

Abstract
Objective
To examine the associations of foot posture and foot function to foot pain.
Methods
Data were collected on 3,378 members of the Framingham Study who completed foot examinations in 2002–2008. Foot pain (generalized and at six locations) was based on the response to the question “On most days, do you have pain, aching or stiffness in either foot?” Foot posture was categorized as normal, planus or cavus using static pressure measurements of the arch index. Foot function was categorized as normal, pronated or supinated using the center of pressure excursion index from dynamic pressure measurements. Sex-specific multivariate logistic regression models were used to examine the effect of foot posture and function on generalized and location-specific foot pain, adjusting for age and weight.
Results
Planus foot posture was significantly associated with an increased likelihood of arch pain in men (odds ratio [OR] 1.38, 95% confidence interval [CI] 1.01 – 1.90), while cavus foot posture was protective against ball of foot pain (OR 0.74, 95% CI 0.55 – 1.00) and arch pain (OR 0.64, 95% CI 0.48 – 0.85) in women. Pronated foot function was significantly associated with an increased likelihood of generalized foot pain (OR 1.28, 95% CI 1.04 – 1.56) and heel pain (OR 1.54, 95% CI 1.04 – 2.27) in men, while supinated foot function was protective against hindfoot pain in women (OR 0.74, 95% CI 0.55 – 1.00).
Conclusion
Planus foot posture and pronated foot function are associated with foot symptoms. Interventions that modify abnormal foot posture and function may therefore have a role in the prevention and treatment of foot pain.
Foot pain and foot-related disability are very common in the general population. Population-based studies indicate that 24% of people aged over 45 years report frequent foot pain, and of these, approximately two-thirds report at least moderate disability in an aspect of daily life related to their foot condition (1). Foot disorders have been shown to have a detrimental impact on health-related quality of life across a spectrum of age-groups (2) and are responsible for a substantial proportion of primary care consultations (3) and surgical interventions (4). Despite the high prevalence and significant impact of foot pain, relatively little is known about the underlying risk factors for its development beyond increased age (2), female sex (5–7), obesity (2, 6, 8, 9) and chronic medical conditions such as osteoarthritis and diabetes (2, 7, 8). However, one potentially modifiable risk factor for foot pain that is commonly suggested in the literature is abnormal foot structure and function, based on the premise that variations in the skeletal architecture of the foot may result in altered walking patterns and contribute to excessive loading of osseous and soft tissue structures (10).
Foot posture is generally characterized by the contour of the medial longitudinal arch, and is typically divided into normal (rectus), low-arched (planus), or highly-arched (cavus) categories. Several techniques, including visual estimation, footprint parameters and radiographic evaluation have been used to classify foot posture, however there is no clear consensus as to which is the most appropriate approach (11). As a consequence of this variability, the literature pertaining to the contribution of foot posture and function to foot symptoms is inconsistent. While some studies have reported associations between planus and cavus foot types and a range of lower limb conditions (12–16), others have not (17–19). Furthermore, most studies investigating this association have focused on specific clinical groups such as athletes or military recruits, so their findings may not be applicable to the general population.
Only three population-based studies have explored the relationship between foot posture and foot problems. An analysis of the US National Health Interview Survey of 74,721 adults conducted in 1990 found that self-reported “flat foot” was associated with self-reported calluses, hammertoes and bunions, however foot symptoms were not documented (20). The Cheshire Foot Pain and Disability Survey of 3,417 people reported that both flat feet and highly arched feet (determined by self-report) were associated with foot pain, but no association was evident when a subset of the sample had their foot posture assessed by a clinician (7). More recently, a cross-sectional postal survey of 2,100 adults in Denmark found that self-reported foot deformity (categorized as either planus or cavus, based on line drawings) was significantly associated with foot pain present for at least one day in the past month (21). Each of these studies, however, is limited by the lack of an objective measure of foot posture. In addition, static assessment of foot posture does not adequately capture the functional role of the foot during gait. It is possible that the dynamic function of the foot, rather than its static morphology, may play a greater role in the development of foot symptoms by influencing the loads placed on osseous and soft tissue structures when walking (10). However, due to the significant data collection and processing requirements of gait analysis systems, this has yet to be explored in detail. As such, there remains a need to examine the relationship between foot structure, function and pain using objective, validated measures in a large population-based sample.
Therefore, the objective of this study was to evaluate the associations of foot posture and dynamic foot function to foot pain in men and women who participated in the Framingham Foot Study. We hypothesized that people with planus or cavus foot posture would be more likely to report foot pain than those with normal foot posture. Similarly, we hypothesized that people classified as having pronated or supinated feet when walking would be more likely to report foot pain than those with normal dynamic foot function. We examined these associations for both generalized foot pain and for foot pain present at six specific locations on the foot.
PARTICIPANTS AND METHODS
Participants
The study sample, the Framingham Foot Study cohort, was derived from two large, population-based samples of residents of Framingham, Massachusetts (22). The majority of the cohort was comprised of members from the Framingham Study Original Cohort and the Framingham Offspring Cohort. The Framingham Study Original Cohort was formed in 1948 from a two-thirds sample of the town of Framingham, MA in order to study risk factors for heart disease (23). This cohort has been followed biennially since that time. The Framingham Offspring cohort, formed in 1972, consists of adult offspring who had a parent in the Original Cohort, and the spouses of the offspring (24). This group has been followed every four years since cohort inception to study familial risk factors for heart disease. Members of the Framingham cohorts were examined for the current study either at their scheduled Framingham clinic examination or at a call-back examination.
The second population-based group used for the study was a new population sample that was derived from census-based, random-digit dialing within the Framingham community, selecting subjects who were ≥50 years old and ambulatory. This group was added to the Framingham Foot Study recruitment to increase participation by minority persons and other community members of the Framingham catchment area. Persons contacted via the random-digit dialing methodology who were interested in being part of a multi-phasic physical examination (foot, osteoarthritis, bone health, and general health), received a written letter of invitation to join the study and a follow-up phone call to schedule a study appointment. All Framingham Foot Study participants gave informed consent for the data collection and this study has undergone institutional review by both the Hebrew SeniorLife and the Boston University Medical Center Institutional Review Boards.
From these combined population-based cohorts, the Framingham Foot Study conducted a physical examination of the foot, and collected participant history, performance measures, and other data via questionnaire. A validated foot examination with specific criteria was used to assess presence of common foot disorders based upon visual inspection and/or palpation, and queries of foot pain and foot symptoms. Foot pain was assessed using an NHANES-based query about foot pain (see Foot Pain Assessment). Trained clinical examiners performed all foot examinations. All participants were ambulatory and cognitively intact (as indicated by mini-mental status score screening to identify qualified study subjects who would be able to give symptom information about their feet).
Foot Pain Assessment
Foot pain was assessed in 1,477 men and 1,901 women in the population-based Framingham Foot Study between 2002–2008. Generalized foot pain was measured using the following National Health and Nutrition Examination Survey-based query about foot pain: “On most days, do you have pain, aching, or stiffness in either of your feet?” Possible responses were no; yes, left foot only; yes, right foot only; yes, both feet; yes, not sure what side; and unknown. Foot pain at specific locations (on both feet) was also assessed. Participants were given a picture of the top and bottom of the foot and were asked to point out any areas with pain, aching, or stiffness on most days (Figure 1). The identifiable areas were the toes, forefoot, hindfoot, heel, arch of the foot, and ball of the foot.
Figure 1.
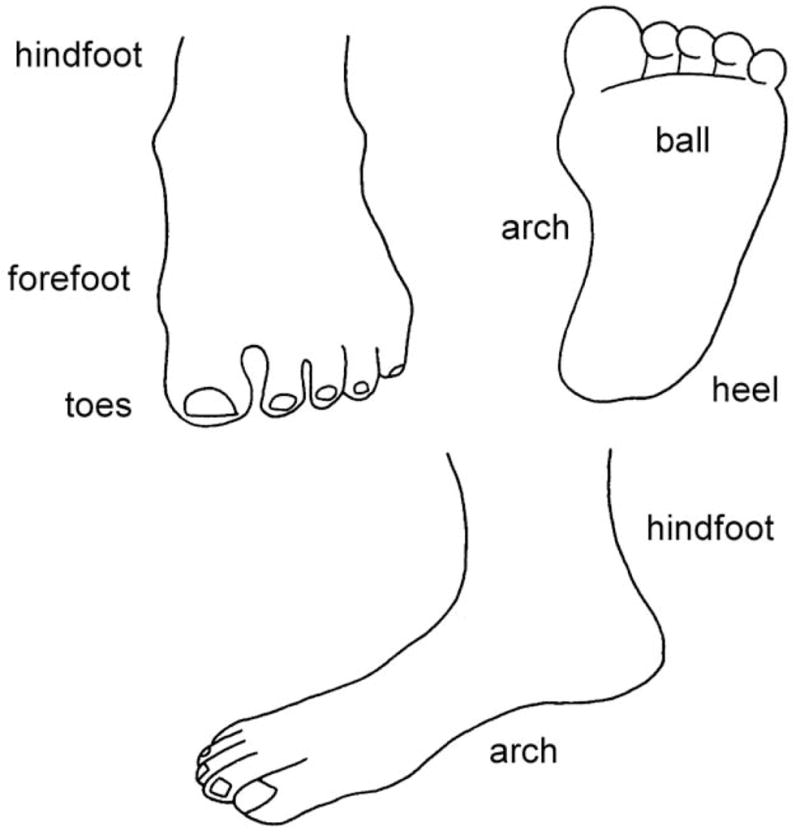
Foot map used to determine the location of foot pain (from Dufour AB, Broe KE, Nguyen US, Gagnon DR, Hillstrom HJ, Walker AH, et al. Foot pain: is current or past shoewear a factor? Arthritis Rheum 2009;61:1352–1358.)
Foot Posture and Function Assessment
Several methods for categorising feet into structural and functional groups have been reported in the literature (11), but there is currently no consensus as to which is the most appropriate technique. For the purpose of this study, we defined foot posture as the shape of the medial longitudinal arch of the foot when weightbearing, and assigned the labels “planus” to indicate a low-arched foot, and “cavus” to indicate a high-arched foot. Because the static posture of the foot may not always be indicative of how it functions, we also defined foot function according to how the foot moves when walking. We assigned the labels “pronated” to indicate a foot that undergoes greater lowering of the medial longitudinal arch and more medial distribution of plantar loading during gait and “supinated” to indicate a foot that undergoes greater elevation of the medial longitudinal arch and more lateral distribution of plantar loading during gait.
Foot posture and function were both assessed using the Tekscan® MatScan® system (Tekscan Inc, Boston, MA). The system consists of a 5 mm thick floor mat (432 × 368 mm), comprising of 2288 resistive sensors (1.4 sensors/cm2), and sampling data at a frequency of 40 Hz. The reliability of this system has been described in detail previously (25). Two types of scans were collected: standing and walking. For the standing scan, a one-frame self-selected bipedal stance “snap shot” image was collected for each participant. For the walking scans, participants walked across the mat at a self-selected pace using the two-step method, which involves striking the platform on the second step (26). One walking trial of each foot was recorded.
Foot posture was assessed using the arch index (AI), first described by Cavanagh and Rogers (27). From the maximum peak pressure image of the participant’s bipedal relaxed stance, the AI was calculated as the ratio of the area of the middle third of the footprint to the entire footprint area (excluding the toes), with a higher value representing a flatter foot (Figure 2). AI scores have previously been shown to be highly correlated with navicular height (28, 29) and angular medial longitudinal arch measures (29–32) obtained from foot radiographs. AI scores were divided into quintiles for men and women separately, and foot posture categorized as cavus (those in the lowest 20%), normal (those in the middle 60%) or planus (those in the highest 20%). The cut-off scores to define each category were as follows: cavus (0 – 0.134, n= 536 feet), normal (0.135 – 0.272, n= 1612 feet) and planus (0.273 – 0.565, n= 538 feet) for men, and cavus (0 – 0.119, n= 684 feet), normal (0.120 – 0.261, n=2,056 feet) and planus (0.262 – 0.534, n= 692 feet) for women.
Figure 2.
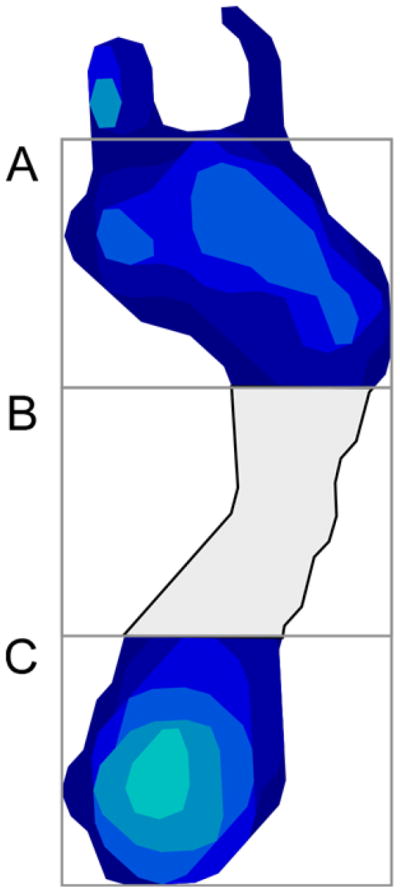
Calculation of the arch index (AI). The length of the static footprint excluding the toes is divided into equal thirds. The AI is then calculated as the area of the middle third of the footprint divided by the entire footprint area (AI = B/A + B + C).
Foot function was assessed by calculating the center of pressure excursion index (CPEI) of the walking trials. The CPEI represents the degree of medio-lateral deviation of the center of pressure at the anterior one-third trisection of the foot, relative to a line connecting the first and last center of pressure data points (see Figure 3). To calculate the CPEI, the maximum peak pressure image of a dynamic footprint was divided into thirds. A construction line was drawn from the first to the last center of pressure data point. A line (AD) was constructed at the anterior one-third trisection of the foot. The distance between the intersection of the construction line and line AD (point B) and where the center of pressure intersects with line AD (point C) was measured. The CPEI was then calculated by normalizing the distance BC to the width of the foot (AD), so CPEI = BC/AD *100. In a pronated foot, the concavity of the center of pressure curve is decreased, resulting in a smaller CPEI value. In a supinated foot, the concavity of the center of pressure curve is increased, resulting in a larger CPEI value. The CPEI has previously been shown to demonstrate excellent intra- and inter-tester reliability (intra-class correlation coefficients of 0.97 and 0.98, respectively) (33). As with AI scores, CPEI scores were then divided into sex-specific quintiles, and participants were categorized as having supinated foot function (those in the highest 20%), normal foot function (those in the middle 60%) or pronated foot function (those in the lowest 20%). The cut-off scores to define each category were as follows: supinated (22.5 – 43.7), normal (9.4 – 22.4) and pronated (−25.3 – 9.3) for men, and supinated (19.5 – 40.4), normal (6.1 – 19.4) and pronated (−20.6 – 6.0) for women.
Figure 3.

Calculation of the center of pressure excursion index from dynamic walking footprint. See text for explanation.
Typical examples of cavus, normal and planus foot posture and supinated, normal and pronated foot function categories using this classification system are shown in Figure 4.
Figure 4.
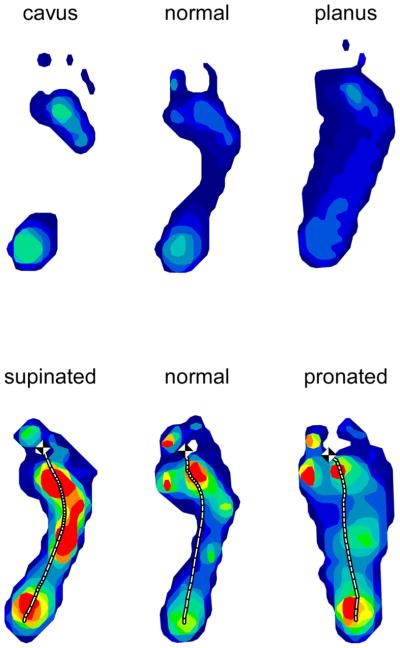
Typical examples of cavus, normal and planus static foot posture categories (top) and supinated, normal and pronated dynamic foot function categories (bottom).
Covariates
Because age and weight are both associated with foot pain, foot posture and foot function, these variables were considered to be potential confounders in our analysis. Age in years at the time of examination was recorded. Weight was measured using a standardized balance beam and recorded to the nearest half pound.
Statistical Analysis
Because sex is a strong confounder for both foot pain and foot function, all analyses were performed as sex-specific. Descriptive statistics were generated separately for men and women as means and standard deviations or percentages, where appropriate. In order to use the full array of data that were collected on right feet and left feet, a per-foot analysis was performed, using sex-specific generalized estimation equations (GEE), to account for the correlation between right and left feet. Odds ratios and 95% confidence intervals were calculated for the association between (i) foot pain and foot posture and (ii) foot pain and foot function, adjusting for age and weight. All analyses were conducted using the SAS statistical analysis package, version 9.1 (SAS Institute, Cary, NC).
RESULTS
Of the 3,378 participants in the Framingham Foot Study, 3,197 completed the foot questionnaire and had valid foot pressure data to calculate the AI and CPEI (1,403 men and 1,794 women), contributing a total of 6,394 feet to this analysis. Of the 6,394 feet, 6,118 feet had complete foot posture data and 5,794 feet had complete foot function data. The mean age of participants was 66 years (range 36–100 years) and 56% of the sample was female. The mean height and weight were 65.5 inches and 174.0 pounds, respectively. Table 1 shows the characteristics of the study sample by sex. Participants missing data on foot posture or on foot function were similar to the included observations in terms of age, weight and generalized foot pain.
Table 1.
Descriptive characteristics of men and women in the Framingham Foot Study with complete biomechanical foot examinations.
| Characteristic | Men (n=1,403) (n feet=2,806) | Women (n=1,794) (n feet=3,588) |
|---|---|---|
| Age, mean ± SD years | 66.19 ± 10.11 | 66.16 ± 10.76 |
| Weight, mean ± SD pounds | 193.81 ± 34.49 | 158.83 ± 36.11 |
| Foot pain | ||
| Generalized foot pain, n (%) | 414 (14.8) | 853 (23.8) |
| Toe pain, n (%) | 198 (7.1) | 438 (12.2) |
| Ball of foot pain, n (%) | 129 (4.6) | 300 (8.4) |
| Forefoot pain, n (%) | 122 (4.4) | 334 (9.3) |
| Arch pain, n (%) | 149 (5.3) | 290 (8.1) |
| Heel pain, n (%) | 136 (4.9) | 222 (6.2) |
| Hindfoot pain, n (%) | 144 (5.1) | 255 (7.1) |
| Foot disorders | ||
| Hallux valgus, n (%) | 470 (16.8) | 1,292 (36.0) |
| Hammertoes, n (%) | 472 (16.8) | 644 (18.0) |
| Overlapping toes, n (%) | 142 (5.1) | 243 (6.8) |
| Plantar fasciitis, n (%) | 81 (2.9) | 131 (3.7) |
| Morton’s neuroma, n (%) | 185 (6.6) | 324 (9.0) |
| Hallux rigidus, n (%) | 123 (4.4) | 113 (3.2) |
| Tailor’s bunion, n (%) | 69 (2.5) | 168 (4.7) |
Note: Means provided across individuals; numbers and % reflect number of feet in the study.
Of the 6,394 feet under study, 20% reported the presence of generalized foot pain on most days. Table 1 also shows the sex-specific distribution of the report of foot pain, both generalized and at specific locations, along with common foot disorders. Generalized foot pain on either foot was reported by 15% of the men and 24% of the women.
The associations between foot posture and foot pain in men and women, adjusted for age and weight, are presented in Table 2. Compared to the normal foot posture referent group, planus foot posture was significantly associated with a 30% increased likelihood of arch pain in men, while cavus foot posture was associated with a 26% decreased likelihood of ball of foot pain and a 36% decreased likelihood of arch pain in women.
Table 2.
Odds ratios (ORs) and 95% confidence intervals (CIs) for the association between static foot posture and foot pain in the men and women of the Framingham Foot Study (2002–2008), adjusted for age and weight.
|
|
||||
|---|---|---|---|---|
| Men | Women | |||
|
| ||||
| OR (95% CI) | P | OR (95% CI) | P | |
| Generalized foot pain | ||||
| Cavus vs. normal | 0.94 (0.74 – 1.20) | 0.620 | 0.83 (0.69 – 1.01) | 0.065 |
| Planus vs. normal | 1.20 (0.96 – 1.49) | 0.104 | 1.03 (0.88 – 1.20) | 0.705 |
| Toe pain | ||||
| Cavus vs. normal | 1.16 (0.84 – 1.60) | 0.380 | 1.03 (0.82 – 1.28) | 0.804 |
| Planus vs. normal | 1.21 (0.84 – 1.74) | 0.304 | 0.97 (0.80 – 1.18) | 0.756 |
| Ball of foot pain | ||||
| Cavus vs. normal | 0.73 (0.49 – 1.08) | 0.117 | 0.74 (0.55 – 1.00) | 0.048 |
| Planus vs. normal | 1.01 (0.74 – 1.37) | 0.956 | 0.97 (0.80 – 1.16) | 0.713 |
| Forefoot pain | ||||
| Cavus vs. normal | 1.25 (0.86 – 1.84) | 0.242 | 0.79 (0.59 – 1.06) | 0.119 |
| Planus vs. normal | 0.97 (0.64 – 1.47) | 0.891 | 0.97 (0.78 – 1.20) | 0.749 |
| Arch pain | ||||
| Cavus vs. normal | 1.00 (0.73 – 1.36) | 0.998 | 0.64 (0.48 – 0.85) | 0.002 |
| Planus vs. normal | 1.38 (1.01 – 1.90) | 0.044 | 1.03 (0.85 – 1.25) | 0.732 |
| Heel pain | ||||
| Cavus vs. normal | 0.82 (0.51 – 1.29) | 0.385 | 0.88 (0.60 – 1.30) | 0.523 |
| Planus vs. normal | 1.29 (0.89 – 1.87) | 0.179 | 0.88 (0.69 – 1.12) | 0.305 |
| Hindfoot pain | ||||
| Cavus vs. normal | 1.00 (0.69 – 1.45) | 0.980 | 0.84 (0.59 – 1.20) | 0.330 |
| Planus vs. normal | 1.29 (0.89 – 1.86) | 0.176 | 1.15 (0.91 – 1.45) | 0.246 |
In a similar fashion, the associations between foot function and foot pain are shown in Table 3 for men and women, adjusted for age and weight. Compared to the normal foot function referent group, pronated foot function was significantly associated with a 28% increased likelihood of generalized foot pain and a 54% increased likelihood of heel pain in men, while supinated foot function was associated with a 26% decreased likelihood of hindfoot pain in women.
Table 3.
Odds ratios (ORs) and 95% confidence intervals (95% CIs) for the association between dynamic foot function and foot pain in the men and women of the Framingham Foot Study (2002–2008), adjusted for age and weight.
|
|
||||
|---|---|---|---|---|
| Men | Women | |||
|
| ||||
| OR (95% CI) | P | OR (95% CI) | P | |
| Generalized foot pain | ||||
| Supinated vs. normal | 1.09 (0.87 – 1.37) | 0.458 | 0.93 (0.78 – 1.10) | 0.396 |
| Pronated vs. normal | 1.28 (1.04 – 1.56) | 0.018 | 1.15 (0.98 – 1.36) | 0.089 |
| Toe pain | ||||
| Supinated vs. normal | 0.99 (0.72 – 1.37) | 0.970 | 1.14 (0.92 – 1.4) | 0.226 |
| Pronated vs. normal | 1.30 (0.99 – 1.71) | 0.063 | 0.97 (0.76 – 1.23) | 0.780 |
| Ball of foot pain | ||||
| Supinated vs. normal | 0.86 (0.57 – 1.32) | 0.494 | 1.06 (0.84 – 1.34) | 0.613 |
| Pronated vs. normal | 1.05 (0.74 – 1.49) | 0.790 | 1.04 (0.82 – 1.32) | 0.758 |
| Forefoot pain | ||||
| Supinated vs. normal | 0.89 (0.6 – 1.34) | 0.579 | 0.90 (0.71 – 1.14) | 0.382 |
| Pronated vs. normal | 1.26 (0.9 – 1.78) | 0.178 | 1.06 (0.84 – 1.32) | 0.633 |
| Arch pain | ||||
| Supinated vs. normal | 1.28 (0.96 – 1.72) | 0.095 | 1.03 (0.81 – 1.32) | 0.800 |
| Pronated vs. normal | 1.26 (0.94 – 1.67) | 0.120 | 1.15 (0.91 – 1.45) | 0.243 |
| Heel pain | ||||
| Supinated vs. normal | 1.18 (0.83 – 1.68) | 0.349 | 0.90 (0.68 – 1.19) | 0.460 |
| Pronated vs. normal | 1.54 (1.04 – 2.27) | 0.030 | 1.22 (0.96 – 1.55) | 0.099 |
| Hindfoot pain | ||||
| Supinated vs. normal | 1.24 (0.89 – 1.74) | 0.203 | 0.74 (0.55 – 1.00) | 0.048 |
| Pronated vs. normal | 1.29 (0.92 – 1.82) | 0.140 | 0.88 (0.67 – 1.15) | 0.341 |
DISCUSSION
The objective of this study was to examine associations of foot posture and foot function to foot pain using objective biomechanical measurements in participants of the population-based Framingham Foot Study. Our findings indicate that both planus foot posture and pronated foot function are associated with foot pain, however these associations vary according to the location of foot pain and by sex. Specifically, planus foot posture was found to be associated with arch pain in men, and pronated foot function was significantly associated with generalized foot pain and heel pain in men. Contrary to our initial hypotheses, neither cavus foot posture nor supinated foot function was significantly associated with an increased likelihood of generalized or site-specific foot pain. In fact, cavus foot type was found to be associated with a decreased likelihood of ball of foot pain and arch pain in women, and supinated foot function was found to be associated with decreased likelihood of hindfoot pain in women.
Pes planus has long been considered to be a postural variation that increases the likelihood of developing foot problems (34). Individuals with “flat feet” have historically been disqualified from military service on this basis (35), although subsequent studies have questioned the validity of this regulation based on prospective observations of a lower risk of injury in army trainees with flat feet (36). Nevertheless, our observation of a significant association between planus foot posture and arch pain in men is consistent with previous studies in civilian populations that have reported this foot type to be associated with metatarsal stress fractures (37), tibialis posterior tendinopathy (13) and plantar heel pain (15). As other population-based studies evaluated this association using self-reported foot posture (7, 21), it is difficult to directly compare our findings. However, the Cheshire Foot Pain and Disability Survey also reported an association between planus foot posture and foot pain after adjusting for age and sex (7).
A novel aspect of our study is that we also included a measure of dynamic foot function – the center of pressure excursion index – which provides an indication of dynamic medial-lateral load distribution under the foot when walking (33). Using this measure, pronated foot function was found to be significantly associated with generalized foot pain and heel pain in men. No previous studies have been conducted exploring the association between this measure of foot function and foot symptoms. However, kinematic analysis has shown that runners with plantar heel pain exhibit greater rearfoot eversion (38) – a component of foot pronation that may be reflected in the center of pressure excursion index. The underlying mechanism linking dynamic foot pronation to foot pain remains unclear, although cadaver studies have shown that simulating a flat foot results in increased plantar fascia strain (39), increased talo-navicular joint motion (40), increased dorsal compressive forces in the midfoot (41) and reduced gliding ability of the tibialis posterior tendon (42) – factors that could potentially lead to tissue damage and subsequent foot symptoms.
Sex differences in the association of foot posture and foot function to foot pain were evident in this study. The reasons for these different patterns are unclear, although sex differences in foot posture, prevalence of foot disorders, pain reporting, occupation and footwear could all potentially play a role. In particular, footwear is likely to contribute to this difference, given that women are more likely to wear ill-fitting footwear than men and that such footwear has been associated with forefoot disorders (such as hallux valgus and lesser toe deformity) and foot pain (43). Despite this variation in risk profiles between men and women, the association was consistently in the direction of planus foot posture and pronated foot function increasing the likelihood of foot symptoms, and cavus foot type and supinated foot function decreasing the likelihood of foot symptoms. The apparent protective effect of cavus foot type and supinated foot function was unexpected, as previous studies have reported this foot type to be predisposed to exercise-related lower limb overuse injuries in athletes (14, 36) and foot pain in older people (44). There are several possible reasons for this discrepancy, including differences in sample characteristics, foot posture assessment techniques and cut-points used to define foot type categories.
The findings we report here need to be interpreted in the context of several study design limitations. First, we focused on foot symptoms, not specific diagnoses, so we cannot infer a link between foot posture, function and specific foot disorders. Second, in the absence of any established criteria, we used quintiles to determine the cut-points defining the three foot posture and function categories, which assumes that 60% of participants have “normal” feet and that the distribution of “abnormal” feet is symmetrical, i.e. 20% of the population has planus/pronated feet and 20% has cavus/supinated feet. While this approach is epidemiologically sound, it may not reflect clinical observations, which suggest that planus/pronated feet are more common than cavus/supinated feet. Nevertheless, since standard cut-points do not yet exist, this distribution based approach is reasonable, especially when using large samples. Third, while the center of pressure excursion index has been shown to discriminate between clinically-determined planus and rectus foot types (33) and individuals with and without posterior tibial tendon dysfunction (45), it has yet to be validated against a multi-segment kinematic foot model. Therefore, whether a pronated foot defined using this measure also demonstrates greater rearfoot eversion, sagittal plane midfoot motion or forefoot abduction is yet to be determined, and it is possible that other factors (such as medio-lateral sway) also influence this variable. Fourth, although our findings suggest that the degree of planus-cavus and pronation-supination of the foot are associated with foot pain, we acknowledge that there are many other biomechanical, psychosocial and occupational factors that may also contribute. Fifth, it is possible that foot pain may result in altered gait patterns and that this effect may be influenced by duration of foot pain and/or whether foot pain is unilateral or bilateral, however our analysis did not allow for these factors to be explored. Sixth, the Framingham population is relatively older and largely Caucasian. Given that there are significant differences in foot posture according to age (46) and between Caucasians, Hispanics and African Americans (47) different patterns of association may be evident in more diverse populations. Finally, the key limitation of all cross-sectional studies is the inability to confidently infer causation, although we consider reverse causation (i.e. foot pain resulting in more pronated foot posture and function) to be unlikely.
In summary, this is the first population-based investigation to examine the associations of foot posture and function to foot pain using objective biomechanical measurements, and provides evidence of an association between planus foot posture, pronated foot function and foot symptoms. As foot function is modifiable with footwear modifications and orthoses, such interventions could potentially play a role in both the treatment and prevention of foot pain.
SIGNIFICANCE AND INNOVATIONS.
This is the first population-based investigation to examine the associations of foot posture and function to foot pain using objective biomechanical measurements.
Planus foot posture and pronated foot function are associated with foot pain.
Interventions which modify foot function may play a role in both the treatment and prevention of foot pain.
Acknowledgments
Funding: National Institute of Arthritis and Musculoskeletal and Skin Diseases and National Institute on Aging (AR047853), National Heart, Lung and Blood Institute’s Framingham Heart Study (Contract No. N01-HC-25195)
The authors thank the Framingham Foot Study research team and study participants for the contribution of their time, effort, and dedication. We also thank Thomas Hagedorn (Institute for Aging Research, Hebrew SeniorLife, Boston, Massachusetts), Jocelyn Hafer and Mark Lenoff (Hospital for Special Surgery, New York City, New York) for their work on processing foot pressure scans and obtaining foot function and foot posture data, and Dr. Virginia Casey for providing valuable feedback and project management. Prof Menz is a National Health and Medical Research Council of Australia Senior Research Fellow (ID: 1020925) and was supported by an Australian-American Fulbright Commission Senior Scholarship at the time this work was undertaken.
Footnotes
AUTHOR CONTRIBUTIONS
All authors were involved in drafting the article or revising it critically for important intellectual content, and all authors approved the final version submitted for publication. Dr Hannan and Ms Dufour had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Study conception and design. Menz, Dufour, Hillstrom, Hannan.
Acquisition of data. Dufour, Hillstrom, Hannan.
Analysis and interpretation of data. Menz, Dufour, Riskowski, Hillstrom, Hannan.
References
- 1.Thomas MJ, Roddy E, Zhang W, Menz HB, Hannan MT, Peat GM. The population prevalence of foot and ankle pain in middle and old age: A systematic review. Pain. 2011;152:2870–2880. doi: 10.1016/j.pain.2011.09.019. [DOI] [PubMed] [Google Scholar]
- 2.Hill CL, Gill T, Menz HB, Taylor AW. Prevalence and correlates of foot pain in a population-based study: the North West Adelaide Health Study. J Foot Ankle Res. 2008;1:2. doi: 10.1186/1757-1146-1-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Menz HB, Jordan KP, Roddy E, Croft PR. Characteristics of primary care consultations for musculoskeletal foot and ankle problems in the UK. Rheumatology. 2010;49:1391–1398. doi: 10.1093/rheumatology/keq092. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Menz HB, Gilheany MF, Landorf KB. Foot and ankle surgery in Australia: a descriptive analysis of the Medicare Benefits Schedule database, 1997–2006. J Foot Ankle Res. 2008;1:10. doi: 10.1186/1757-1146-1-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Benvenuti F, Ferrucci L, Guralnik JM, Gangemi S, Baroni A. Foot pain and disability in older persons: an epidemiologic survey. J Am Geriatr Soc. 1995;43:479–484. doi: 10.1111/j.1532-5415.1995.tb06092.x. [DOI] [PubMed] [Google Scholar]
- 6.Gorter KJ, Kuyvenhoven MM, deMelker RA. Nontraumatic foot complaints in older people. A population-based survey of risk factors, mobility, and well-being. J Am Podiatr Med Assoc. 2000;90:397–402. doi: 10.7547/87507315-90-8-397. [DOI] [PubMed] [Google Scholar]
- 7.Garrow AP, Silman AJ, Macfarlane GJ. The Cheshire Foot Pain and Disability Survey: a population survey assessing prevalence and associations. Pain. 2004;110:378–384. doi: 10.1016/j.pain.2004.04.019. [DOI] [PubMed] [Google Scholar]
- 8.Leveille SG, Guralnik JM, Ferrucci L, Hirsch R, Simonsick E, Hochberg MC. Foot pain and disability in older women. Am J Epidemiol. 1998;148:657–665. doi: 10.1093/aje/148.7.657. [DOI] [PubMed] [Google Scholar]
- 9.Menz HB, Barr EL, Brown WJ. Predictors and persistence of foot problems in women aged 70 years and over: A prospective study. Maturitas. 2011;68:83–87. doi: 10.1016/j.maturitas.2010.08.010. [DOI] [PubMed] [Google Scholar]
- 10.McPoil TG, Hunt GC. Evaluation and management of foot and ankle disorders: present problems and future directions. J Orthop Sports Phys Ther. 1995;21:381–388. doi: 10.2519/jospt.1995.21.6.381. [DOI] [PubMed] [Google Scholar]
- 11.Razeghi M, Batt ME. Foot type classification: a critical review of current methods. Gait and Posture. 2002;15:282–291. doi: 10.1016/s0966-6362(01)00151-5. [DOI] [PubMed] [Google Scholar]
- 12.Kaufman KR, Brodine SK, Shaffer RA, Johnson CW, Cullison TR. The effect of foot structure and range of motion on musculoskeletal overuse injuries. Am J Sports Med. 1999;27:585–593. doi: 10.1177/03635465990270050701. [DOI] [PubMed] [Google Scholar]
- 13.Williams DS, 3rd, McClay IS, Hamill J. Arch structure and injury patterns in runners. Clin Biomech. 2001;16:341–7. doi: 10.1016/s0268-0033(01)00005-5. [DOI] [PubMed] [Google Scholar]
- 14.Burns J, Keenan A-M, Redmond A. Foot type and overuse injury in triathletes. J Am Podiatr Med Assoc. 2005;95:235–241. doi: 10.7547/0950235. [DOI] [PubMed] [Google Scholar]
- 15.Irving DB, Cook JL, Young MA, Menz HB. Obesity and pronated foot type may increase the risk of chronic plantar heel pain: a matched case-control study. BMC Musculoskelet Disord. 2007;8:41. doi: 10.1186/1471-2474-8-41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Gross KD, Felson DT, Niu J, Hunter DJ, Guermazi A, Roemer FW, et al. Association of flat feet with knee pain and cartilage damage in older adults. Arthritis Care Res. 2011;63:937–944. doi: 10.1002/acr.20431. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Wen DY, Puffer JC, Schmalzried TP. Lower extremity alignment and risk of overuse injuries in runners. Med Sci Sports Exerc. 1997;29:1291–1298. doi: 10.1097/00005768-199710000-00003. [DOI] [PubMed] [Google Scholar]
- 18.Michelson JD, Durant DM, McFarland E. The injury risk associated with pes planus in athletes. Foot Ankle Int. 2002;23:629–633. doi: 10.1177/107110070202300708. [DOI] [PubMed] [Google Scholar]
- 19.Nakhaee Z, Rahimi A, Abaee M, Rezasoltani A, Kalantari KK. The relationship between the height of the medial longitudinal arch (MLA) and the ankle and knee injuries in professional runners. Foot. 2008;18:84–90. doi: 10.1016/j.foot.2008.01.004. [DOI] [PubMed] [Google Scholar]
- 20.Shibuya N, Jupiter DC, Ciliberti LJ, VanBuren V, LaFontaine J. Characteristics of adult flatfoot in the United States. J Foot Ankle Surg. 2010;49:363–368. doi: 10.1053/j.jfas.2010.04.001. [DOI] [PubMed] [Google Scholar]
- 21.Molgaard C, Lundbye-Christensen S, Simonsen O. High prevalence of foot problems in the Danish population: a survey of causes and associations. Foot. 2010;20:7–11. doi: 10.1016/j.foot.2010.03.002. [DOI] [PubMed] [Google Scholar]
- 22.Dufour AB, Broe KE, Nguyen US, Gagnon DR, Hillstrom HJ, Walker AH, et al. Foot pain: is current or past shoewear a factor? Arthritis Rheum. 2009;61:1352–8. doi: 10.1002/art.24733. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Dawber T, Meadors G, Moore F. Epidemiological approaches to heart disease: the Framingham Study. Am J Public Health Nations Health. 1951;41:279–281. doi: 10.2105/ajph.41.3.279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Feinleib M, Kannel W, Garrison R, McNamara P, Castelli W. The Framingham Offspring Study: design and preliminary data. Prev Med. 1975;4:518–525. doi: 10.1016/0091-7435(75)90037-7. [DOI] [PubMed] [Google Scholar]
- 25.Zammit GV, Menz HB, Munteanu SE. Reliability of the TekScan MatScan(R) system for the measurement of plantar forces and pressures during barefoot level walking in healthy adults. J Foot Ankle Res. 2010;3:11. doi: 10.1186/1757-1146-3-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Bryant A, Singer K, Tinley P. Comparison of the reliability of plantar pressure measurements using the two-step and midgait methods of data collection. Foot Ankle Int. 1999;20:646–650. doi: 10.1177/107110079902001006. [DOI] [PubMed] [Google Scholar]
- 27.Cavanagh PR, Rodgers MM. The arch index: a useful measure from footprints. J Biomech. 1987;20:547–551. doi: 10.1016/0021-9290(87)90255-7. [DOI] [PubMed] [Google Scholar]
- 28.McCrory JL, Young MJ, Boulton AJM, Cavanagh PR. Arch index as a predictor of arch height. Foot. 1997;7:79–81. [Google Scholar]
- 29.Menz HB, Munteanu SE. Validity of 3 clinical techniques for the measurement of static foot posture in older people. J Orthop Sports Phys Ther. 2005;35:479–486. doi: 10.2519/jospt.2005.35.8.479. [DOI] [PubMed] [Google Scholar]
- 30.Kanatli U, Yetkin H, Cila E. Footprint and radiographic analysis of the feet. J Pediatr Orthop. 2001;21:225–228. [PubMed] [Google Scholar]
- 31.Yalcin N, Esen E, Kanatli U, Yetkin H. Evaluation of the medial longitudinal arch: a comparison between the dynamic plantar pressure measurement system and radiographic analysis. Acta Orthop Traumatol Turc. 2010;44:241–245. doi: 10.3944/AOTT.2010.2233. [DOI] [PubMed] [Google Scholar]
- 32.Murley GS, Menz HB, Landorf KB. A protocol for classifying normal- and flat-arched foot posture for research studies using clinical and radiographic measurements. J Foot Ankle Res. 2009;2:22. doi: 10.1186/1757-1146-2-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Song J, Hillstrom HJ, Secord D, Levitt J. Foot type biomechanics: a comparison of planus and rectus foot types. J Am Podiatr Med Assoc. 1996;86:16–23. doi: 10.7547/87507315-86-1-16. [DOI] [PubMed] [Google Scholar]
- 34.Humphrey GM. A lecture on flat-foot and the construction of the plantar arch. Lancet. 1886;127:529–531. [Google Scholar]
- 35.Ilfeld FW. Pes planus military significance and treatment with simple arch support. JAMA. 1944;124:281–283. [Google Scholar]
- 36.Cowan DN, Jones BH, Robinson JR. Foot morphologic characteristics and risk of exercise-related injury. Arch Fam Med. 1993;2:773–777. doi: 10.1001/archfami.2.7.773. [DOI] [PubMed] [Google Scholar]
- 37.Simkin A, Leichter I, Giladi M, Stein M, Milgrom C. Combined effect of foot arch structure and an orthotic device on stress fractures. Foot Ankle. 1989;10:25–29. doi: 10.1177/107110078901000105. [DOI] [PubMed] [Google Scholar]
- 38.Messier SP, Pittala KA. Etiologic factors associated with selected running injuries. Med Sci Sports Exerc. 1988;20:501–505. [PubMed] [Google Scholar]
- 39.Kogler GF, Solomonidis SE, Paul JP. In vitro method for quantifying the effectiveness of the longitudinal arch support mechanism of a foot orthosis. Clin Biomech. 1995;10:245–252. doi: 10.1016/0268-0033(95)99802-9. [DOI] [PubMed] [Google Scholar]
- 40.Kitaoka HB, Luo ZP, An KN. Mechanical behavior of the foot and ankle after plantar fascia release in the unstable foot. Foot Ankle Int. 1997;18:8–15. doi: 10.1177/107110079701800103. [DOI] [PubMed] [Google Scholar]
- 41.Kitaoka HB, Luo ZP, An KN. Contact features of the talonavicular joint of the foot. Clin Orthop Relat Res. 1996;325:290–295. doi: 10.1097/00003086-199604000-00035. [DOI] [PubMed] [Google Scholar]
- 42.Fujii T, Uchiyama E, Kitaoka HB, Luo ZP, Zhao KD, An KN. The influence of flatfoot deformity on the gliding resistance of tendons about the ankle. Foot Ankle Int. 2009;30:1107–1110. doi: 10.3113/FAI.2009.1107. [DOI] [PubMed] [Google Scholar]
- 43.Menz HB, Morris ME. Footwear characteristics and foot problems in older people. Gerontology. 2005;51:346–351. doi: 10.1159/000086373. [DOI] [PubMed] [Google Scholar]
- 44.Badlissi F, Dunn JE, Link CL, Keysor JJ, McKinlay JB, Felson DT. Foot musculoskeletal disorders, pain, and foot-related functional limitation in older persons. J Am Geriatr Soc. 2005;53:1029–1033. doi: 10.1111/j.1532-5415.2005.53315.x. [DOI] [PubMed] [Google Scholar]
- 45.Ringleb SI, Kavros SJ, Kotajarvi BR, Hansen DK, Kitaoka HB, Kaufman KR. Changes in gait associated with acute stage II posterior tibial tendon dysfunction. Gait Posture. 2007;25:555–564. doi: 10.1016/j.gaitpost.2006.06.008. [DOI] [PubMed] [Google Scholar]
- 46.Redmond AC, Crane YZ, Menz HB. Normative values for the Foot Posture Index. J Foot Ankle Res. 2008;1:6. doi: 10.1186/1757-1146-1-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Castro-Aragon O, Vallurupalli S, Warner M, Panchbhavi V, Trevino S. Ethnic radiographic foot differences. Foot Ankle Int. 2009;30:57–61. doi: 10.3113/FAI.2009.0057. [DOI] [PubMed] [Google Scholar]