

Abstract
Currently, laparoscopic cholecystectomy is an undoubtfully optimal treatment of cholelithiasis. What about performing this procedure on a patient with situs inversus totalis and what are the difficulties of this operation for a right-handed surgeon We presented a 35-year-old man with unknown situs inversus totalis who was admitted with epigastric pain and digestive problems. Ultrasonography and computed tomography of the abdomen confirmed the diagnosis of a gallstone. Besides, the liver and gallbladder were on the left side and the spleen was on the right. All systems were left-right reversal as mirror image in all diagnostic studies. Laparoscopic cholecystectomy was safely performed, despite of difficulties of situs inversus. The patient was discharged on postoperative day 1. It should be considered that existence of other anomalies may easily cause uninvited injuries. In the patients with situs inversus, laparoscopic cholecystectomy can be safely managed by an experienced surgeon through laparoscopy, and also hepatobiliary surgery.
Keywords: Situs inversus totalis, Laparoscopic chole-cystectomy, Cholelithiasis
INTRODUCTION
Situs inversus totalis (SIT) is a very uncommon entity. It was first reported by Fabricius in 1600[1]. The incidence is thought to be in the range of 1:10 000 to 1:20 000[2]. Transposition of the organs may also affect thoracic organs, besides abdominal organs. It can be associated with Kartegener triad or some other cardiac anomalies. There is no evidence for increased incidence of choleli-thiasis in SIT[3]. Since Mouret first performed it in 1987, laparoscopic cholecystectomy (LC) has become the standard operative procedure for cholelithiasis[4].
In the present study, the new technique and sub-sequently possible difficulties of LC in a patient with SIT was reported.
CASE REPORT
A 35-year-old male was admitted to the Department of General Surgery, Ege University School of Medicine, with a 2-year history of intermittent epigastric pain and concomitant digestive problems. The patient had not been diagnosed as situs inversus totalis before. Apex beat was found in the right hemithorax on physical examination. An electrocardiography showed right axis deviation and right ventricular hypertrophy, in keeping with dextrocardia. Laboratory data showed no abnormality of liver function tests, or white blood cell count. An ultrasonography identified SIT and multiple stones, which were millimetric in size in the gallbladder. The common bile duct was also noted as dilated. A thoracoabdominal computed tomography (CT) revealed the situs inversus totalis abnormality and a suspicious opacity located at the neck of the gallbladder (Figure 1). Endoscopic retrograde cholangiopancreatography was performed and a stone was extracted from the common bile duct (Figure 2). The patient then underwent LC.
Figure 1.
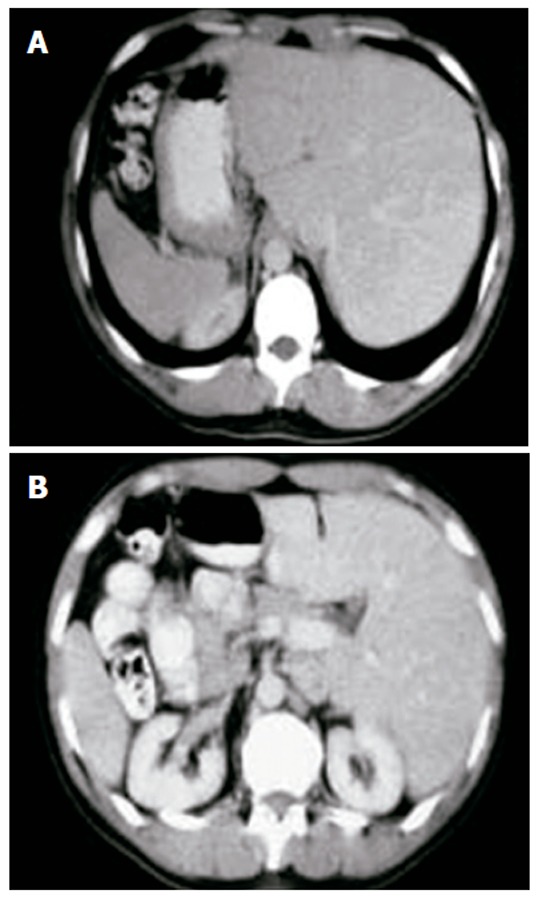
Computed tomography of the patient. A: The liver is on the left side; B: The spleen and stomach are on the right side of the patient.
Figure 2.
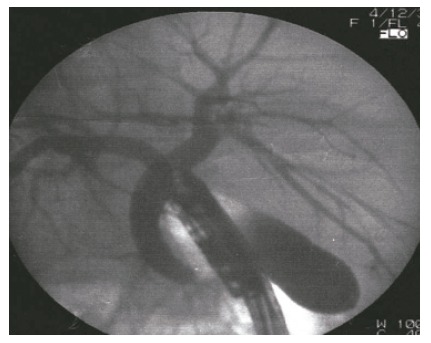
Endoscopic retrograde cholangiography of the patient. A stone was extracted from the main duct. The gallbladder can be observed on the left side.
Operation techniques
The operation team and the laparoscopic devices were located in the theater as a mirror image configuration of normal LC. Dissection of the Calot’s triangle is one of the major problems for a right-handed surgeon in case of situs inversus totalis abnormality. Four ports were used: optical (10 mm), one 5 mm and one 10 mm operating, and one 5 mm assisting port (Figure 3). The optical port was near the umbilicus and a 30° laparoscope was used. Because of previously unoperated abdomen, the closed technique was employed by the insertion of a Veress needle through the subumbilical area. Carbon dioxide (CO2) pneumoperitoneum was then created with a pressure of 12 mmHg. Two 10-mm trocars were inserted into the abdominal cavity, one in the position of the Veress needle for laparoscope and the other one in the sub-xiphoid location. A 5-mm trocar was inserted midline at the midpoint of xiphoid-umbilicus line and a second 5-mm trocar was inserted into the abdominal cavity in the left mid-axillary line under the view of laparoscope. Fundus of the gallbladder was grasped and retracted by the assistant using a clinch, which was inserted through the 5-mm trocar in the left mid-axillary region. Traction of the Hartmann’s pouch was performed by the left hand of the surgeon using a grasper inserted through the trocar located at the subxiphoid region. Dissection of Calot’s triangle was carried out with a posterior approach by using a forceps that was inserted through the trocar located in the midline. The cystic duct and cystic artery were first divided by blunt dissection and separated. Dissection was performed above the plane of Rouviere’s sulcus to avoid any injury. Both of them were clipped (double proximal, single distal 10-mm titanium clips) and then divided by hook scissors. After division of all peritoneal reflection on either side, the gallbladder was retrogradely separated from the liver bed by using electrocautery. It was then extracted through the 10-mm operating port. Fascial closure of large ports was sutured with absorbable material (polydiaxonon) to prevent herniation.
Figure 3.
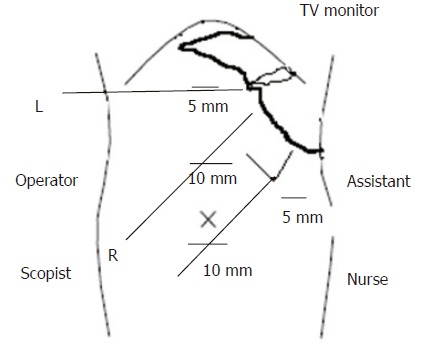
Port sites in new technique. L: left hand; R: right hand.
DISCUSSION
Situs inversus viscerum is considered to have a genetic predisposition that is autosomal recessive[5,6] and may be associated with several syndromes[7,8]. Physical examination of the patient with situs inversus can be misleading. As the central nervous system may not share the general transposition, pain may be felt in the epigastrium alone or in the right-upper quadrant and in the mid-scapular region[9-11]. In patients of acute cholecystitis with situs inversus, pain can be felt in the left upper quadrant due to irritation of the peritoneum[11,12]. Intrahepatic biliary tree, arterial and venous systems are in the mirror-image configuration of the normal anatomy. The hepatoduodenal ligament is the same as seen in the orthotopic patient[13]. Arterial system anomalies are in the mirror-image configuration of the orthotopic patients[14]. Although there are many reports of patients with situs inversus and cholelithiasis, there is no evidence that the incidence of cholelithiasis is greater in these patients[15]. In the preoperative period CT may be useful in determining the anomalies[12]. Twenty cases of LC in SIT were reported in the literature[16]. The most challenging factor for performing LC in patients with situs inversus is the mirror image anatomy. This uninvited condition may lead to some problems in orientation and dissection during the procedure since at least two thirds of the surgeons are right handed[16]. To overcome this issue, several alternative modifications were proposed: (1) retraction of Hartmann pouch by the first assistant, (2) surgeon standing between the two abducted lower limbs of the patient[1,16].
We propose that it helps by changing the position of grasper with the dissector and dissecting the Calot‘s triangle from the lateral side, taking advantage of using the right hand. To use the midclavicular trocar in dissection, which is used only for traction in traditional technique, the view angle should be increased and crossing of the scope and dissector should be prevented. To achieve this, the midclavicular 5 mm trocar is placed at the midline and a 30º viewing scope is used via the subumbilical trocar. By using this technique, an extra 45º is added to the 30º viewing of the scope. Careful dissection of Calot’s triangle can be managed by performing it from the lateral side with the help of this totally 75º. Working in two dimensions is the biggest difficulty in laparoscopic surgery. In addition to this, mirror-image that is seen in situs inversus increases the difficulty. As a result, this may lead to high risk of iatrogenic injuries. In those cases as Thomas B Hugh mentioned in his article; in traditional cholecystectomy technique, the start point is fundus of the gallbladder but this is not convenient for laparoscopic method[16]. In laparoscopic cholecystectomy, the sulcus, which is called Rouviere’s sulcus that runs to the right of the hilum of the liver can be an alternative reference point. This sulcus is open in 78% of patients and its site is recognizable in more than 90% of the patients[16]. Dissection should be safely carried out close to the gallbladder in the triangle that is described in this article. Reviewing the operative field regularly and releasing the traction of the gallbladder may help you know where you are. Withdrawing the camera will help to obtain a large field of view. With the help of these, overall relationship in the hepatobiliary triangle can be evaluated. The findings during the operation should be checked with other members of the operating team. Care must be taken for the concentration of the operative team and arrangement of the equipment setup in the operation room.
In conclusion, we suggest that LC procedure in these patients with SIT should be performed by surgeons who are experienced in laparoscopy and hepatobiliary surgery as well.
Footnotes
S- Editor Wang J L- Editor Zhu LH E- Editor Ma WH
References
- 1.Yaghan RJ, Gharaibeh KI, Hammori S. Feasibility of laparoscopic cholecystectomy in situs inversus. J Laparoendosc Adv Surg Tech A. 2001;11:233–237. doi: 10.1089/109264201750539763. [DOI] [PubMed] [Google Scholar]
- 2.Al-Jumaily M, Hoche F. Laparoscopic cholecystectomy in situs inversus totalis: is it safe. J Laparoendosc Adv Surg Tech A. 2001;11:229–231. doi: 10.1089/109264201750539754. [DOI] [PubMed] [Google Scholar]
- 3.Crosher RF, Harnarayan P, Bremner DN. Laparoscopic cholecystectomy in situs inversus totalis. J R Coll Surg Edinb. 1996;41:183–184. [PubMed] [Google Scholar]
- 4.Jaffray B. Minimally invasive surgery. Arch Dis Child. 2005;90:537–542. doi: 10.1136/adc.2004.062760. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.D'Agata A, Boncompagni G. [Video laparoscopic cholecystectomy in situ viscerum inversus totalis] Minerva Chir. 1997;52:271–275. [PubMed] [Google Scholar]
- 6.Demetriades H, Botsios D, Dervenis C, Evagelou J, Agelopoulos S, Dadoukis J. Laparoscopic cholecystectomy in two patients with symptomatic cholelithiasis and situs inversus totalis. Dig Surg. 1999;16:519–521. doi: 10.1159/000018780. [DOI] [PubMed] [Google Scholar]
- 7.VARANO NR, MERKLIN RJ. Situs inversus: review of the literature, report of four cases and analysis of the clinical implications. J Int Coll Surg. 1960;33:131–148. [PubMed] [Google Scholar]
- 8.Schiffino L, Mouro J, Levard H, Dubois F. [Cholecystectomy via laparoscopy in situs inversus totalis. A case report and review of the literature] Minerva Chir. 1993;48:1019–1023. [PubMed] [Google Scholar]
- 9.Southam JA. Left-sided gallbladder: : calculous cholecystitis with situs inversus. Ann Surg. 1975;182:135–137. doi: 10.1097/00000658-197508000-00009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Heimann T, Sicular A. Acute cholecystitis with situs inversus. N Y State J Med. 1979;79:253–254. [PubMed] [Google Scholar]
- 11.Drover JW, Nguyen KT, Pace RF. Laparoscopic cholecystectomy in a patient with situs inversus viscerum: a case report. Can J Surg. 1992;35:65–66. [PubMed] [Google Scholar]
- 12.Goh P, Tekant Y, Shang NS, Ngoi SS. Laparoscopic cholecystectomy in a patient with empyema of the gallbladder and situs inversus. Endoscopy. 1992;24:799–800. doi: 10.1055/s-2007-1010589. [DOI] [PubMed] [Google Scholar]
- 13.McDermott JP, Caushaj PF. ERCP and laparoscopic cholecystectomy for cholangitis in a 66-year-old male with situs inversus. Surg Endosc. 1994;8:1227–1229. doi: 10.1007/BF00591057. [DOI] [PubMed] [Google Scholar]
- 14.Kamitani S, Tsutamoto Y, Hanasawa K, Tani T. Laparoscopic cholecystectomy in situs inversus totalis with "inferior" cystic artery: a case report. World J Gastroenterol. 2005;11:5232–5234. doi: 10.3748/wjg.v11.i33.5232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.McKay D, Blake G. Laparoscopic cholecystectomy in situs inversus totalis: a case report. BMC Surg. 2005;5:5. doi: 10.1186/1471-2482-5-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hugh TB. New strategies to prevent laparoscopic bile duct injury--surgeons can learn from pilots. Surgery. 2002;132:826–835. doi: 10.1067/msy.2002.127681. [DOI] [PubMed] [Google Scholar]