

Abstract
We experienced a case of intussusception caused by cystic lymphangioma of the colon in a 32 years old female who was admitted to our hospital for the chief complaint of bloody stool. In the colonoscopic examination, cystic mass with stalk which had smooth mucosal surface was noted at the descending colon. Abdominal ultrasonography and computed tomography revealed left colon intussusception with a multilocular cystic tumor as a leading point. Emergent operation was performed. On the histopathologic examination, the cystically dilated spaces lined by endothelium and septated by fibrous septa were present. The pathological diagnosis was cystic lymphangioma of the colon. Although intussusception due to lymphangioma in an adult are rare, it should be taken into consideration that it is possible diagnosis.
Keywords: Cystic lymphangioma of the colon, Adult intussusception
INTRODUCTION
Lymphangioma is a benign tumor consisting of several expanded lymphatics, each lymphatics is surrounded by benign endothelial cells and it could be developed in any parts of the body. However, it is developed primarily in the neck, the axillary area, the scapula and other areas where lymphatic organs are abundant[1,2]. Lymphangioma is hardly developed in the digestive organs and the development of the colon is very rare. It was reported for the first time by Chisholm and Hillkowitz in 1932 and recently, with the increased application of colonoscopy and endoscopic ultrasonography, these cases are on the rise[4,5]. We report a case who was diagnosed as intussusception due to cystic lymphangioma by abdominal ultrasound, computed tomography and colonoscopy.
CASE REPORT
A 32-year-old female was admitted to our hospital due to bloody stool for 3 d. In her past, family and social history, specific findings were not detected. At the time of visit, blood pressure of 100/60 mmHg, pulse rate of 76 per min and body temperature of 36.7 °C was recorded. In physical examination, the acute ill appearance was detected and she were conscious. The conjunctiva was pale and the head-neck lymph node was not palpated. In abdominal examination, the liver or the spleen was not palpated and the bowel sound was normal. But, left lower quadrant pain was detected, however, the rebound tenderness was not detected. In laboratory findings, in peripheral blood test, the number of leukocyte was 16 140/mm3, hemoglobin was 128 g/L, and platelet was 317 000/mm3. In biochemical test was all normal. CEA, CA 125 and CA 19-9 showed normal limits.
In colonoscopic examination, a cystic mass with a stalk of the descending colon was detected (Figure 1). The mass was covered with the normal mucosa with smooth surface and palpated with the tissue biopsy forceps, it was cystic that changed readily. On the next day, the patient reported severe abdominal pain and thus abdominal ultrasonography and abdominal computed tomography were performed. In abdominal ultrasonography, a cystic mass divided by several septa was detected and the situation was that intussusception by this mass (Figure 2). In abdominal computed tompgraphy, a mass was detected and in the proximal area, intussusception was detected (Figure 3). The patient underwent emergent surgery and the partial resection of the descending colon was performed. The resected specimen was a mass 2.5 cm× 3.5 cm× 5.0 cm in size and similarly to ultrasonographic finding. The specimen was a bag shape, its inside was divided into several fibrous septa and filled with clear serous liquid (Figure 4). In histological finding, the cyst was located below the mucosal membrane, the inside was surrounded by normal epithelial cells and divided by several fibrous septa (Figure 5). Based on the above findings, she was diagnosed as intussusception caused by cystic lymphangioma.
Figure 1.
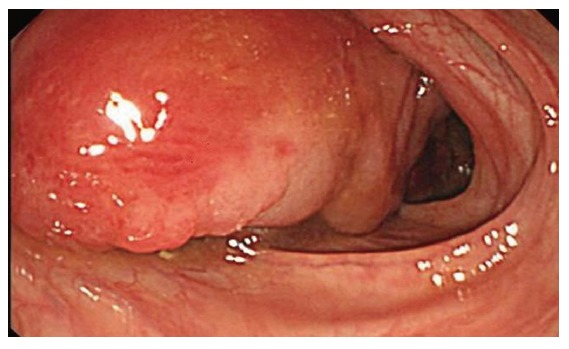
Colonoscopic examination shows a 2.5 cm x 2.5 cm x 5.0 cm sized round, smooth surfaced mass covered by normal mucosa in the descending colon. This mass is pedunclated cystic nature, and compressible pillow sign positive.
Figure 2.
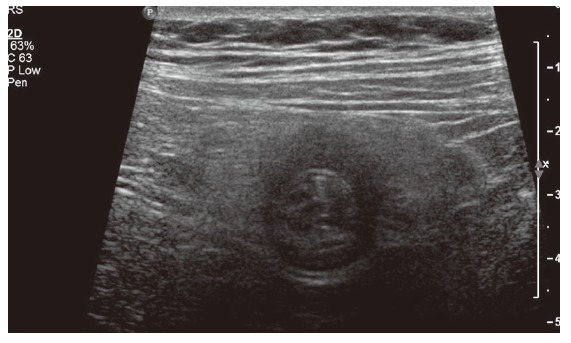
Ultrasonography of the mass shows a multilocular cystic lesion with septa.
Figure 3.
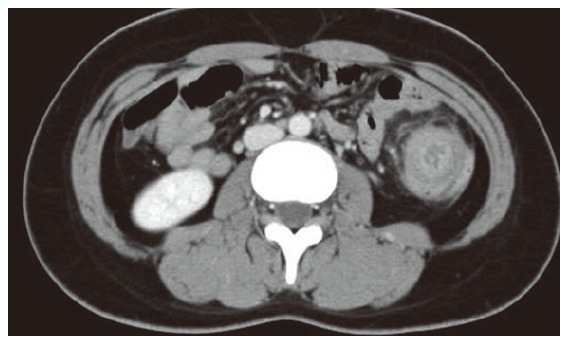
Computed tomography shows the cystic lesion in the descending colon, occupying the whole lumen, and also shows multicentric target sign and sausage-shaped inhomogeneous soft-tissue mass.
Figure 4.

Macroscopic finding of the resected specimen reveals 2.5 cm x 3.5 cm x 5.0 cm sized multiseptated submucosal cystic tumor, which changed shape easily. The tumor shows fluctuation and serous clear fluid was aspirated by needle puncture.
Figure 5.
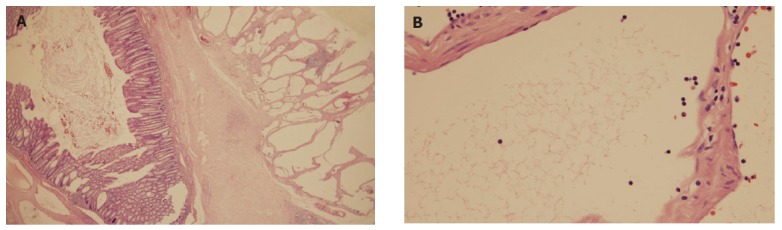
(A) Cystically dilated spaces are covered with single layer of endothelial cells and separated by fibrous septa are present in the submucosa. The overlying colonic mucosa is normal (H & E stain, x100). (B) Atypical cell are not noted, and endothelium is lined by benign cuboidal cells (H-E, original magnification, x400).
DISCUSSION
Intussusception in adults is developed relatively infrequently. They are equivalent to 1 % of colonic obstructive patients and they are equivalent to 5 - 10 % of total intussusception[1,2]. Different from in children, they occur secondarily by definite lesions. For the diagnosis of such intussusception in adults, computed tomography has been reported to be the most useful radiological method[1]. This case is a patient that intussusception is caused by the cystic lymphangioma in the descending colon. Lymphangioma within the abdominal cavity is rare, and it occupies less than 5 % of the entire lymphangioma[3]. Most reported cases are the cases detected accidentally during colonoscopy or barium enema and definitely diagnosed histologically by the resection of the lesion[5,7]. Pathophysiologically, according to its shape, it is classified into 3 types: (1) simple capillary, (2) cavernous and (3) cystic. As in our case, cystic cases are most frequent. Recently, with the increase of the application of colonoscopy, the reported cases of the lymphangioma of the colon are increased [4,5]. The findings suggesting lymphangioma are the characteristics that are the round and soft surface, a wide base area, pink color and semi-transparent. In response to the peristaltic movement or the position of patient, its shape changes and it has the characteristic that the diameter and the location change upon pressing by forceps. In our case also, it was stalked cystic and the smooth surface of mass was covered with the normal mucosa of large intestine, and palpated with the biopsy forceps, it showed the pattern of readily changing its shape. The disease should be differentiated from other mass lesions, such as lipoma, cavernous angioma, leimyoma and enteric duplication cyst. However, endoscopic findings are very diverse, subjective and it is not of help to the diagnosis. So, the confirmation of its structure by endoscopic ultrasonography is important for the differential diagnosis[6]. In ultrasonography, it is detected as a mass limited to the submucosal area, separated well from adjacent tissues, and divided by several septa and for the cases showing such findings, it could be definitely diagnosed without further tests, and for the asymptomatic cases, the follow-up observation without treatment is sufficient[7]. Occasionally, nonspecific symptoms, in other words, hemorrhage or abdominal pain may be reported, it may induce protein loss enteropathy, and intussusception may be developed by the mass[8]. Our case is also the example that the patient was admitted for bloody stool and developed intussusception on the next day. In such cases, if symptomatic or with complications, it should be removed by surgery or endoscopic resection. The indications of endoscopic polyp resection are staked masses or partially staked masses less than 2 cm in size[6]. However, in the cases of masses with a large diameter, surgical resection is required. It has been reported that generally, in the patient with intussusception, there are a large volume of hemorrhage, or protein loss enteropathy, a large mass in size, and asymptomatic patients showed a mass in a small size[9]. We experienced a case of intussusception in a 32-year-old female patient admitted for bloody stool, and it is an important causality although rare, therefore, the case is reported here together with a review of the literature.
Footnotes
S- Editor Wang J L- Editor Zhang JZ E- Editor Wu M
References
- 1.Singh S, Baboo ML, Pathak IC. Cystic lymphangioma in children: report of 32 cases including lesions atrrare sites. Surgery. 1971;69:947–951. [PubMed] [Google Scholar]
- 2.Begos DG, Sandor A, Modlin IM. The diagnosis and management of adult intussusception. Am J Surg. 1997;173:88–94. doi: 10.1016/S0002-9610(96)00419-9. [DOI] [PubMed] [Google Scholar]
- 3.Chung JH, Suh YL, Park IA, Jang JJ, Chi JG, Kim YI, Kim WH. A pathologic study of abdominal lymphangiomas. J Korean Med Sci. 1999;14:257–262. doi: 10.3346/jkms.1999.14.3.257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hatada T, Ikeda H, Tanigawa A, Fujiwara Y, Hanada Y, Yamamura T. Lymphangioma of the colon: a case report and review of the Japanese literature. Acta Gastroenterol Belg. 2000;63:239–241. [PubMed] [Google Scholar]
- 5.Kuramoto S, Sakai S, Tsuda K, Kaminishi M, Ihara O, Oohara T, Jinbo S, Murakami T. Lymphangioma of the large intestine. Report of a case. Dis Colon Rectum. 1988;31:900–905. doi: 10.1007/BF02554857. [DOI] [PubMed] [Google Scholar]
- 6.Geboes K, De Wolf-Peeters C, Rutgeerts P, Vantrappen G, Desmet V. Submucosal tumors of the colon: experience with twenty-five cases. Dis Colon Rectum. 1978;21:420–425. doi: 10.1007/BF02586719. [DOI] [PubMed] [Google Scholar]
- 7.Irisawa A, Bhutani MS. Cystic lymphangioma of the colon: endosonographic diagnosis with through-the-scope catheter miniprobe and determination of further management. Report of a case. Dis Colon Rectum. 2001;44:1040–1042. doi: 10.1007/BF02235494. [DOI] [PubMed] [Google Scholar]
- 8.Zilko PJ, Laurence BH, Sheiner H, Pollard J. Cystic lymphangiomyoma of the colon causing protein-losing enteropathy. Am J Dig Dis. 1975;20:1076–1080. doi: 10.1007/BF01071198. [DOI] [PubMed] [Google Scholar]
- 9.Matsuda T, Matsutani T, Tsuchiya Y, Okihama Y, Egami K, Yoshioka M, Maeda S, Onda M. A clinical evaluation of lymphangioma of the large intestine: a case presentation of lymphangioma of the descending colon and a review of 279 Japanese cases. J Nippon Med Sch. 2001;68:262–265. doi: 10.1272/jnms.68.262. [DOI] [PubMed] [Google Scholar]