

Abstract
Necrotizing fasciitis is a devastating soft tissue infection affecting fascias and subcutaneous soft tissues. Literature reviews have identified several related risk factors, including malignancy, alcoholism, malnutrition, diabetes, male gender and old age. There are only scanty case reports in the literature describing its rare association with colorectal malignancy. All published cases are attributed to bowel perforation resulting in necrotizing fasciitis over the perineal region. Isolated upper or lower limb diseases are rarely identified. Simultaneous upper and lower limb infection in colorectal cancer patients has never been described in the literature. We report an unusual case of multi-limb necrotizing fasciitis in a patient with underlying non-perforated rectal carcinoma.
Keywords: Necrotizing fasciitis, Soft tissue infection, Colorectal cancer, Malignancy, Group G streptococcus
INTRODUCTION
Necrotizing fasciitis is a devastating soft tissue infection affecting fascias and subcutaneous soft tissues[1]. Two distinctive clinical entities are recognized: hyperacute and subacute variants[2]. Hyperacute necrotizing fasciitis usually manifests as a rapidly progressing infection with resultant multi-organ failure due to group A streptococcus or clostridium species[3]. Contrarily, polymicrobial infection is implicated in subacute necrotizing fasciitis that represents a slowly evolving disease with less fulminant systemic complications[4]. Regarding its etiology, necrotizing soft tissue infection can be secondary to trauma, wound infections, perianal or urogenital abscesses, decubitus ulcers or idiopathic in origin[5]. Malignancy, alcoholism, malnutrition, diabetes, male gender and old age are general risk factors associated with necrotizing fasciitis[6,7]. There are only scanty case reports in the literature describing its rare association with colorectal malignancy[8-13]. All these cases are attributed to bowel perforation resulting in necrotizing fasciitis over the perineal or abdominal region. Isolated upper or lower limb diseases are exceedingly uncommon. Multi-limb necrotizing fasciitis is even rarer. We report here the first case of multi-limb involvement of necrotizing fasciitis in a patient with underlying rectal carcinoma.
CASE REPORT
A 56-year-old male patient, who had a medical history of alcoholic cirrhosis, poorly-controlled diabetes mellitus and mild renal impairment, presented with an one-month history of per rectal bleeding. Digital rectal examination revealed a non-obstructing rectal tumour situated at 8 cm above the anal verge. Tumour biopsy was taken through proctoscope and the histology confirmed it to be an adenocarcinoma. No abdominal discomfort or increase in per rectal bleeding was reported after the procedure. However, one day after the tumour biopsy, he complained of bilateral lower limb pain over the pre-existing ankle edema. He denied any previous history of trauma. No wound or skin abrasions could be identified over both lower limbs. In addition to the swollen lower limbs, he was noticed to have unexplained sinus tachycardia (pulse rate 100 per min) despite normal haemodynamic status and oxygen saturation. Examination of other organ systems was unremarkable. The arterial blood gas, white cell counts, chest radiograph and electrocardiogram were normal. Though Doppler ultrasound did not show any evidence of deep vein thrombosis in both lower limbs, low molecular weight heparin was commenced as pulmonary embolism was not excluded.
His clinical condition rapidly deteriorated over the next 24 h when he developed acute on chronic renal impairment, hypotension and worsening metabolic acidosis that necessitated inotropes and hemodialysis support in the intensive care unit. Urgent ultrasound of the abdomen did not reveal any evidence of obstructive uropathy. He became hypothermic (core temperature 32°C), drowsy and mentally confused. Blood parameters revealed marked leukocytosis and disseminated intravascular coagulation. Empirical intravenous antibiotics including augmentin (amoxycillin and clavulanate), clindamycin and metornidazole were commenced in view of the clinical features of sepsis. Shortly after his stay in the intensive care unit, blisters (Figure 1) were discovered on both swollen lower limbs. Necrotizing fasciitis was suspected and ultimately confirmed with surgical exploration 12 h after the appearance of blisters. Initially, fasciotomy and excisional debridement were endeavored in an attempt to preserve the lower limbs. Meanwhile, high dose penicillin was introduced to replace augmentin. Nevertheless, the worsening clinical sepsis and migratory soft tissue necrosis inevitably resulted in bilateral above knee amputation. Microbiological cultures of blood and necrotic tissues invariably grew group G streptococcus only. Histological examination of the excised tissue also confirmed the diagnosis of necrotizing fasciitis. One day afterwards, similar features of skin changes developed over both upper limbs (Figure 2) that required repeated excisional debridements. In spite of limb amputation, surgical debridement and parenteral antibiotics, he developed fulminant group G streptococcal septicaemia and deteriorated rapidly until he succumbed to multi-organ failure six days after the onset of sepsis. Throughout his disease course, the perineum, groin and abdominal wall remained uninvolved.
Figure 1.
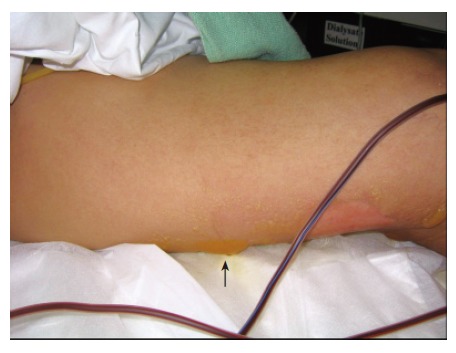
Enlarging blisters over the thigh. One of the blisters is indicated by black arrow.
Figure 2.

Necrotic skin patches over dorsum of hand.
DISCUSSION
In the English literature, there are only six reported cases of necrotizing fasciitis associated with colorectal malignancy (Table 1). In these cases, necrotizing fasciitis was all preceded by perforation of colorectal tumours. All except two cases[8,10-12] presented as Fournier's gangrene. One case manifested as psoas abscess with spreading infection to the thigh after retroperitoneal perforation of a sigmoid tumour[9]. The other one involved the anterior abdominal wall as a result of direct tumour invasion and perforation from the transverse colon[13]. In essence, perforated colorectal tumours represent an entry focus for bacterial translocation that might penetrate the subcutaneous soft tissues, leading to necrotizing infection[14]. To our knowledge, our patient is the first reported case of disseminated necrotizing fasciitis affecting all limbs in a non-perforated rectal tumour.
Table 1.
Literature review of necrotizing fasciitis associated with colorectal malignancy
| Authors | Yr published | Patient sex | Colorectal cancer type | Predisposing factors | Location of necrotizing fasciitis | Bacteria cultured | Outcome |
| Dewire et al[8] | 1992 | Male | Sigmoid | Bowel perforation | Fournier’s gangrene | E coli, Bacteroides fragilis, enterococci, anaerobes | Alive |
| Lam et al[9] | 1996 | Male | Sigmoid | Bowel perforation | Psoas abscess to upper thigh | E coli, Bacteroides fragilis, Edwardsiella tarda, staphylococcus, & Group G streptococci | Death |
| Gould et al[10] | 1997 | Male | Sigmoid | Bowel perforation | Fournier’s gangrene | Group F streptococci, anaerobes | Death |
| Lawrentschuk et al[11] | 2003 | Male | Rectum | Perforation with abscess | Fournier’s gangrene | E coli, Enterococcus, anaerobes & staphylococcus epidermidis | Alive |
| Gamagami et al[12] | 1998 | Male | Rectum | Perforation with abscess, Diabetes | Fournier’s gangrene | E coli, enterococci | Alive |
| Ku et al[13] | 2006 | Female | Transverse | Perforation with invasion to rectus fascia | Abdominal wall | Klebsiella pneumonia | Alive |
With regard to its etiology, we postulate three causes for such a fulminating disease in our patient. First, chronic subcutaneous tissue edema due to cirrhotic hypoalbuminaemia predispose him to subcutaneous tissue infection[6]. In addition, systemic immunosuppression could well be secondary to the cumulative effects of malignancy, diabetes mellitus and cirrhosis[7]. Lastly, transient bacteraemia might have arisen as a consequence of bacterial translocation emanated from occult necrosis of his rectal tumor[14]. Interestingly, there was a close temporal association between tumour biopsy and the onset of necrotizing sepsis in our patient. Transient bacteraemia following endoscopic tissue biopsy has been reported[15]. However, Gram negative organisms were the main bacteria retrieved and it was elusive to verify the causative association between rectal biopsy and necrotizing soft tissue infection in our patient.
So far as the bacteriological origin was concerned, group G streptococcus was the only culprit in our patient. In 1935, Lancefield, an American microbiologist, first described a Gram positive facultative anaerobic coccus as group G streptococcus that constitutes parts of the normal flora of human skin, respiratory tract and gastrointestinal tract[16-18]. Although it has been rarely implicated in necrotizing fasciitis[19], its associated mortality could be comparable to those induced by streptococcus pyogenes[20], suggesting that group G streptococcus, being a normal flora of the gastrointestinal tract, could represent a potentially life-threatening pathogen for all patients[20].
Regardless of the disparity in pathological and microbiological etiologies, the mortality rate of necrotizing fasciitis remains high. High index of suspicion and prompt surgical intervention are the cornerstone of treatment for improving the disease outcome[7]. We believe that delay in diagnosis and surgical treatment contributes to the demise of our patient.
Footnotes
S- Editor Wang J L- Editor Wang XL E- Editor Liu WF
References
- 1.Cunningham JD, Silver L, Rudikoff D. Necrotizing fasciitis: a plea for early diagnosis and treatment. Mt Sinai J Med. 2001;68:253–261. [PubMed] [Google Scholar]
- 2.Wong CH, Wang YS. The diagnosis of necrotizing fasciitis. Curr Opin Infect Dis. 2005;18:101–106. doi: 10.1097/01.qco.0000160896.74492.ea. [DOI] [PubMed] [Google Scholar]
- 3.Chelsom J, Halstensen A, Haga T, Høiby EA. Necrotising fasciitis due to group A streptococci in western Norway: incidence and clinical features. Lancet. 1994;344:1111–1115. doi: 10.1016/s0140-6736(94)90629-7. [DOI] [PubMed] [Google Scholar]
- 4.Jarrett P, Rademaker M, Duffill M. The clinical spectrum of necrotising fasciitis. A review of 15 cases. Aust N Z J Med. 1997;27:29–34. doi: 10.1111/j.1445-5994.1997.tb00910.x. [DOI] [PubMed] [Google Scholar]
- 5.Childers BJ, Potyondy LD, Nachreiner R, Rogers FR, Childers ER, Oberg KC, Hendricks DL, Hardesty RA. Necrotizing fasciitis: a fourteen-year retrospective study of 163 consecutive patients. Am Surg. 2002;68:109–116. [PubMed] [Google Scholar]
- 6.McHenry CR, Piotrowski JJ, Petrinic D, Malangoni MA. Determinants of mortality for necrotizing soft-tissue infections. Ann Surg. 1995;221:558–563; discussion 563-565. doi: 10.1097/00000658-199505000-00013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Francis KR, Lamaute HR, Davis JM, Pizzi WF. Implications of risk factors in necrotizing fasciitis. Am Surg. 1993;59:304–308. [PubMed] [Google Scholar]
- 8.Dewire DM, Bergstein JM. Carcinoma of the sigmoid colon: an unusual cause of Fournier's gangrene. J Urol. 1992;147:711–712. doi: 10.1016/s0022-5347(17)37363-9. [DOI] [PubMed] [Google Scholar]
- 9.Lam TP, Maffulli N, Chen EH, Cheng JC. Carcinomatous perforation of the sigmoid colon presenting as a thigh mass. Bull Hosp Jt Dis. 1996;55:83–85. [PubMed] [Google Scholar]
- 10.Gould SW, Banwell P, Glazer G. Perforated colonic carcinoma presenting as epididymo-orchitis and Fournier's gangrene. Eur J Surg Oncol. 1997;23:367–368. doi: 10.1016/s0748-7983(97)91020-9. [DOI] [PubMed] [Google Scholar]
- 11.Lawrentschuk N, Young AB, Nguyen H. Necrotizing fasciitis: an unusual presentation for rectal carcinoma. ANZ J Surg. 2003;73:865–867. doi: 10.1046/j.1445-2197.2003.02794.x. [DOI] [PubMed] [Google Scholar]
- 12.Gamagami RA, Mostafavi M, Gamagami A, Lazorthes F. Fournier's gangrene: an unusual presentation for rectal carcinoma. Am J Gastroenterol. 1998;93:657–658. doi: 10.1111/j.1572-0241.1998.189_b.x. [DOI] [PubMed] [Google Scholar]
- 13.Ku HW, Chang KJ, Chen TY, Hsu CW, Chen SC. Abdominal necrotizing fasciitis due to perforated colon cancer. J Emerg Med. 2006;30:95–96. doi: 10.1016/j.jemermed.2005.03.014. [DOI] [PubMed] [Google Scholar]
- 14.Panwalker AP. Unusual infections associated with colorectal cancer. Rev Infect Dis. 1988;10:347–364. doi: 10.1093/clinids/10.2.347. [DOI] [PubMed] [Google Scholar]
- 15.Lal D, Levitan R. Bacteremia following proctoscopic biopsy of a rectal polyp. Arch Intern Med. 1972;130:127–128. [PubMed] [Google Scholar]
- 16.Sylvetsky N, Raveh D, Schlesinger Y, Rudensky B, Yinnon AM. Bacteremia due to beta-hemolytic Streptococcus group G: increasing incidence and clinical characteristics of patients. Am J Med. 2002;112:622–626. doi: 10.1016/s0002-9343(02)01117-8. [DOI] [PubMed] [Google Scholar]
- 17.Tong SH, Tang WM, Wong JW. Group G streptococcus--a rare cause of osteomyelitis simulating bone tumour: a case report. J Orthop Surg (Hong Kong) 2003;11:221–223. doi: 10.1177/230949900301100221. [DOI] [PubMed] [Google Scholar]
- 18.Humar D, Datta V, Bast DJ, Beall B, De Azavedo JC, Nizet V. Streptolysin S and necrotising infections produced by group G streptococcus. Lancet. 2002;359:124–129. doi: 10.1016/S0140-6736(02)07371-3. [DOI] [PubMed] [Google Scholar]
- 19.Auckenthaler R, Hermans PE, Washington JA 2nd. Group G streptococcal bacteremia: clinical study and review of the literature. Rev Infect Dis. 1983;5:196–204. doi: 10.1093/clinids/5.2.196. [DOI] [PubMed] [Google Scholar]
- 20.Sharma M, Khatib R, Fakih M. Clinical characteristics of necrotizing fasciitis caused by group G Streptococcus: case report and review of the literature. Scand J Infect Dis. 2002;34:468–471. doi: 10.1080/003655402320170318. [DOI] [PubMed] [Google Scholar]