

Abstract
Preoperative images of acute appendiceal diverticulitis are rarely reported because of the difficulty of distinguishing appendiceal diverticulitis from other iliocecal diseases like acute appendicitis or cecal diverticulitis. We report a case of preoperatively diagnosed acute appendiceal diverticulitis. A 30-year-old female with a presumptive diagnosis of acute appendicitis from history and physical examination was admitted to our hospital. Ultrasound sonography showed inflamed appendiceal diverticula and inflammatory changes of the surrounding tissue. The swollen appendix was detected but its findings were slightly different from those of typical acute appendicitis in the following points. One difference was the thickened wall of the appendix, the other difference was the presence of air in the appendix. The patient underwent appendectomy and the pathological specimen revealed inflammatory changes of diverticula within the appendix.
Keywords: Appendiceal diverticulitis, Sonography, Preoperative diagnosis
INTRODUCTION
Acute appendiceal diverticulitis is an uncommon clinical entity. Some patients treated for presumed acute appendicitis have acute vermiform appendiceal diverticulitis. Almost all acute appendiceal diverticulitis are found after appendectomy because history and physical findings of appendiceal diverticulitis closely resemble those of acute appendicitis. The preoperative images are not so effective in detecting an appendiceal diverticulum. Here, we report a case of acute appendiceal diverticulitis diagnosed preoperatively by ultrasound sonography.
CASE REPORT
A 30 year-old female was admitted to our hospital for abdominal pain, slight fever and mild anorexia. The present episode of abdominal pain began four days before admission. At first, she felt epigastralgia and by the time she arrived at the hospital the pain shifted to the right lower abdomen. Physical examination showed a body temperature of 37.4°C and localized tenderness in the right lower quadrant of abdomen. No rebound tenderness was observed. Laboratory studies demonstrated a white blood cell count of 11.0 × 109/L. Abdominal roentgenogram showed no remarkable abnormality except for a small amount of intestinal gas. Abdominal ultrasound sonography, with a 7-MHz linear-array transducer (GE LOGIC 7), demonstrated an enlarged swollen appendix with a cross section diameter of 10 mm and multiple hypoechoic small lateral pouch-like projections (Figure 1). The surrounding was enclosed by pouch like projections in the hyperechoic lesion which was thought to be caused by inflammatory changes of the mesoappendix. Wall thickening of appendix was more prominent than that seen in typical appendicitis (Figure 2). We made a diagnosis of acute appendiceal diverticulitis. The patient underwent an emergent appendectomy. The resected appendix was 14 cm long and 1.0 cm in diameter with multiple diverticula. One of the diverticula was surrounded by inflammatory tissue (Figure 3). Microscopic study revealed a pseudodiverticulum with inflammation in its wall and mesoappendix. She had an uneventful recovery and was discharged two days after surgery.
Figure 1.
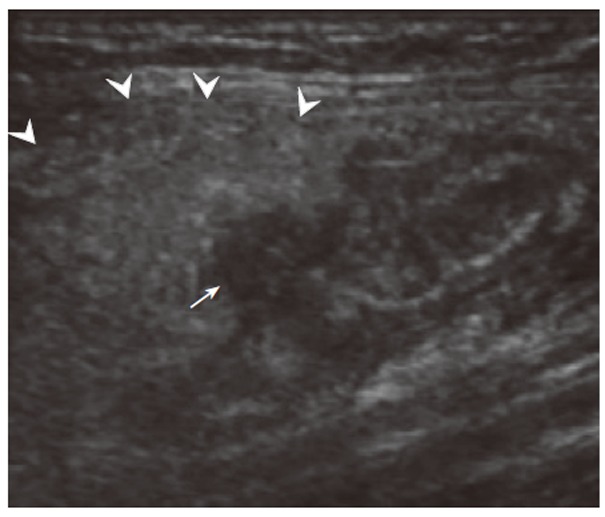
Longitudinal view of the appendix. A hyperechoic mass (arrowheads) including hypoechoic lateral pouch like lesion (arrow) is observed. Hypo lesion is appendiceal diverticula, and hyperechoic mass is inflamed adipose tissue (= mesoappendix).
Figure 2.
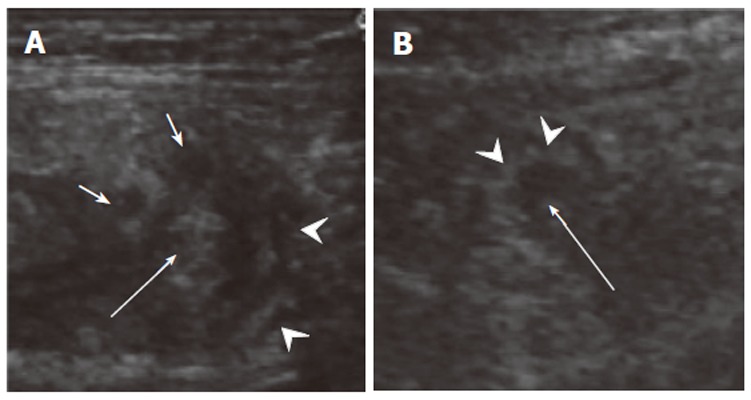
Cross section of acute appendiceal diverticulitis (A) in the present case and acute suppurative appendicitis (B) in another case. Layer structure (A: arrowheads) was found in appendiceal diverticulitis because of all inflamed layers, and inside echogenic (A: arrow) which means containing air. Multiple lateral hypoechoic projections (= diverticula) were observed. In comparison, an echogenic ring (B: arrowheads) was observed in acute appendicitis showing mucosal and submucosal inflammation, and an echo free space filled with inflammatory fluid inside it.
Figure 3.
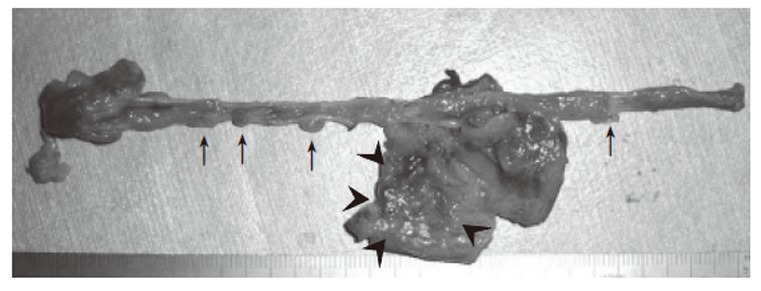
Multiple diverticuloses in the resected appendix (arrows) and peri-appendiceal inflammation (= diverticulitis) in 5 cm from the tip (arrowheads).
DISCUSSION
Appendiceal diverticulum is an uncommon clinical entity, with an incidence of 0.2%-1.5% in surgical pathologic specimens[1]. Its preoperative images have been rarely reported. Place et al[2] have reported abdominal CT findings of appendiceal diverticulitis but they could not distinguish it from cecal diverticulitis preoperatively. Macheiner et al[3] have also reported sonographic features of diverticulitis of the appendix vermiformis. According to their reports, a hypoehoic, inflamed diverticulum is surrounded by echogenic fatty tissue. This description is the same as our sonographic findings of acute appendiceal diverticulitis. Other than these findings, we found different appendiceal features of acute appendiceal diverticulitis from those of typical acute appendicitis (Figure 2). In typical suppurative acute appendicitis, edematous mucosa is observed as a cross-sectional ring of strong echo and inside it there is an echo free space filled with fluid. In comparison,the appendix wall layers are thickened and echogenic in appendiceal diverticulitis because of air in it. These findings strongly support that the main inflammation is in the appendiceal wall itself rather than in the actual appendix.
Diverticular disease of the appendix has four variations[4], namely appendiceal diverticula without inflammation, acute appendicitis with diverticula, acute appendiceal diverticulitis with acute appendicitis, and acute diverticulitis. The fourth variation is true acute appendiceal diverticulitis as the case presented here. Its sonographic features resemble those of colonic diverticulitis rather than acute appendicitis except for the enlarged appendix. We suggest that sonographyic study is useful for the early diagnosis of acute appendiceal divetticulitis.
Footnotes
S- Editor Wang J L- Editor Wang XL E- Editor Liu Y
References
- 1.COLLINS DC. A study of 50,000 specimens of the human vermiform appendix. Surg Gynecol Obstet. 1955;101:437–445. [PubMed] [Google Scholar]
- 2.Place RJ, Simmang CL, Huber PJ Jr. Appendiceal diverticulitis. South Med J. 2000;93:76–79. [PubMed] [Google Scholar]
- 3.Macheiner P, Hollerweger A, Gritzmann N. Sonographic features of diverticulitis and diverticulosis of the vermiform appendix. J Clin Ultrasound. 2002;30:456–457. doi: 10.1002/jcu.10097. [DOI] [PubMed] [Google Scholar]
- 4.Lipton S, Estrin J, Glasser I. Diverticular disease of the appendix. Surg Gynecol Obstet. 1989;168:13–16. [PubMed] [Google Scholar]