

Abstract
AIM: To investigate whether microvessel density (MVD) is related with prognosis in gastric cancer patients, and the expression of cyclooxygenase-2 (COX-2) and vessel endothelial growth factor (VEGF) so as to determine the possible role of COX-2 and VEGF in gastric cancer angiogenesis.
METHODS: Forty-seven formalin-fixed paraffin-embedded tissue samples of gastric cancer were evaluated for COX-2, VEGF by immunohistochemical staining. To assess tumor angiogenesis, MVD was determined by immunohistochemical staining of endothelial protein factor VIII-related antigen. The relationship among COX-2 and VEGF expression, MVD, and clinicopathologic parameters was analyzed.
RESULTS: Among the 67 samples, high MVD was significantly associated with lymph node metastasis and poor survival. Multivariate survival analysis showed that MVD value and lymph node metastasis were independent prognostic factors. The expression rate of COX-2 and VEGF was significantly higher than that of the adjacent tissues. COX-2 and VEGF expression in gastric cancer was significantly correlated with tumor differentiation and depth of invasion, but not with survival. The mean MVD value of COX-2 or VEGF positive tumors was higher than that of COX-2 or VEGF negative tumors. A significant correlation was found between the expressions of COX-2 and VEGF.
CONCLUSION: MVD may be one of the important prognostic factors for gastric cancer patients. COX-2 and VEGF may play an important role in tumor progression by stimulating angiogenesis. VEGF might play a main role in the COX-2 angiogenic pathway. The inhibition of angiogenesis or COX-2, VEGF activity may have an important therapeutic benefit in the control of gastric cancer.
Keywords: Gastric cancer, Angiogenesis, Microvessel density, Vessel endothelial growth factor, Cyclooxygenase, Prognostic marker, Nonsteroidal anti inflammatory drug
INTRODUCTION
Gastric cancer is one of the most frequent and lethal malignancies worldwide, especially in Eastern Asia including China, and the 5-year survival rate is only about 20%[1]. A recent research has shown an increasing trend of gastric cancer mortality in China in the past 20 years, especially in rural areas and among aged people[2]. To date, the treatment outcome of this common malignancy is still not satisfactory. One major difficulty in the diagnosis and treatment of gastric cancer is that only a few prognostic indicators can predict its clinical behavior. Recently, angiogenesis has been related to metastasis and poor prognosis in gastric cancer.
Angiogenesis, the process leading to the formation of new blood vessels, plays a central role in cancer cell survival, local tumor growth, and development of distant metastasis[3-5]. The degree of intratumoral microvessel density (MVD) by immunohistochemistry is thought to influence tumor metastasis and consequently prognosis in various human cancers, including gastric cancer[6-10]. The formation of tumor microvessels is dependent on the production of angiogenic growth factors by tumor cells. The formation of tumor microvessels is stimulated by angiogenic growth factors, including vessel endothelial growth factor (VEGF), platelet derived growth factor (PDGF), and transforming growth factor β1 (TGF-β1). The expression of these factors correlates with tumor angiogenesis, tumor progression and poor prognosis[11-13]. Among the known angiogenic factors, VEGF has emerged as the central regulator of the angiogenic process in cancer. The biological functions of VEGF include selective promotion of mitosis of endothelial cells, stimulation of their proliferation and angiogenesis, an increase in vessel transparency and extra-vasculization of large plasma molecules[14-17].
Cyclooxygenase (COX) is the rate-limiting enzyme in prostaglandin (PG) metabolism. COX has two isoforms: COX-1 and COX-2. COX-1 is constitutively expressed in most normal tissues and is thought to be involved in maintaining physiological function. COX-2 is frequently undetectable in normal tissue, but can be induced in response to growth factors, tumor promoters, hormones and cytokines, thus contributing to the synthesis of prostaglandin in inflamed and malignant tissues[18,19]. Over-expression of COX-2 is detectable in various solid malignancies including gastric cancer, and is thought to be involved in the critical steps in carcinogenesis, as well as a regulator of tumor angiogenesis[20-22]. However, the potential mechanism remains unclear.
To analyze the relationships between MVD, COX-2 and VEGF expression, clinicopathologic parameters and survival time of patients in gastric cancer, 67 specimens were evaluated for COX-2, VEGF and endothelial protein factor VIII-related antigen by immunohistochemical staining of MVD.
MATERIALS AND METHODS
Patients and specimens
Sixty-seven patients (54 men and 13 women, medium age 56 years) with gastric cancer undergone radical gastrectomy in the Department of Surgery, the First Affiliated Hospital of Anhui Medical University, from October 1997 to October 2000, were enrolled in this study. The eligibility criteria were: histologically proven gastric adenicarcinoma, no previous systemic chemotherapy or radiotherapy before operation, and well documented clinical data. The mean follow-up time was 34 mo (from 16 d to 60 mo).
All tissues were surgically resected. Cancerous tissue and para-cancerous gastric mucosa were all from the same specimens. Each specimen was fixed in 10% phosphate-buffered formalin immediately after resection, embedded in paraffin and cut into 4 μm-thick sections for immunohistochemical study and routine histological examination.
Immunohistochemistry
The sections were dewaxed and rehydrated by sequential immersion in xylene and graded ethanol and water. Endogenous peroxidase activity was blocked by incubation with 3% hydrogen peroxide methanol. Antigen-retrieval treatment was performed in a full pressure cooker for 10-15 min to obtain optimal results. After washed in phosphate-buffered saline (PBS) and exposed to 10% normal horse serum for 10 min to reduce non-specific binding, the sections were incubated with the primary antibody, which reacts specifically with VEGF (polyclonal, L2702, 1:50 dilution, overnight at 4°C; Santa Cruz Biotechnology, Inc.), COX-2 (polyclonal, J1602, 1:50 dilution, overnight at 4°C; Santa Cruz Biotechnology, Inc.), or factor VIII-related antigen (polyclonal, ZA-0111, overnight at 4°C; Santa Cruz Biotechnology, Inc.). All the sections were incubated with biotinylated IgG for 30 min and then with streptoavidin-peroxidase regent for 20 min. Finally, the sections were incubated in PBS containing diaminobenzidine and 1% hydrogen peroxide for 5 min, counterstained with Mayer hematoxylin, and mounted. PBS was substituted for primary antibody as the negative control.
Evaluation of immunostaining and microvessel counting
To evaluate COX-2 and VEGF expression, a score was established corresponding to the sum of a: percentage of positive cells (0 = 0% immunopositive cells, 1 = < 25% positive cells, 2 = 26%-50% positive cells, and 3 = > 50% positive cells), and b: staining intensity (0 = negative, 1 = weak, 2 = moderate, 3 = high). The sum of a + b reached a maximum score at 6. Scores between 0 and 2 were regarded as negative (-), between 3 and 4 as weak (+), and between 5 and 6 as strongly positive (++), respectively.
Intratumoral microvessels were highlighted by immunostaining with anti-factor VIII related antigen polyclonal antibody. Any single brownly stained cells or cluster of endothelial cells clearly separated from adjacent microvessels, tumor cells, and other connective tissue elements were considered as vessels. Branching structures were counted as a single vessel unless there was a discontinuity in the structure. The stained sections were screened at 100-magnification under a light microscope to identify the 5 regions of the section with the highest vascular density. Vessels were counted in the 5 regions at 200-magnification, and the average number of microvessels was recorded. Two observers did the counting, and the mean value was used for analysis.
Statistical analysis
Data were analyzed by SPSS version 10.0 for windows. The correlations between expression of COX-2, VEGF and clinic pathological parameters were assessed by the Chi-square test or the Spearman rank test. The Kaplan-Meier method was used to estimate survival as a function of time, and survival differences were analyzed by the log-rank test. The COX proportional hazard model was used for multivariate analysis of prognostic factors. P < 0.05 was considered statistically significant. All P values are represented as two-sided.
RESULTS
Correlation between MVD and clinicopathologic features
The MVD for 67 tumor specimens ranged from 14 to 58 with a mean MVD of 28.46 ± 8.28. When a mean MVD value of 28 was chosen as the cut-off point for discrimination of the 67 patients, 37 patients were categorized as low MVD and 30 as high MVD. The correlation between MVD and clinicopathologic features is shown in Table 1. High MVD was significantly associated with lymph node metastasis (P = 0.003).
Table 1.
Correlation between MVD, COX-2 and VEGF expression and clinicopathologic parameters of gastric cancer
| Clinicopathologic features | n |
MVD |
VEGF |
COX-2 |
||||||
| Low MVD (n = 37) | High MVD (n = 30) | P | - (n = 16) | +~++ (n = 51) | P | - (n = 16) | +~++ (n = 51) | P | ||
| Gender | 1.000 | 0.131 | 0.431 | |||||||
| Male | 54 | 30 | 24 | 15 | 39 | 14 | 40 | |||
| Female | 13 | 7 | 6 | 1 | 12 | 2 | 11 | |||
| Age (yr) | 1.000 | 0.820 | 0.820 | |||||||
| < 55 | 31 | 17 | 14 | 7 | 24 | 7 | 24 | |||
| ≥ 55 | 36 | 20 | 16 | 9 | 27 | 9 | 27 | |||
| Size of tumor (cm) | 0.227 | 0.636 | 0.218 | |||||||
| < 5 | 30 | 14 | 16 | 8 | 22 | 5 | 25 | |||
| ≥ 5 | 37 | 23 | 14 | 8 | 29 | 11 | 26 | |||
| Lymph node metastasis | 0.003 | 0.528 | 0.231 | |||||||
| Yes | 33 | 12 | 21 | 9 | 24 | 10 | 23 | |||
| No | 34 | 25 | 9 | 7 | 27 | 6 | 28 | |||
| Depth of invasion | 0.280 | 0.001 | 0.016 | |||||||
| Mucosa and submucosa | 9 | 3 | 6 | 6 | 3 | 5 | 4 | |||
| Muscularis propria | 58 | 34 | 24 | 10 | 48 | 11 | 47 | |||
| TNM stage | 0.280 | 0.342 | 0.342 | |||||||
| I and II | 58 | 34 | 24 | 15 | 43 | 15 | 43 | |||
| III and IV | 9 | 3 | 6 | 1 | 8 | 1 | 8 | |||
MVD: Microvessel density; VEGF: Vessel endothelial growth factor; COX-2: Cyclooxygenase-2; -: Negative; +~++: Positive to strong positive.
Multivariate survival analysis
Multivariate survival analysis showed that MVD value and lymph node metastasis were independent prognostic factors (Table 2). No other variables, including COX-2 and VEGF expression, were retained in the model or affected the magnitude of the hazard ratios of variables in the final model. Kaplan Meier curves for patients’ survival are shown in Figure 1. A significant difference in the overall survival rate was found between patients according to the MVD value (P < 0.001, comparison between low and high MVD).
Table 2.
Multivariate analysis of overall survival in gastric cancer
| Variable | Regression coefficient | Standard error (SE) | Odds ratio (95% CI) | P |
| Microvessel density (MVD) | 1.069 | 0.503 | 0.727-0.893 | 0.033 |
| Lymph node metastasis | 1.168 | 0.457 | 1.312-7.882 | 0.011 |
Figure 1.
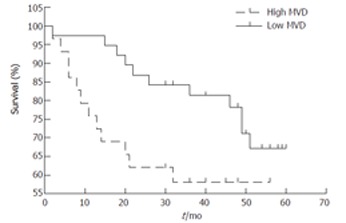
Kaplan-Meier survival curve correlating disease specific survival with high microvessel density (MVD) or low MVD.
Expression of COX-2 and VEGF in gastric cancer tissues
Immunoreactivity of both COX-2 and VEGF proteins was found in the tumor epithelial cells within cytoplasm (Figure 2). However, occasionally normal epithelial cells in adjacent tissues of cancer showed little staining. Among the 67 gastric cancer samples, the positive rates of COX-2 and VEGF expression were 76.1% and 76.1%, significantly higher than those in the adjacent tissues. The expression of VEGF protein in well-differentiated adenocarcinoma was significantly higher than that in poorly-differentiated adenocarcinoma (P < 0.05). There was a statistical difference in the expression of COX-2 protein among well-, moderately- and poorly-differentiated adenocarcinomas (P < 0.05).
Figure 2.
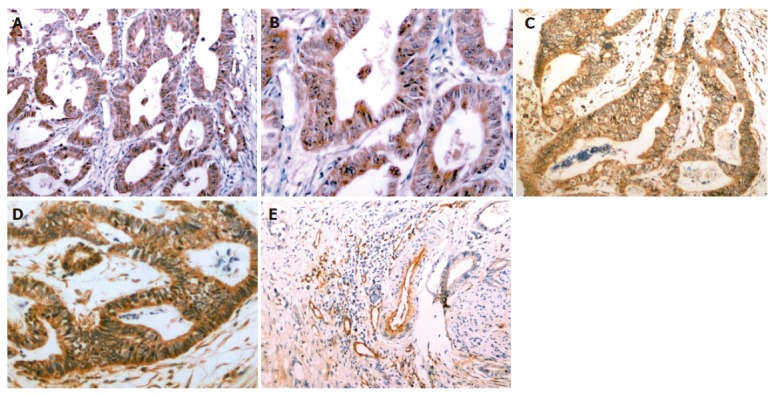
Immunohistochemical stainings of COX-2 (A, B), VEGF (C, D) and microvessels (E) in tissue sections obtained from gastric adenocarcinoma. COX-2 was mainly expressed in the cytoplasm of cancer cells (brown staining; A × 100, B × 200). VEGF expression was restricted to the cytoplasm of cancer cells (brown staining; C × 100, D × 200). Microvessels were detected in gastric cancer tissues by immunostaining for factor VIII-related antigen (E × 100).
Correlation between COX-2 or VEGF expression and MVD
The correlation between COX-2 or VEGF expression and MVD is summarized in Table 3. The mean MVD value of COX-2 or VEGF positive tumors was higher than that of COX-2 or VEGF negative tumors.
Table 3.
Relationship between expressions of VEGF, COX-2 and MVD of gastric cancer (mean ± SD)
| Group | n | MVD | P |
| VEGF | 0.008 | ||
| – | 16 | 20.14 ± 4.52 | |
| +~++ | 51 | 29.46 ± 8.28 | |
| COX-2 | 0.005 | ||
| – | 16 | 22.32 ± 3.80 | |
| +~++ | 51 | 29.88 ± 8.52 |
VEGF: Vessel endothelial growth factor; COX-2: Cyclooxygenase-2; MVD: Microvessel density; -: Negative; +~++: Positive to strong positive.
Association between COX-2 and VEGF expression
A significant correlation was found between the expression levels of COX-2 and VEGF (Table 4, r = 0.425, P < 0.001).
Table 4.
Relationship between VEGF and COX-2 expression in gastric cancer
| VEGF |
COX-2 |
r | P | |
| – | +~++ | |||
| – | 9 | 7 | 0.425 | < 0.001 |
| +~++ | 7 | 44 | ||
VEGF: Vessel endothelial growth factor; COX-2: Cyclooxygenase-2; -: Negative; +~++: Positive to strong positive.
Correlations of COX-2, VEGF expression with clinicopathologic parameters
The associations between COX-2 and VEGF expressions and the clinicopathologic parameters are shown in Table 1. The expression of both proteins in gastric cancer was significantly correlated with depth of invasion. There was no significant association between COX-2 and VEGF expression and patient gender, age, tumor size, lymph node metastasis, and TNM stage.
DISCUSSION
Folkman J and Shing Y[3] initiated a new field of research about tumor angiogenesis in 1971 and found that several factors take part in the process of angiogenesis. Tumor angiogenesis is now believed to be one of the most crucial steps in tumor growth and metastases[3-5]. Moreover, tumor angiogenesis which can be quantified by measurement of MVD is a significant negative prognostic factor[6-10]. In our study, when a mean MVD value was chosen as the cut-off point for discrimination of the study patients, high MVD was significantly associated with lymph node metastasis and poor survival. Multivariate survival analysis showed that MVD value and lymph node metastasis were independent prognostic factors for gastric cancer patients.
Tumor angiogenesis is controlled by a balance between angiogenic and angiostatic regulators involved in multiple pathways that result in endothelial proliferation, differentiation and organization into a functional network of vascular channels[3-5]. Among the reported angiogenic factors[11-14], VEGF (a key factor for induction of tumor angiogenesis) is increased in various human tumors, often correlating with higher MVD[15-17]. In our study, VEGF was over-expressed in gastric cancer tissues. We found that VEGF expression was associated with the histologic types of gastric cancer and depth of invasion. The results suggest that VEGF might be mainly involved in the progression of gastric carcinoma. The mean MVD value of VEGF positive tumors was significantly higher than that of VEGF negative tumors, suggesting that VEGF may facilitate tumor progression by promoting tumor angiogenesis.
Epidemiologic studies indicate that use of aspirin and other non-steroidal anti inflammatory drugs (NSAIDs), with COX being their major target, decreases the incidence and mortality of colorectal, gastric, and esophageal cancers[23-26]. The expression of COX-2 mRNA and protein is elevated in various human malignancies, which may play a critical role in the development of cancer[27-30]. Our study showed that the positive rate of COX-2 expression in human gastric cancers was significantly higher than that in the matched normal gastric tissue. COX-2 expression was associated with the degree of tumor cell differentiation and depth of invasion, but not with survival. These results suggest that over-expression of COX-2 plays an important role in the development of human gastric cancer, but cannot predicate the outcome in individual cases.
The contributions of COX-2 to tumor angiogenesis include: increasing expression of VEGF, producing of prostaglandin E (PGE) 2 and prostaglandin I (PGI) 2 that can directly stimulate endothelial cell migration and growth factor-induced angiogenesis, and inhibiting endothelial cell apoptosis by stimulation of Bcl-2 or Akt activation[31,32]. In our present study, COX-2 expression was significantly associated with that of VEGF. The mean MVD value of COX-2 or VEGF positive tumors was higher than that of COX-2 or VEGF negative tumors, which is in agreement with previous reports[33,34]. These data strongly suggest that COX-2 and VEGF may be partly responsible for the important process of angiogenesis in the development of human gastric cancer, and VEGF plays the main role in COX-2 stimulated angiogenesis. However, there still exist some other pathways, which also participate in COX-2-induced angiogenesis.
In conclusion, high MVD is significantly associated with lymph node metastasis and poor survival. MVD value and lymph node metastasis are independent prognostic factors for gastric cancer patients. Expression of COX-2 and VEGF is closely correlated to the depth of invasion, and leads to increased angiogenesis, which may be the mechanisms underlying the contribution of COX-2 to the development of gastric cancer. VEGF might play a main role in the COX-2 angiogenic pathway. Inhibition of angiogenesis or COX-2, VEGF activity may have an important therapeutic benefit in the control of gastric cancer.
COMMENTS
Background
Gastric cancer is one of the most frequent and lethal malignancies worldwide, especially in Eastern Asia including China, and the 5-year survival rate is only about 20%. To date, the treatment outcome of this common malignancy is still not satisfactory. One major difficulty in the diagnosis and treatment of gastric cancer is that only a few prognostic indicators can predict its clinical behavior.
Research frontiers
Tumor angiogenesis plays a central role in cancer cell survival, local tumor growth, and development of distant metastasis, which can be assessed by the MVD. The degree of intratumoral MVD is thought to influence tumor metastasis and consequently prognosis in various human cancers, including gastric cancer. Additionally, tumor MVD is associated with COX-2 and VEGF expression.
Applications
The present work suggests that high MVD is significantly associated with lymph node metastasis and poor survival. MVD value and lymph node metastasis are two independent prognostic factors for gastric cancer patients. Expression of COX-2 and VEGF is closely correlated to the depth of invasion, and leads to increased angiogenesis, which may be the mechanisms underlying the development of gastric cancer. VEGF might play a main role in the COX-2 angiogenic pathway. Inhibition of angiogenesis or COX-2, VEGF activity may have an important therapeutic benefit in the control of gastric cancer.
Peer review
This is a well-written and carefully performed study. The title, results and discussion are clear. The abstract and introduction are well-organized.
Footnotes
Supported by the Major State Basic Research Development Program (973 Program) of China (No. 2003CB515507) and Science and Technology Fund by Department of Education of Anhui Province
S- Editor Wang GP L- Editor Wang XL E- Editor Bi L
References
- 1.Stadtländer CT, Waterbor JW. Molecular epidemiology, pathogenesis and prevention of gastric cancer. Carcinogenesis. 1999;20:2195–2208. doi: 10.1093/carcin/20.12.2195. [DOI] [PubMed] [Google Scholar]
- 2.Yang L, Parkin DM, Li LD, Chen YD, Bray F. Estimation and projection of the national profile of cancer mortality in China: 1991-2005. Br J Cancer. 2004;90:2157–2166. doi: 10.1038/sj.bjc.6601813. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Folkman J, Shing Y. Angiogenesis. J Biol Chem. 1992;267:10931–10934. [PubMed] [Google Scholar]
- 4.Risau W. Mechanisms of angiogenesis. Nature. 1997;386:671–674. doi: 10.1038/386671a0. [DOI] [PubMed] [Google Scholar]
- 5.Folkman J. Seminars in Medicine of the Beth Israel Hospital, Boston. Clinical applications of research on angiogenesis. N Engl J Med. 1995;333:1757–1763. doi: 10.1056/NEJM199512283332608. [DOI] [PubMed] [Google Scholar]
- 6.Tsutsui S, Kume M, Era S. Prognostic value of microvessel density in invasive ductal carcinoma of the breast. Breast Cancer. 2003;10:312–319. doi: 10.1007/BF02967651. [DOI] [PubMed] [Google Scholar]
- 7.Lackner C, Jukic Z, Tsybrovskyy O, Jatzko G, Wette V, Hoefler G, Klimpfinger M, Denk H, Zatloukal K. Prognostic relevance of tumour-associated macrophages and von Willebrand factor-positive microvessels in colorectal cancer. Virchows Arch. 2004;445:160–167. doi: 10.1007/s00428-004-1051-z. [DOI] [PubMed] [Google Scholar]
- 8.Raspollini MR, Amunni G, Villanucci A, Baroni G, Boddi V, Taddei GL. Prognostic significance of microvessel density and vascular endothelial growth factor expression in advanced ovarian serous carcinoma. Int J Gynecol Cancer. 2004;14:815–823. doi: 10.1111/j.1048-891X.2004.014514.x. [DOI] [PubMed] [Google Scholar]
- 9.Bremnes RM, Camps C, Sirera R. Angiogenesis in non-small cell lung cancer: the prognostic impact of neoangiogenesis and the cytokines VEGF and bFGF in tumours and blood. Lung Cancer. 2006;51:143–158. doi: 10.1016/j.lungcan.2005.09.005. [DOI] [PubMed] [Google Scholar]
- 10.Tanigawa N, Amaya H, Matsumura M, Shimomatsuya T, Horiuchi T, Muraoka R, Iki M. Extent of tumor vascularization correlates with prognosis and hematogenous metastasis in gastric carcinomas. Cancer Res. 1996;56:2671–2676. [PubMed] [Google Scholar]
- 11.Affara NI, Robertson FM. Vascular endothelial growth factor as a survival factor in tumor-associated angiogenesis. In Vivo. 2004;18:525–542. [PubMed] [Google Scholar]
- 12.Ferrara N, Gerber HP. The role of vascular endothelial growth factor in angiogenesis. Acta Haematol. 2001;106:148–156. doi: 10.1159/000046610. [DOI] [PubMed] [Google Scholar]
- 13.Tanigawa N, Amaya H, Matsumura M, Shimomatsuya T. Correlation between expression of vascular endothelial growth factor and tumor vascularity, and patient outcome in human gastric carcinoma. J Clin Oncol. 1997;15:826–832. doi: 10.1200/JCO.1997.15.2.826. [DOI] [PubMed] [Google Scholar]
- 14.Ferrara N, Gerber HP, LeCouter J. The biology of VEGF and its receptors. Nat Med. 2003;9:669–676. doi: 10.1038/nm0603-669. [DOI] [PubMed] [Google Scholar]
- 15.Ferrara N, Heinsohn H, Walder CE, Bunting S, Thomas GR. The regulation of blood vessel growth by vascular endothelial growth factor. Ann N Y Acad Sci. 1995;752:246–256. doi: 10.1111/j.1749-6632.1995.tb17435.x. [DOI] [PubMed] [Google Scholar]
- 16.Kolch W, Martiny-Baron G, Kieser A, Marmé D. Regulation of the expression of the VEGF/VPS and its receptors: role in tumor angiogenesis. Breast Cancer Res Treat. 1995;36:139–155. doi: 10.1007/BF00666036. [DOI] [PubMed] [Google Scholar]
- 17.Leung DW, Cachianes G, Kuang WJ, Goeddel DV, Ferrara N. Vascular endothelial growth factor is a secreted angiogenic mitogen. Science. 1989;246:1306–1309. doi: 10.1126/science.2479986. [DOI] [PubMed] [Google Scholar]
- 18.Dubois RN, Abramson SB, Crofford L, Gupta RA, Simon LS, Van De Putte LB, Lipsky PE. Cyclooxygenase in biology and disease. FASEB J. 1998;12:1063–1073. [PubMed] [Google Scholar]
- 19.Williams CS, Mann M, DuBois RN. The role of cyclooxygenases in inflammation, cancer, and development. Oncogene. 1999;18:7908–7916. doi: 10.1038/sj.onc.1203286. [DOI] [PubMed] [Google Scholar]
- 20.Zha S, Yegnasubramanian V, Nelson WG, Isaacs WB, De Marzo AM. Cyclooxygenases in cancer: progress and perspective. Cancer Lett. 2004;215:1–20. doi: 10.1016/j.canlet.2004.06.014. [DOI] [PubMed] [Google Scholar]
- 21.Koga T, Shibahara K, Kabashima A, Sumiyoshi Y, Kimura Y, Takahashi I, Kakeji Y, Maehara Y. Overexpression of cyclooxygenase-2 and tumor angiogenesis in human gastric cancer. Hepatogastroenterology. 2004;51:1626–1630. [PubMed] [Google Scholar]
- 22.Walther Z. COX-2 and angiogenesis in gastric cancer. J Clin Gastroenterol. 2003;37:4–6. doi: 10.1097/00004836-200307000-00003. [DOI] [PubMed] [Google Scholar]
- 23.Chan AT, Giovannucci EL, Meyerhardt JA, Schernhammer ES, Curhan GC, Fuchs CS. Long-term use of aspirin and nonsteroidal anti-inflammatory drugs and risk of colorectal cancer. JAMA. 2005;294:914–923. doi: 10.1001/jama.294.8.914. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Hur C, Simon LS, Gazelle GS. The cost-effectiveness of aspirin versus cyclooxygenase-2-selective inhibitors for colorectal carcinoma chemoprevention in healthy individuals. Cancer. 2004;101:189–197. doi: 10.1002/cncr.20329. [DOI] [PubMed] [Google Scholar]
- 25.Jolly K, Cheng KK, Langman MJ. NSAIDs and gastrointestinal cancer prevention. Drugs. 2002;62:945–956. doi: 10.2165/00003495-200262060-00006. [DOI] [PubMed] [Google Scholar]
- 26.Farrow DC, Vaughan TL, Hansten PD, Stanford JL, Risch HA, Gammon MD, Chow WH, Dubrow R, Ahsan H, Mayne ST, et al. Use of aspirin and other nonsteroidal anti-inflammatory drugs and risk of esophageal and gastric cancer. Cancer Epidemiol Biomarkers Prev. 1998;7:97–102. [PubMed] [Google Scholar]
- 27.Soumaoro LT, Uetake H, Higuchi T, Takagi Y, Enomoto M, Sugihara K. Cyclooxygenase-2 expression: a significant prognostic indicator for patients with colorectal cancer. Clin Cancer Res. 2004;10:8465–8471. doi: 10.1158/1078-0432.CCR-04-0653. [DOI] [PubMed] [Google Scholar]
- 28.Wolff H, Saukkonen K, Anttila S, Karjalainen A, Vainio H, Ristimäki A. Expression of cyclooxygenase-2 in human lung carcinoma. Cancer Res. 1998;58:4997–5001. [PubMed] [Google Scholar]
- 29.Buskens CJ, Van Rees BP, Sivula A, Reitsma JB, Haglund C, Bosma PJ, Offerhaus GJ, Van Lanschot JJ, Ristimäki A. Prognostic significance of elevated cyclooxygenase 2 expression in patients with adenocarcinoma of the esophagus. Gastroenterology. 2002;122:1800–1807. doi: 10.1053/gast.2002.33580. [DOI] [PubMed] [Google Scholar]
- 30.Ristimäki A, Sivula A, Lundin J, Lundin M, Salminen T, Haglund C, Joensuu H, Isola J. Prognostic significance of elevated cyclooxygenase-2 expression in breast cancer. Cancer Res. 2002;62:632–635. [PubMed] [Google Scholar]
- 31.Gately S. The contributions of cyclooxygenase-2 to tumor angiogenesis. Cancer Metastasis Rev. 2000;19:19–27. doi: 10.1023/a:1026575610124. [DOI] [PubMed] [Google Scholar]
- 32.Saukkonen K, Rintahaka J, Sivula A, Buskens CJ, Van Rees BP, Rio MC, Haglund C, Van Lanschot JJ, Offerhaus GJ, Ristimaki A. Cyclooxygenase-2 and gastric carcinogenesis. APMIS. 2003;111:915–925. doi: 10.1034/j.1600-0463.2003.1111001.x. [DOI] [PubMed] [Google Scholar]
- 33.Uefuji K, Ichikura T, Mochizuki H. Cyclooxygenase-2 expression is related to prostaglandin biosynthesis and angiogenesis in human gastric cancer. Clin Cancer Res. 2000;6:135–138. [PubMed] [Google Scholar]
- 34.Joo YE, Rew JS, Seo YH, Choi SK, Kim YJ, Park CS, Kim SJ. Cyclooxygenase-2 overexpression correlates with vascular endothelial growth factor expression and tumor angiogenesis in gastric cancer. J Clin Gastroenterol. 2003;37:28–33. doi: 10.1097/00004836-200307000-00009. [DOI] [PubMed] [Google Scholar]