

Abstract
Prompt treatment in tumor-associated encephalopathy may prolong survival. We describe a 69-year-old male patient who was presented with fulminant hepatic failure, secondary to small-cell lung carcinoma with rapidly progressing encephalopathy. Both symptoms remitted following chemotherapy, suggesting swift diagnosis and administration of chemotherapy to be effective in treatment of fulminant hepatic failure and encephalopathy.
Keywords: Small-cell lung carcinoma, Fulminant hepatic failure, Chemotherapy
INTRODUCTION
Fulminant hepatic failure (FHF) is defined as a liver failure with encephalopathy, developing within eight weeks from the onset symptoms in the absence of pre-existing liver disease. The most common causes of FHF are viral or drug-induced hepatitis[1]. Small-cell lung cancer (SCLC) manifesting as acute hepatic failure resulting from diffuse parenchymal infiltration by metastatic tumor is rare. The prognosis is poor, with death usually occurring within several days[1]. We describe herein a patient with SCLC and FHF that improved after chemotherapy.
CASE REPORT
A 69-year-old male was admitted to our hospital because of a 2-wk history of nausea, anorexia, fatigue, jaundice, and pain in the right upper quadrant of the abdomen. He had no history of blood transfusion, hepatitis, intravenous drug use, or alcohol abuse, though had an average of 2 packs of cigarettes a day for 50 years. Physical examination revealed hepatomegaly and bilateral pretibial edema, but he was alert. Laboratory analyses revealed 1760 U/L alkaline phosphatase, 6695 U/L lactate dehydrogenase (LDH), 470 U/L aspartate aminotransferase (AST), 7.6 mg/dL bilirubin, 85 μg/dL ammonia, prothrombin time level of 63%, and 680 ng/mL neuron specific enolase (NSE) levels. A computed tomography (CT) of the abdomen showed multiple lesions and massive infiltration throughout the liver parenchyma (Figure 1A). A chest roentgenogram and CT scan showed a right hilar mass with pleural effusion (Figure 1B). Bronchoscopy with transbronchial lung biopsy revealed small-cell carcinoma of the lung (Figure 2). On the seventh day of hospitalization, chemotherapy was initiated with carboplatin (area under the curve 4) administered on d 1, and 80 mg/m2 etoposide from d 1 to 3, with cycles repeated every 3 wk.
Figure 1.
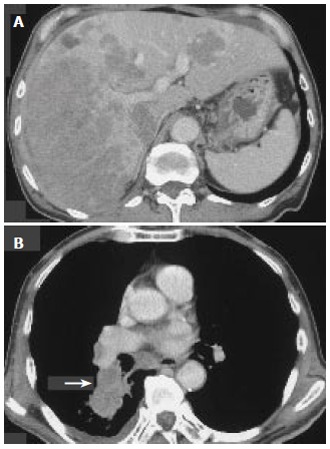
Computed tomography of the patient. A: CT of the abdomen showing multiple lesions and massively infiltrative process throughout the liver parenchyma; B: CT of the chest showing a right hilar mass (arrow) with pleural effusion.
Figure 2.
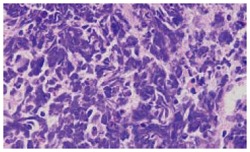
Histological examination of transbronchial lung biopsy specimen showing extensive infiltration small-cell carcinoma.
After two cycles of chemotherapy, the patient felt symptomatically better, and a CT of the chest and abdomen revealed a marked reduction of tumor size in the primary site and liver metastasis. The laboratory analyses revealed an improvement of hepatic failure. During the 2 months of initial chemotherapy, the patient’s condition deteriorated due to progression of hepatic failure (total bilirubin level, 19.5 mg/dL; LDH, 4 699 U/L; AST, 424 U/L; ammonia, 145 μg/dL; glucose, 129 mg/dL; prothrombin time, 38%), the development of ascites, and stage II encephalopathy. A CT scan of the brain revealed no evidence of cerebral metastatic disease. However, the radiological examination revealed the recurrence of SCLC. Therefore, the patient was treated with 35 mg/m2 amrubicin from d 1 to 3, with cycles repeated every 3 wk. Though grade 4 neutropenia (NCI-CTC ver 2.0) occurred after two cycles of chemotherapy, the patient had a marked improvement of encephalopathy (stage 0), general condition, and laboratory values (LDH, 180 U/L; AST, 45 U/L; ammonia, 42 μg/dL; prothrombin time 89%; and NSE, 9.6 ng/mL). Follow-up CT imaging documented a good partial response of the liver metastases, and a complete disappearance of the right hilar mass. Then, he was discharged from our hospital. However, the patient died of bacterial pneumonia at six months after presentation. A post-mortem was not done because of refusal of his family.
DISCUSSION
FHF secondary to metastatic SCLC is rare and results in death within days to weeks[1-3]. In literature, there are 21 previously reported cases of acute hepatic failure resulting from metastatic SCLC (Table 1). Two of the 21 reported patients presented an apparent dramatic response of severe tumor-related lactic acidosis to the initiation of chemotherapy (cyclophosphamide, doxorubicin, and vincristine)[3,4]. In most of the reported patients, however, the administration of appropriate chemotherapy was not performed, and no diagnosis was made before death. The rapid deterioration of the patient’s condition may account for the difficulty of an accurate diagnosis[1]. The seven patients of acute hepatic failure with encephalopathy, even if metastatic SCLC was diagnosed before death, all died without the administration of chemotherapy because of a rapidly deteriorating course[1,5-8].
Table 1.
Summary of 21 previously reported cases of acute hepatic failure due to metastatic small-cell carcinoma
| References | Age (yr) | Chemotherapy | Coma | Diagnosis before death | Survival (d) |
| 1 | 68 | No | Yes | No | 18 |
| 1 | 66 | No | Yes | Yes | 1 |
| 1 | 58 | No | Yes | No | 2 |
| 1 | 51 | Yes | No | Yes | 19 |
| 2 | 68 | No | No | Yes | 3 |
| 3 | 56 | Yes | No | Yes | >140 |
| 4 | 45 | Yes | No | Yes | 114 |
| 5 | 66 | No | Yes | No | 3 |
| 6 | 85 | No | Yes | No | 8 |
| 7 | 64 | No | Yes | No | 6 |
| 8 | 46 | No | Yes | No | 8 |
| 12 | 48 | No | No | No | 14 |
| 12 | 59 | No | No | No | 14 |
| 12 | 45 | No | No | No | 6 |
| 13 | 79 | No | No | No | 6 |
| 14 | 57 | No | No | No | 10 |
| 14 | 52 | No | No | No | 16 |
| 15 | 55 | Yes | No | No | 5 |
| 15 | 57 | NR1 | NR1 | No | NR1 |
| 16 | 46 | NR1 | NR1 | No | 9 |
| 17 | 65 | No | No | No | 20 |
| Present case | 71 | Yes | Yes | Yes | >182 |
NR: not reported.
This case presents an apparent dramatic response of tumor-related encephalopathy to the administration of chemotherapy. There was no evidence for other, more usual causes of encephalopathy. Although the combination of carboplatin and etoposide as first-line chemotherapy was effective to acute hepatic failure, it failed to exert any effect against rapid encephalopathy. However, the encephalopathy improved dramatically after the administration of amrubicin as second-line chemotherapy.
Amrubicin (SM-5887) is a totally synthetic anth-racycline and a potent topoisomerase II inhibitor[9], and is one of the most active agents for SCLC. In a phase II study of amrubicin using a schedule of 45 mg/m2 on d 1-3 every 3 wk in 33 previously untreated extensive-stage SCLC patients, an overall response rate of 76% and median survival of 11.7 mo have been observed[10]. In this case, amrubicin, as second-line chemotherapy, was effective for the improvement of encephalopathy and liver metastases. However, the efficacy of amrubicin as a salvage chemotherapy remains unknown.
Extremely high serum LDH level represents diffuse replacement of the liver parenchyma and is associated with a higher risk of developing FHF[2]. Several reports have shown correlation between serum LDH levels with survival in SCLC patients with liver metastases, and suggested an accurate relationship between elevated LDH levels and hepatic dysfunction[1,2,7]. These findings are in agreement with the LDH levels in our patient, who was observed with elevated LDH serum levels prior to chemotherapy, then regressing to normal LDH levels after the improvement of liver metastasis.
In the reports of malignant diseases manifesting as acute hepatic failure complicated by encephalopathy, a non-Hodgkin’s lymphoma patient responded to chemotherapy and survived FHF[11]. Once FHF develops secondary to diffuse liver metastases in cancer patients, prognosis is dismal and there is no effective treatment with the exception of chemotherapy. Our case, with supporting evidence from non-Hodgkin’s Lymphoma[11] and 2 cases of lactic acidosis[3,4], suggests that early diagnosis and a prompt administration of appropriate chemotherapy may result in the improvement of acute hepatic failure, and thereby improving survival.
Hence, we suggest that in addition to the efficacy of amrubicin as second-line chemotherapy, early diagnosis and prompt initiation of chemotherapy may result in the improvement of FHF, and thereby improving survival.
Footnotes
S- Editor Wang J L- Editor Kumar M E- Editor Ma WH
References
- 1.McGuire BM, Cherwitz DL, Rabe KM, Ho SB. Small-cell carcinoma of the lung manifesting as acute hepatic failure. Mayo Clin Proc. 1997;72:133–139. doi: 10.4065/72.2.133. [DOI] [PubMed] [Google Scholar]
- 2.Athanasakis E, Mouloudi E, Prinianakis G, Kostaki M, Tzardi M, Georgopoulos D. Metastatic liver disease and fulminant hepatic failure: presentation of a case and review of the literature. Eur J Gastroenterol Hepatol. 2003;15:1235–1240. doi: 10.1097/00042737-200311000-00014. [DOI] [PubMed] [Google Scholar]
- 3.Colman LK, Baker TM. Lactic acidosis with extensive oat cell carcinoma of the lung--not necessarily a poor prognostic sign: case report. Mil Med. 1983;148:440. [PubMed] [Google Scholar]
- 4.Rice K, Schwartz SH. Lactic acidosis with small cell carcinoma. Rapid response to chemotherapy. Am J Med. 1985;79:501–503. doi: 10.1016/0002-9343(85)90038-5. [DOI] [PubMed] [Google Scholar]
- 5.Ojeda VJ. Metastatic oat cell carcinoma simulating liver cirrhosis. N Z Med J. 1977;86:480–481. [PubMed] [Google Scholar]
- 6.Krauss EA, Ludwig PW, Sumner HW. Metastatic carcinoma presenting as fulminant hepatic failure. Am J Gastroenterol. 1979;72:651–654. [PubMed] [Google Scholar]
- 7.Harrison HB, Middleton HM 3rd, Crosby JH, Dasher MN Jr. Fulminant hepatic failure: an unusual presentation of metastatic liver disease. Gastroenterology. 1981;80:820–825. [PubMed] [Google Scholar]
- 8.Lin MS, Donati RM. "Mottled" liver scan in giant hepatomegaly due to intrasinusoidal metastasis of small cell lung cancer. Clin Nucl Med. 1981;6:496–497. [PubMed] [Google Scholar]
- 9.Noguchi T, Ichii S, Morisada S, Yamaoka T, Yanagi Y. In vivo efficacy and tumor-selective metabolism of amrubicin to its active metabolite. Jpn J Cancer Res. 1998;89:1055–1060. doi: 10.1111/j.1349-7006.1998.tb00496.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Yana T, Negoro S, Takada Y. Phase II study of amrubicin (SM-5887), a 9-amino-anthracycline, in previously untreated patients with extensive stage small-cell lung cancer (ES-SCLC): a West Japan Lung Cancer Group trial. Proc Am Soc Clin Oncol. 1998;17:450a Available from: URL; http: //www.asco.org/portal/site/ASCO. [Google Scholar]
- 11.Rowbotham D, Wendon J, Williams R. Acute liver failure secondary to hepatic infiltration: a single centre experience of 18 cases. Gut. 1998;42:576–580. doi: 10.1136/gut.42.4.576. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Watson KJ. Zinc abnormalities in fulminant hepatic failure. Aust N Z J Med. 1986;16:415–416. doi: 10.1111/j.1445-5994.1986.tb01206.x. [DOI] [PubMed] [Google Scholar]
- 13.Wesbey G. Lactic acidosis in oat cell carcinoma with extensive hepatic metastases. Arch Intern Med. 1981;141:816–817. [PubMed] [Google Scholar]
- 14.Spechler SJ, Esposito AL, Koff RS, Hong WK. Lactic acidosis in oat cell carcinoma with extensive hepatic metastases. Arch Intern Med. 1978;138:1663. [PubMed] [Google Scholar]
- 15.Sheriff DS. Lactic acidosis and small cell carcinoma of the lung. Postgrad Med J. 1986;62:297–298. doi: 10.1136/pgmj.62.726.297. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Galus M. Liver failure due to metastatic small-cell carcinoma of the lung. Mayo Clin Proc. 1997;72:791. doi: 10.1016/S0025-6196(11)63603-3. [DOI] [PubMed] [Google Scholar]
- 17.Ihara N, Yashiro N, Kinoshita T, Yoshigi J, Ouchi T, Narita M, Hattori C, Kaneko N. Diffuse intrasinusoidal liver metastasis of small cell lung cancer causing fulminant hepatic failure: CT findings-a case report. Radiat Med. 2001;19:275–277. [PubMed] [Google Scholar]