. 2009;14(2):153–161. doi: 10.1097/QAI.0b013e31819367cd. [DOI] [PubMed] [Google Scholar]
- Hubert HB, Feinleib M, McNamara PM, Castelli WP. Obesity as an independent risk factor for cardiovascular disease: a 26-year follow-up of participants in the Framingham Heart Study. Circulation. 1983;14(5):968–977. doi: 10.1161/01.cir.67.5.968. [DOI] [PubMed] [Google Scholar]
- Burke GL, Bertoni AG, Shea S, Tracy R, Watson KE, Blumenthal RS, Chung H, Carnethon MR. The impact of obesity on cardiovascular disease risk factors and subclinical vascular disease: the Multi-Ethnic Study of Atherosclerosis. Arch Intern Med. 2008;14(9):928–935. doi: 10.1001/archinte.168.9.928. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kozakova M, Palombo C, Paterni M, Anderwald CH, Konrad T, Colgan MP, Flyvbjerg A, Dekker J. Body composition and common carotid artery remodeling in a healthy population. J Clin Endocrinol Metab. 2008;14(9):3325–3332. doi: 10.1210/jc.2007-2484. [DOI] [PubMed] [Google Scholar]
- Martinez E, Larrousse M, Gatell JM. Cardiovascular disease and HIV infection: host, virus, or drugs? Curr Opin Infect Dis. 2009;14(1):28–34. doi: 10.1097/QCO.0b013e328320a849. [DOI] [PubMed] [Google Scholar]
- Bongiovanni M, Casana M, Cicconi P, Pisacreta M, Codemo R, Pelucchi M, d’Arminio Monforte A, Bini T. Predictive factors of vascular intima media thickness in HIV-positive subjects. J Antimicrob Chemother. 2008;14(1):195–199. doi: 10.1093/jac/dkm414. [DOI] [PubMed] [Google Scholar]
- Mercie P, Thiebaut R, Aurillac-Lavignolle V, Pellegrin JL, Yvorra-Vives MC, Cipriano C, Neau D, Morlat P, Ragnaud JM, Dupon M, Mercie P, Thiebaut R, Aurillac-Lavignolle V, Pellegrin JL, Yvorra-Vives MC, Cipriano C, Neau D, Morlat P, Ragnaud JM, Dupon M, Bonnet F, Lawson-Ayayi S, Malvy D, Roudaut R, Dabis F. Groupe d'Epidemiologie Clinique du Sida en Aquitaine. Carotid intima-media thickness is slightly increased over time in HIV-1-infected patients. HIV Med. 2005;14(6):380–387. doi: 10.1111/j.1468-1293.2005.00324.x. [DOI] [PubMed] [Google Scholar]
- Johnsen S, Dolan SE, Fitch KV, Kanter JR, Hemphill LC, Connelly JM, Lees RS, Lee H, Grinspoon S. Carotid intimal medial thickness in human immunodeficiency virus-infected women: effects of protease inhibitor use, cardiac risk factors, and the metabolic syndrome. J Clin Endocrinol Metab. 2006;14(12):4916–4924. doi: 10.1210/jc.2006-1140. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hsue PY, Lo JC, Franklin A, Bolger AF, Martin JN, Deeks SG, Waters DD. Progression of atherosclerosis as assessed by carotid intima-media thickness in patients with HIV infection. Circulation. 2004;14(13):1603–1608. doi: 10.1161/01.CIR.0000124480.32233.8A. [DOI] [PubMed] [Google Scholar]
- Sankatsing RR, Wit FW, Vogel M, de Groot E, Brinkman K, Rockstroh JK, Kastelein JJ, Stroes ES, Reiss P. Increased carotid intima-media thickness in HIV patients treated with protease inhibitors as compared to non-nucleoside reverse transcriptase inhibitors. Atherosclerosis. 2009;14(2):589–595. doi: 10.1016/j.atherosclerosis.2008.05.028. [DOI] [PubMed] [Google Scholar]
- Lekakis J, Tsiodras S, Ikonomidis I, Palios J, Poulakou G, Rallidis L, Antoniadou A, Panagopoulos P, Papadopoulos A, Giamarellou H, Lekakis J, Tsiodras S, Ikonomidis I, Palios J, Poulakou G, Rallidis L, Antoniadou A, Panagopoulos P, Papadopoulos A, Giamarellou H, Kremastinos DT. HIV-positive patients treated with protease inhibitors have vascular changes resembling those observed in atherosclerotic cardiovascular disease. Clin Sci (Lond) 2008;14(6):189–196. doi: 10.1042/CS20070353. [DOI] [PubMed] [Google Scholar]
- Kaplan RC, Kingsley LA, Gange SJ, Benning L, Jacobson LP, Lazar J, Anastos K, Tien PC, Sharrett AR, Hodis HN. Low CD4+ T-cell count as a major atherosclerosis risk factor in HIV-infected women and men. AIDS. 2008;14(13):1615–1624. doi: 10.1097/QAD.0b013e328300581d. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boger MS, Shintani A, Redhage LA, Mitchell V, Haas DW, Morrow JD, Hulgan T. Highly sensitive C-reactive protein, body mass index, and serum lipids in HIV-infected persons receiving antiretroviral therapy: a longitudinal study. J Acquir Immune Defic Syndr. 2009;14(4):480–487. doi: 10.1097/qai.0b013e3181b939e5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Seminari E, Pan A, Voltini G, Carnevale G, Maserati R, Minoli L, Meneghetti G, Tinelli C, Testa S. Assessment of atherosclerosis using carotid ultrasonography in a cohort of HIV-positive patients treated with protease inhibitors. Atherosclerosis. 2002;14(2):433–438. doi: 10.1016/s0021-9150(01)00736-5. [DOI] [PubMed] [Google Scholar]
- Kastelein JJ, de Groot E, Sankatsing R. Atherosclerosis measured by B-mode ultrasonography: effect of statin therapy on disease progression. Am J Med. 2004;14(Suppl 6A):31S–36S. doi: 10.1016/j.amjmed.2004.02.009. [DOI] [PubMed] [Google Scholar]
- van Wijk JP, de Koning EJ, Cabezas MC, Joven J, op’t Roodt J, Rabelink TJ, Hoepelman AM. Functional and structural markers of atherosclerosis in human immunodeficiency virus-infected patients. J Am Coll Cardiol. 2006;14(6):1117–1123. doi: 10.1016/j.jacc.2005.09.073. [DOI] [PubMed] [Google Scholar]
- Mangili A, Polak JF, Quach LA, Gerrior J, Wanke CA. Markers of atherosclerosis and inflammation and mortality in patients with HIV infection. Atherosclerosis. 2011;14(2):468–473. doi: 10.1016/j.atherosclerosis.2010.11.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hsue PY, Hunt PW, Sinclair E, Bredt B, Franklin A, Killian M, Hoh R, Martin JN, McCune JM, Waters DD, Hsue PY, Hunt PW, Sinclair E, Bredt B, Franklin A, Killian M, Hoh R, Martin JN, McCune JM, Waters DD, Deeks SG. Increased carotid intima-media thickness in HIV patients is associated with increased cytomegalovirus-specific T-cell responses. AIDS. 2006;14(18):2275–2283. doi: 10.1097/QAD.0b013e3280108704. [DOI] [PubMed] [Google Scholar]