

Abstract
This is a case report of an 85-year old patient who presented with abdominal pain, nausea and vomiting associated with altered liver function test. The plain X-rays and CT scan showed pneumobilia with an ectopic gallstone. The patient was diagnosed with Bouveret syndrome and managed surgically. The report is followed by a discussion about Bouveret syndrome.
Keywords: Bouveret syndrome, Gall bladder, Stone, Fistula, Gastric outlet obstruction
INTRODUCTION
Gallstone ileus is a rare complication of gallstones but it accounts for almost 25% of non strangulated intestinal obstruction in patients above 65 years of age. Mortality has improved but remains at 15%-18% due to the age and co-morbidity of patients[1]. Bouveret syndrome, first described in 1896, is a subgroup of gallstone ileus in which a cholecystoduodenal fistula allows the passage of a stone which impacts in the duodenum and causes gastric outlet obstruction. It is rare with 175 cases reported in the literature up to the year 2000[2]. We present a case of Bouveret syndrome, with typical radiological findings, that was successfully managed surgically.
CASE REPORT
An 85-year old lady presented with a five-day history of right upper quadrant (RUQ) abdominal pain radiating to her back, associated with nausea and vomiting. On examination she had tenderness, guarding and rebound in the RUQ and epigastrium. The leukocyte count was 20.6 (predominantly neutrophils), the amylase 1039 and urea and creatinine were elevated. Plain abdominal X-ray showed a radio-opaque shadow in the right side of the abdomen, air in the gall bladder and biliary tree but no evidence of small bowel obstruction (Figure 1). She was assumed to have pancreatitis and a suspected cholecystoenteric fistula.
Figure 1.
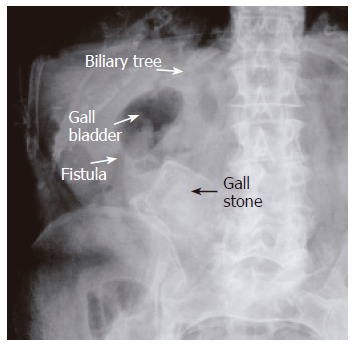
Plain X-ray showing air in the biliary tree and an ectopic bizarre-shaped gall stone suggesting the diagnosis of cholecystoenteric fistula.
CT scan with oral contrast revealed a large amount of air in the biliary tree, a fistula between the second part of duodenum and the gall bladder and a large stone in the third part of duodenum. A small amount of contrast outlined the stone and reached the small bowel (Figure 2). This impacted stone (7.5 cm × 4 cm × 4 cm) was removed surgically from the junction of the second and third part of duodenum through a small jejunostomy after mobilization of the duodenum and the DJ flexure. Her post operative recovery was uneventful.
Figure 2.
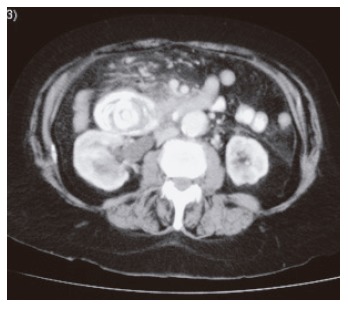
CT abdomen with contrast showing the gall stone in the duodenum with some contrast passing distal to the stone.
DISCUSSION
Cholecystoenteric fistulae occur in less than 1% of patients with gallstones. Most (60%) are cholecystoduodenal fistulae, but cholecystocolic, cholecystogastric and choledochoduodenal fistulae have been described. Large stones passing through the fistula may cause intestinal obstruction, especially in the terminal ileum[1,3]. A plain abdominal X-ray is diagnostic in about 50% of cases[3] and may demonstrate intestinal obstruction, pneumobilia, an ectopic gallstone, alteration in the position of the previously observed stone or two air fluid levels in the right upper quadrant secondary to air in the gall bladder.
Patients with Bouveret syndrome usually present with symptoms of gastric outlet obstruction, though presenting with other complications of gall stone disease or upper gastrointestinal bleeding has been reported[4]. A plain abdominal X-ray may show a dilated stomach, and CT may demonstrate pneumobilia, intestinal obstruction and an ectopic gallstone[5]. Open surgery, endoscopic removal[6] and laparoscopic or laparoscopic assisted enterolithotomy[7] have all been used successfully for stone removal. A stone in the duodenum can be difficult to access laparoscopically but may be reached endoscopically[6].
Whether the gallbladder should be disturbed is controversial but the recurrence of gallstone ileus following enterolithotomy is rare, and complications related to the persistence of a cholecystoenteric fistula are unusual[3,8].
Bouveret syndrome is a rare complication of cholelithiasis with a relatively high mortality. In the patient has a pre-operative diagnosis of Bouveret syndrome, endoscopic disimpaction should be attempted. Failing this laparotomy is likely to be required but laparoscopy may allow identification of the stone’s position minimizing subsequent skin incision.
Footnotes
S- Editor Wang J L- Editor Wang XL E- Editor Liu WF
References
- 1.1 Reisner RM, Cohen JR. Gallstone ileus: a review of 1001 reported cases. Am Surg. 1994;60:441–446. [PubMed] [Google Scholar]
- 2.Ariche A, Czeiger D, Gortzak Y, Shaked G, Shelef I, Levy I. Gastric outlet obstruction by gallstone: Bouveret syndrome. Scand J Gastroenterol. 2000;35:781–783. doi: 10.1080/003655200750023480. [DOI] [PubMed] [Google Scholar]
- 3.Clavien PA, Richon J, Burgan S, Rohner A. Gallstone ileus. Br J Surg. 1990;77:737–742. doi: 10.1002/bjs.1800770707. [DOI] [PubMed] [Google Scholar]
- 4.Salah-Eldin AA, Ibrahim MA, Alapati R, Muslah S, Schubert TT, Schuman BM. The Bouveret syndrome: an unusual cause of hematemesis. Henry Ford Hosp Med J. 1990;38:52–54. [PubMed] [Google Scholar]
- 5.Liew V, Layani L, Speakman D. Bouveret's syndrome in Melbourne. ANZ J Surg. 2002;72:161–163. doi: 10.1046/j.1445-2197.2002.02319.x. [DOI] [PubMed] [Google Scholar]
- 6.Lübbers H, Mahlke R, Lankisch PG. Gallstone ileus: endoscopic removal of a gallstone obstructing the upper jejunum. J Intern Med. 1999;246:593–597. doi: 10.1046/j.1365-2796.1999.00597.x. [DOI] [PubMed] [Google Scholar]
- 7.Sarli L, Pietra N, Costi R, Gobbi S. Gallstone ileus: laparoscopic-assisted enterolithotomy. J Am Coll Surg. 1998;186:370–371. doi: 10.1016/s1072-7515(97)00151-8. [DOI] [PubMed] [Google Scholar]
- 8.Rodríguez-Sanjuán JC, Casado F, Fernández MJ, Morales DJ, Naranjo A. Cholecystectomy and fistula closure versus enterolithotomy alone in gallstone ileus. Br J Surg. 1997;84:634–637. [PubMed] [Google Scholar]