

Abstract
AIM: To ultrasonographicaly evaluate the acute effects of smoking on gallbladder contraction and refilling in chronic smokers and nonsmokers.
METHODS: Fifteen chronic smokers (21-30 years old) and fifteen nonsmokers (21-35 years old) participated in this study. Chronic smokers were selected among the volunteers who had been smoking for at least 5 years and 10 cigarettes per day (mean 17.5/d). Examinations were performed in two separate days. In the first day, basal gallbladder (GB) volumes of volunteers were measured after 8-h fasting. After the examinations, participants had a meal containing at least 30-40 gram fat. Gallbladder volume was assessed at 5, 15, 30, 60, 120 and 180 min after the meal. In the second day, participants smoked 2 cigarettes after 8-h fasting. Then, they had the same meal, and gallbladder measurements were repeated at the same time points. Same procedures were applied to both groups.
RESULTS: The mean starving GB volumes were 23.3 ± 3.3 mL in the first day, 21.9 ± 3.0 mL in the second day in nonsmoker group and 18.3 ± 3.0 mL in the first day, 19.5 ± 2.8 mL in second day in smoker group. There was no significant difference between starving GB volumes. We did not find any significant difference between the GB volumes measured at 5, 15, 30, 60, 120 and 180 min in the first and second days in nonsmoker group. In smokers, post cigarette GB volume was found significantly higher at 5, 15 and 30 min which corresponded to GB contraction phase (P < 0.05). Control GB volume measurements were not significantly different between the two groups. Post-smoking GB volumes were also not significantly different between the two groups.
CONCLUSION: Smoking prolongs the maximal GB emptying time both in smokers and in nonsmokers though it is not significant. It delays GB contraction in chronic smokers and causes a significant decrease in GB emptying volume. Smoking causes no significant delay in GB refilling in both smokers and nonsmokers. These effects of smoking observed in acute phase result in bile stasis in GB. Bile stasis is the underlying cause of most GB disorders in chronic process.
Keywords: Gallbladder, Emptying, Smoking, Ultra-sonography
INTRODUCTION
Smoking is still widespread in many societies despite the recognized relationship of it with many diseases. It is one of the risk factors for lung, stomach, larynx, esophagus, and some other cancers. Its association with lung cancer has been well described. Besides, smoking carries an important risk of developing cardiovascular diseases[1]. Chronic pulmonary diseases, gastric ulcers, and many other diseases are increased among smokers. Some reports showed that smoking increases the risk of gallbladder cancer[2]. Many prospective studies have found an association between smoking and clinical gallbladder disease[3-6]. On the other hand, no relation has been found between smoking and gallstone formation in some other reports[7,8]. A population-based study reported that sonographically detected gallbladder diseases are associated with smoking and are moderately increased in smokers[9]. Some epidemiologic researches focused on the relation of smoking and gallbladder diseases, but they have not found any positive relation[10,11]. There are a limited number of studies in the literature evaluating the effect of smoking on gallbladder motility by ultrasonography. Janderko et al[12] evaluated gallbladder contraction and refilling in chronic smokers by ultrasonography and found that refilling is delayed. In our study, we evaluated the gallbladder volume changes in contraction and refilling periods in both smokers and nonsmokers by ultrasonography. We compared the obtained data of both groups. To our knowledge, there is no other study in the literature evaluating the effects of smoking on gallbladder in the acute period in smokers and nonsmokers by ultrasonography.
MATERIALS AND METHODS
Subjects
Fifteen smoker (10 women and 5 men) and 15 nonsmoker volunteers (9 men and 6 women) were included in the study. The mean age of smokers was 24.2 years (21-30 years), and the mean age of nonsmokers was 28.1 years (21-34 years). Volunteers having smoked for at least 5 years were included in group of smokers. The mean smoking rate in this group was 17.5 cigarettes per day (10-25). None of the volunteers had gastrointestinal disorder, gallbladder disease, any disease like diabetes mellitus that could affect gallbladder, or any previous surgery of gastrointestinal tract. Prior to 48-h and during the study, no medicine or smoking was allowed. A preliminary gallbladder sonography was performed and only the volunteers without any gallbladder abnormality were included in the study. All participants gave their informed consent.
Study design
Gallbladder volumes of all volunteers were measured twice in two separate days. At least 8 h after the last meal, participants were taken into the dimly lighted sonography room at a temperature of 22-24°C. A 3.5 6 MHz convex broadband (tissue harmonic) abdominal transducer (Toshiba, Nemio, Tokyo-Japan) was established for the measurements. All measurements were performed in supine, left lateral, and lateral decubit positions in which gallbladder cross-sectional and longitudinal diameters were best visualized. The best imaging position of gallbladder was recorded for each participant and used in following measurements. The most appropriate transducer position was noted for each volunteer and marked on the skin. Cross-sectional diameters were calculated from the widest diameters measured during sonography. The longest axis of the gallbladder was established as the longitudinal diameter. The distance between internal margins of each opposite wall was used for the measurement of diameters. The subjects with significant folding of gallbladder or the subjects whose longitudinal diameter could not be viewed in a single frame were excluded from the study.
Longitudinal and cross-sectional diameter measure-ments were repeated three times and the mean of these three measurements was established. Gallbladder volume was calculated with the formula V = (π/6) × L ×W × H, where V = GB volume, L = GB length, W = GB width, H = GB height, as previously described[13].
Study methods
Gallbladder volumes of all volunteers were measured twice in two separate days. In the first day (control examination) after 8-h (at least) overnight fasting, basal GB volumes were measured. Then, 30-40 g fat-containing meal was given to the volunteers and participants were told to eat the meal up in 2 min. After that, GB volumes were measured at 5, 15, 30, 60, 120 and 180 min. Contraction phase as the measurements till 60 min, and refilling phase was presumed as the measurements at 120 and 180 min. To avoid the start of cephalic phase of digestion, volunteers and meals were kept in separate rooms until the examinations. In the second day (study examination), after an overnight fasting, two cigarettes were given to the participants who were encouraged to consume the cigarettes in 5-10 min with deep inhalations. Approximately 3 min after the smoking, a meal containing 30-40 g fat, was given to the volunteers. Then, GB volumes were measured at 5, 15, 30, 60, 120 and 180 min.The same procedures were repeated in smoker and nonsmoker groups.
GB volume changes versus time were presented graphically for both two groups using the pre- and post-smoking values (Figure 1A and 1B). Acquired data are shown on Tables 1 and 2 by comparing them between the two groups and within each group.
Figure 1.
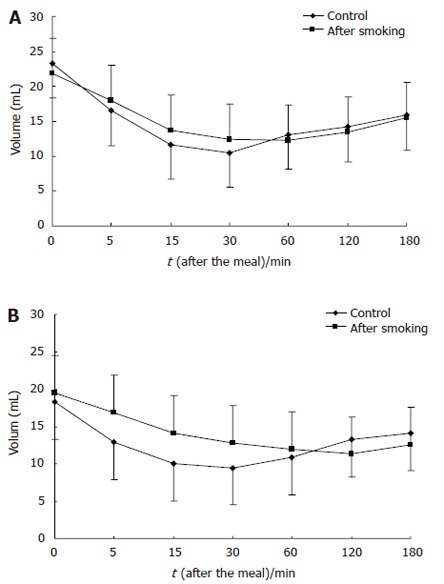
Effect of smoking on gallbladder emptying and refilling in nonsmokers (A) and smokers (B).
Table 1.
Postprandial gallbladder volumes after smoking in smokers and non-smokers (mean ± SD, mL)
| t/min |
Non smoker |
Smoker |
||||
| Control | After smoking | P | Control | After smoking | P | |
| 0 | 23.3 ± 3.3 | 21.9 ± 3.0 | 0.175 | 18.3 ± 3.0 | 19.5 ± 2.8 | 0.371 |
| 5 | 16.5 ± 2.9 | 18.0 ± 2.8 | 0.174 | 12.9 ± 2.1 | 16.9 ± 2.5 | 0.022 |
| 15 | 11.7 ± 2.5 | 13.7 ± 2.6 | 0.080 | 10.0 ± 1.5 | 14.1 ± 1.6 | 0.011 |
| 30 | 10.5 ± 1.9 | 12.4 ± 2.1 | 0.432 | 9.5 ± 1.6 | 12.8 ± 1.7 | 0.042 |
| 60 | 13.1 ± 2.4 | 12.3 ± 2.0 | 0.756 | 10.9 ± 1.5 | 12.0 ± 1.6 | 0.359 |
| 120 | 14.2 ± 2.5 | 13.5 ± 1.8 | 0.859 | 13.3 ± 2.9 | 11.3 ± 1.5 | 0.398 |
| 180 | 15.9 ± 2.5 | 15.5 ± 1.9 | 0.508 | 14.1 ± 2.9 | 12.6 ± 1.7 | 0.449 |
Table 2.
Postprandial gallbladder volumes after smoking in smokers and non-smokers (mean ± SD, mL)
| t/min |
Control |
After smoking |
||||
| Non smoker | Smoker | P | Non smoker | Smoker | P | |
| 0 | 23.3 ± 3.3 | 18.3 ± 3.0 | 0.360 | 21.9 ± 3.0 | 19.5 ± 2.8 | 0.604 |
| 5 | 16.5 ± 2.9 | 12.9 ± 2.1 | 0.392 | 18.0 ± 2.8 | 16.9 ± 2.5 | 0.783 |
| 15 | 11.7 ± 2.5 | 10.0 ± 1.5 | 0.623 | 13.7 ± 2.6 | 14.1 ± 1.6 | 0.883 |
| 30 | 10.5 ± 1.9 | 9.5 ± 1.6 | 0.732 | 12.4 ± 2.1 | 12.8 ± 1.7 | 0.883 |
| 60 | 13.1 ± 2.4 | 10.9 ± 1.5 | 0.513 | 12.3 ± 2.0 | 12.0 ± 1.6 | 0.909 |
| 120 | 14.2 ± 2.5 | 13.3 ± 2.9 | 0.839 | 13.5 ± 1.8 | 11.3 ± 1.5 | 0.318 |
| 180 | 15.9 ± 2.5 | 14.1 ± 2.9 | 0.701 | 15.5 ± 1.9 | 12.6 ± 1.7 | 0.295 |
Statistical analysis
Values are presented as mean ± SD. The paired and two-tailed Student’s t tests were used. P < 0.05 was considered statistical significant.
RESULTS
There was no difference in body mass index and age between smokers and nonsmokers. The mean fasting GB volume in nonsmoker group was 23.3 ± 3.3 mL in the first day and 21.9 ± 3.0 mL in the second day, and was 18.3 ± 3.0 mL in the first day and 19.5 ± 2.8 mL in the second day in smoker group. Although the fasting GB volumes did not differ significantly, these values were lower in smoker group. In the first day, minimum GB volumes (in other words, maximal GB emptying) were measured at 30 min in both groups.
However, the post-smoking measurements in the second day were performed at 60 postprandial minute in nonsmoker group, and at 120 min in smoker group (Figures 1A and 1B). Smoking delayed the maximal GB emptying in both smokers and nonsmokers. Besides, in both groups, GB refilling was faster in the first day and slowed down in the second day (Figure 1A and 1B). In nonsmoker group, GB volumes measured at 5, 15, 30, 60, 120 and 180 min in the first and second days were not significantly different (Table 1). GB volume was significantly higher in smoker group at GB contraction phase (5, 15 and 30 min) after the two cigarettes were smoked (P < 0.05, Table 1). There was no significant difference between two groups both in basal GB volume measurements and in post-smoking measurements between the two groups (Table 2).
DISCUSSION
In this study, we showed the disrupted GB contractility in smokers and delayed maximal GB emptying both in smokers and nonsmokers just after smoking. Although our study group was small in size, basal GB volume had a tendency to be lower in smokers than in nonsmokers. However, this difference was not statistically significant. Many epidemiologic studies have reported a mild or moderate association between smoking and gallstone or postcholecystectomic state[4,6,10,11]. On the other hand, no association has been detected between smoking and gall stone formation[7,8,14]. It is not clear which biologic mechanism is mediated in the predisposition of smoking to gallstone formation. Some authors suggested that smoking lowers the plasma high-density lipoprotein cholesterol level which increases risk of gall stone formation by decreasing hepatic excretion of the bile acids[15]. Estrogen is blamed for gall stone formation because of high incidence of gallstone in women. In respect to this, some studies have shown high plasma estrogen level in smokers[16], while some others have not found any significant difference[17].Cholecystokinin, a proximal gout hormone, is a well known mediator of GB contraction[18]. It is the main determining factor for the postprandial GB discharge. Cholecystokinin starts GB contraction by affecting the pre-ganglionic cholinergic nerves. Cholecystokinin is released from mucosa cells by the arrival of stomach content that is rich in fat and protein to the small intestine[19]. Smoking exerts an inhibitory effect on intestinal and gastric motility[20-22]. As a result of decreased gut motility and delayed gastric emptying, cholecystokinin release is also decreased or delayed. Therefore, decreased GB contractility can be expected. However, in our study, smoking caused a nonsignificant and minimal decrease of GB contractility in nonsmoker volunteers. In addition, GB volume was slightly increased in post-smoking contraction phase in this group (Figure 1A). Previous studies have also reported similar results[23]. On the other hand, we showed a significant difference of GB volume in post-smoking early contraction phase (postprandial 5, 15 and 30 min) of smokers (Table 2). It was also significantly higher in post-smoking 5, 15 and 30 min (Figure 1B). To the best of our knowledge, no data are available on whether this delay of GB contraction in smokers results from a disruption in the smooth muscle contraction mechanism of GB wall or from the delay of the blood cholecystokinin increase due to delayed gastric emptying. One of the limitations of this study is that the blood levels of cholecystokinin were not measured. According to Jonderko et al[12], smoking delays GB refilling at acute phase in chronic smokers. Our results also showed that GB refilling was delayed after smoking both in smokers and in nonsmokers although not significant. Smoking suppresses pancreatic polypeptide release which plays an important role in GB refilling[24,25].
In humans, disruption of GB emptying is associated with gallstone formation[26]. Bile stasis and disrupted GB motility are important factors for gallstone formation[27,28]. Delayed gallbladder emptying and reduced muscle contractility occur in chronic calculus, or in gallstone, cholecystitis[29,30]. It was reported that acalculous cholecystitis is formed after inhalation of intense cigarette smoke in dogs[31]. Impairment of gallbladder contractility may contribute to the clinicopathology of acalculous cholecystitis[32].
In our study, smoking caused a nonsignificant prolongation of the maximal GB emptying time both in smokers and in nonsmokers at acute phase, delayed GB contraction in smokers, and decreased the GB emptying volume. Besides, smoking did not delay GB refilling significantly in both groups. Because of all these acute effects, smoking comprises a risk for GB diseases. In the chronic process, smoking may have these effects by affecting GB smooth muscle contraction or by decreasing cholecystokinin release via the inhibition of intestinal motility, or by both. In vitro studies are needed to evaluate the effects of smoking on gallbladder smooth muscles and laboratory studies are required to show its effects on cholecystokinin release.
Footnotes
S- Editor Wang J L- Editor Wang XL E- Editor Bai SH
References
- 1.Jonas MA, Oates JA, Ockene JK, Hennekens CH. Statement on smoking and cardiovascular disease for health care professionals. American Heart Association. Circulation. 1992;86:1664–1669. doi: 10.1161/01.cir.86.5.1664. [DOI] [PubMed] [Google Scholar]
- 2.Khan ZR, Neugut AI, Ahsan H, Chabot JA. Risk factors for biliary tract cancers. Am J Gastroenterol. 1999;94:149–152. doi: 10.1111/j.1572-0241.1999.00786.x. [DOI] [PubMed] [Google Scholar]
- 3.Diehl AK, Haffner SM, Hazuda HP, Stern MP. Coronary risk factors and clinical gallbladder disease: an approach to the prevention of gallstones. Am J Public Health. 1987;77:841–845. doi: 10.2105/ajph.77.7.841. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kono S, Shinchi K, Ikeda N, Yanai F, Imanishi K. Prevalence of gallstone disease in relation to smoking, alcohol use, obesity, and glucose tolerance: a study of self-defense officials in Japan. Am J Epidemiol. 1992;136:787–794. doi: 10.1093/aje/136.7.787. [DOI] [PubMed] [Google Scholar]
- 5.Murray FE, Logan RF, Hannaford PC, Kay CR. Cigarette smoking and parity as risk factors for the development of symptomatic gall bladder disease in women: results of the Royal College of General Practitioners' oral contraception study. Gut. 1994;35:107–111. doi: 10.1136/gut.35.1.107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Kato I, Nomura A, Stemmermann GN, Chyou PH. Prospective study of clinical gallbladder disease and its association with obesity, physical activity, and other factors. Dig Dis Sci. 1992;37:784–790. doi: 10.1007/BF01296440. [DOI] [PubMed] [Google Scholar]
- 7.Chen CY, Lu CL, Lee PC, Wang SS, Chang FY, Lee SD. The risk factors for gallstone disease among senior citizens: an Oriental study. Hepatogastroenterology. 1999;46:1607–1612. [PubMed] [Google Scholar]
- 8.Attili AF, Capocaccia R, Carulli N, Festi D, Roda E, Barbara L, Capocaccia L, Menotti A, Okolicsanyi L, Ricci G, et al. Factors associated with gallstone disease in the MICOL experience. Multicenter Italian Study on Epidemiology of Cholelithiasis. Hepatology. 1997;26:809–818. doi: 10.1002/hep.510260401. [DOI] [PubMed] [Google Scholar]
- 9.Misciagna G, Leoci C, Guerra V, Chiloiro M, Elba S, Petruzzi J, Mossa A, Noviello MR, Coviello A, Minutolo MC, et al. Epidemiology of cholelithiasis in southern Italy. Part II: Risk factors. Eur J Gastroenterol Hepatol. 1996;8:585–593. doi: 10.1097/00042737-199606000-00017. [DOI] [PubMed] [Google Scholar]
- 10.Okamoto M, Yamagata Z, Takeda Y, Yoda Y, Kobayashi K, Fujino MA. The relationship between gallbladder disease and smoking and drinking habits in middle-aged Japanese. J Gastroenterol. 2002;37:455–462. doi: 10.1007/s005350200066. [DOI] [PubMed] [Google Scholar]
- 11.Kono S, Eguchi H, Honjo S, Todoroki I, Oda T, Shinchi K, Ogawa S, Nakagawa K. Cigarette smoking, alcohol use, and gallstone risk in Japanese men. Digestion. 2002;65:177–183. doi: 10.1159/000064938. [DOI] [PubMed] [Google Scholar]
- 12.Jonderko K, Nowak A, Kasicka-Jonderko A, Błaszczyńska M. Effect of cigarette smoking on gallbladder emptying and filling in man. Am J Gastroenterol. 1994;89:67–71. [PubMed] [Google Scholar]
- 13.Dodds WJ, Groh WJ, Darweesh RM, Lawson TL, Kishk SM, Kern MK. Sonographic measurement of gallbladder volume. AJR Am J Roentgenol. 1985;145:1009–1011. doi: 10.2214/ajr.145.5.1009. [DOI] [PubMed] [Google Scholar]
- 14.Layde PM, Vessey MP, Yeates D. Risk factors for gall-bladder disease: a cohort study of young women attending family planning clinics. J Epidemiol Community Health. 1982;36:274–278. doi: 10.1136/jech.36.4.274. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Criqui MH, Wallace RB, Heiss G, Mishkel M, Schonfeld G, Jones GT. Cigarette smoking and plasma high-density lipoprotein cholesterol. The Lipid Research Clinics Program Prevalence Study. Circulation. 1980;62:IV70–IV76. [PubMed] [Google Scholar]
- 16.Khaw KT, Tazuke S, Barrett-Connor E. Cigarette smoking and levels of adrenal androgens in postmenopausal women. N Engl J Med. 1988;318:1705–1709. doi: 10.1056/NEJM198806303182601. [DOI] [PubMed] [Google Scholar]
- 17.Dai WS, Gutai JP, Kuller LH, Laporte RE, Falvo-Gerard L, Caggiula A. Relation between plasma high-density lipoprotein cholesterol and sex hormone concentrations in men. Am J Cardiol. 1984;53:1259–1263. doi: 10.1016/0002-9149(84)90075-4. [DOI] [PubMed] [Google Scholar]
- 18.Niebergall-Roth E, Teyssen S, Singer MV. Neurohormonal control of gallbladder motility. Scand J Gastroenterol. 1997;32:737–750. doi: 10.3109/00365529708996528. [DOI] [PubMed] [Google Scholar]
- 19.Shaffer EA. Review article: control of gall-bladder motor function. Aliment Pharmacol Ther. 2000;14 Suppl 2:2–8. doi: 10.1046/j.1365-2036.2000.014s2002.x. [DOI] [PubMed] [Google Scholar]
- 20.Watanabe Y, Fujiwara Y, Shiba M, Watanabe T, Tominaga K, Oshitani N, Matsumoto T, Nishikawa H, Higuchi K, Arakawa T. Cigarette smoking and alcohol consumption associated with gastro-oesophageal reflux disease in Japanese men. Scand J Gastroenterol. 2003;38:807–811. doi: 10.1080/00365520310004506. [DOI] [PubMed] [Google Scholar]
- 21.Nowak A, Jonderko K, Kaczor R, Nowak S, Adamczak D, Rudzki K. Inhibitory effect of cigarette smoking on gastric emptying of a solid meal in patients with type I gastric ulcer. Z Gastroenterol. 1991;29:45–48. [PubMed] [Google Scholar]
- 22.Miller G, Palmer KR, Smith B, Ferrington C, Merrick MV. Smoking delays gastric emptying of solids. Gut. 1989;30:50–53. doi: 10.1136/gut.30.1.50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Jonderko K, Sliwinski Z, Lelek A, Kaczor R. Effect of cigarette smoking on the fasted gallbladder volume in man. Ital J Gastroenterol. 1989;21:337–339. [Google Scholar]
- 24.Seino Y, Tsuda K, Mori K, Takemura J, Kuzuya H, Yamamura T, Kotoura Y, Ito N, Imura H. Effect of smoking on gastrointestinal hormone secretion. In: Proceedings on the 5th world conference, smoking and health., editors. Winnipeg, Canada: Canadian Council on Smoking and Health; 1983. pp. 207–212. [Google Scholar]
- 25.Conter R, Roslyn JJ, Muller EL, Pitt HA, Porter-Fink V, DenBesten L, Taylor IL. Effect of pancreatic polypeptide on gallbladder filling. J Surg Res. 1985;38:461–467. doi: 10.1016/0022-4804(85)90062-9. [DOI] [PubMed] [Google Scholar]
- 26.Forgacs IC, Maisey MN, Murphy GM, Dowling RH. Influence of gallstones and ursodeoxycholic acid therapy on gallbladder emptying. Gastroenterology. 1984;87:299–307. [PubMed] [Google Scholar]
- 27.Admirand WH, Small DM. The physicochemical basis of cholesterol gallstone formation in man. J Clin Invest. 1968;47:1043–1052. doi: 10.1172/JCI105794. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Baxter JN. Gall-bladder emptying. J Gastroenterol Hepatol. 1989;4:353–372. doi: 10.1111/j.1440-1746.1989.tb00847.x. [DOI] [PubMed] [Google Scholar]
- 29.Behar J, Lee KY, Thompson WR, Biancani P. Gallbladder contraction in patients with pigment and cholesterol stones. Gastroenterology. 1989;97:1479–1484. doi: 10.1016/0016-5085(89)90392-2. [DOI] [PubMed] [Google Scholar]
- 30.Fisher RS, Rock E, Malmud LS. Cholinergic effects on gallbladder emptying in humans. Gastroenterology. 1985;89:716–722. doi: 10.1016/0016-5085(85)90564-5. [DOI] [PubMed] [Google Scholar]
- 31.Dillon L, Glenn F, Becker CG. Induction of acalculous cholecystitis and pneumonitis in dogs following inhalation of constituents of cigarette smoke condensate. Am J Pathol. 1982;109:253–258. [PMC free article] [PubMed] [Google Scholar]
- 32.Parkman HP, James AN, Bogar LJ, Bartula LL, Thomas RM, Ryan JP, Myers SI. Effect of acalculous cholecystitis on gallbladder neuromuscular transmission and contractility. J Surg Res. 2000;88:186–192. doi: 10.1006/jsre.1999.5788. [DOI] [PubMed] [Google Scholar]