

Abstract
Accessory breast tissue is an uncommon condition which occurs in 0.4–6% of women. It is mostly located in the axilla where it can cause diagnostic difficulty, especially if it is unilateral and large. Usually it is bilateral and presents as an asymptomatic mass during pregnancy or lactation. The diagnosis of ectopic breast tissue is important as it can undergo the same pathological changes that occur in a normal breast, such as mastitis, fibrocystic disease and carcinoma. We present a case of a large right-sided accessory breast in a 32-year-old woman that was clinically diagnosed as pedunculated lipoma. However, subsequent histopathological examination proved it to be an accessory breast tissue with lactational changes.
Background
Accessory breast tissue is an uncommon entity mostly located in the axilla. It undergoes all the cyclical changes and can develop any of the complications of the normal breast. Sometimes it poses a diagnostic challenge, especially when it is unilateral and large.
Case presentation
A 32-year-old woman presented with a large pendulous mass of 3 years’ duration in her right axilla. Initially it was a small swelling of 2×2 cm. It gradually grew larger during pregnancy with a sudden, rapid increase in size after delivery. It was occasionally painful and restricted arm movement.
Physical examination revealed a 15×12×11 cm pedunculated mass in the right axilla which was mobile, non-tender and firm in consistency. Skin over the swelling was hyperpigmented and free from underlying structures. There was no nipple or areola over the mass. The bilateral breasts were normal without any palpable axillary lymphadenopathy (figure 1).
Figure 1.

Accessory breast tissue in the right axilla.
A clinical diagnosis of the pedunculated lipoma was made and the patient was scheduled for excisional biopsy.
Investigations
All routine investigations were within normal limits. No radiological investigations were carried out. Fine-needle aspiration cytology (FNAC) was carried out and revealed a greasy material on aspiration. Smears were paucicellular, consisting of only a few scattered adipocytes.
Differential diagnosis
A differential diagnosis of accessory axillary breast or pedunculated lipoma was made.
Treatment
An excisional biopsy was performed under general anaesthesia and the tissue was sent for histopathology.
Grossly on sectioning, a milky white fluid oozed out (figure 2). Microscopic examination showed mostly mature adipose tissue interspersed with breast tissue having lobular architecture. Numerous ducts and acini were seen lined by ductular epithelial cells showing secretory activity. Sheets of foamy cells and a large area filled with pale eosinophilic secretion were also seen. Thus, histopathological features were consistent with the accessory breast tissue showing lactational changes (figures 3 and 4).
Figure 2.
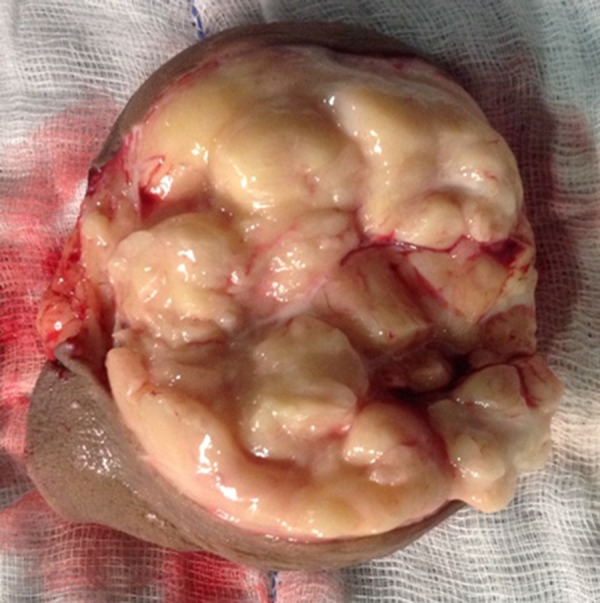
Gross specimen showing lobulated surface that on cutting exuded milky white fluid.
Figure 3.
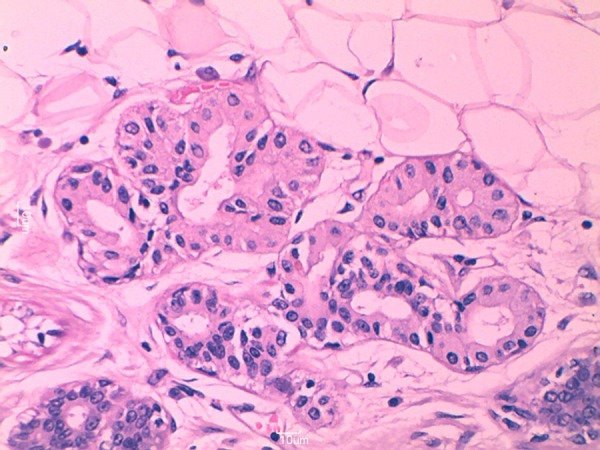
Microphotograph showing breast acini lined by cells showing secretory activity admixed with adipose tissue (H&E stain, 40×).
Figure 4.
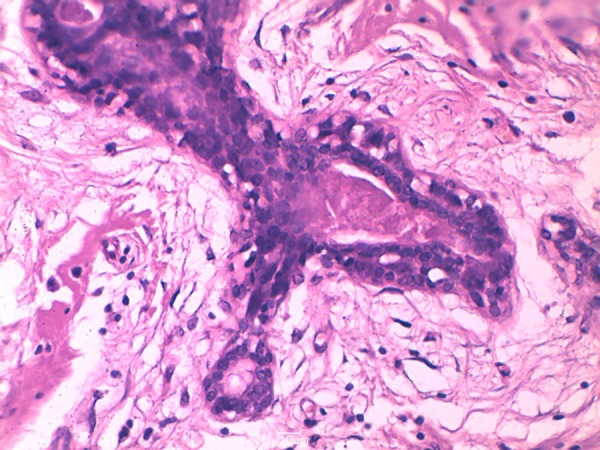
High-power view showing duct with secretion in the lumen (H&E stain, 40×).
Outcome and follow-up
The postoperative period remained uneventful and the patient was discharged on the second postoperative day. Sutures were removed on the eighth postoperative day in the outpatient department. The patient is doing fine with no recurrence or complications.
Discussion
Ectopic breast tissue occurs due to failure of resolution of the embryonic mammary ridge (milk line), which is an ectodermal thickening from axilla to groin bilaterally. It is the term used for both supernumerary and aberrant breast tissue, which are two distinct entities.1 Supernumerary breasts have nipples, areolae or both with varied composition of glandular tissue.2 They mostly present along the mammary ridge but may also occur on the cheek, neck, shoulder, thigh or buttock.3 Pathological findings in a supernumerary breast usually comprise of an organised ductal system communicating with the overlying skin, and usually respond to all the physiological changes of the reproductive cycle.4 5
An aberrant or accessory breast tissue is a diverticular form of the breast during the fetal period which subsequently loses all connection with the ipsilateral breast. Unlike supernumerary breasts, it has no organised secretory system and does not communicate with the overlying skin. The most common location for the aberrant breast tissue is the axilla while other uncommon sites are infraclavicular, subscapular, epigastric and vulva.5 Aberrant breast tissue becomes symptomatic during menarche, pregnancy and lactation and responds to fluctuating hormonal levels.6 Our case fits in the category of accessory or aberrant breast tissue as it was without any nipple areola complex and its size increased during lactation.
The incidence of the accessory breast ranges from 0.4% to 6%.7 Mostly it is bilateral and presents as an asymptomatic mass during pregnancy or lactation. It may also present with pain, restriction of arm movements and cosmetic problems.7 Diagnosis of ectopic breast tissue is important as it can undergo the same pathological events that occur in the normal breast such as mastitis, fibrocystic disease and carcinoma.7 8
Mass-like density, the same as that of the normal breast parenchyma, is seen both on ultrasound and mammography.9 FNAC is a useful tool to distinguish it from other masses like lipoma or lymph nodes. In the present case FNAC was inconclusive. The patient was planned for excisional biopsy for cosmetic reasons.
The management of ectopic breast is mainly surgical, though small size asymptomatic ectopic breasts may be managed conservatively.7 Excision is recommended in large size tissue for cosmetic reasons and to avoid any future complications.10
Learning points.
Accessory breast tissue is not a very common entity and may sometimes pose a diagnostic challenge for the treating physician.
Diagnosis of accessory breast tissue is important as it can undergo the same pathological changes that occur in the normal breast, such as mastitis, fibrocystic disease and even carcinoma.
Surgical management is recommended for cosmetic reasons as well as to avoid any future complications.
Footnotes
Contributors: MH conceived of the concept, designed and drafted the article. AB was involved in drafting the article. SK proofread the article and contributed to the photographs. FH proofread the article.
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Zafer T, Burhan K, Metin A, et al. Primary infiltrating ductal carcinoma arising in aberrant breast tissue of the axilla: a rare entity. Report of a case. Tumori 2008;94:577–83 [DOI] [PubMed] [Google Scholar]
- 2.Evans DM, Guyton DP. Carcinoma of the axillary breast. J Surg Oncol 1995;59:190–5 [DOI] [PubMed] [Google Scholar]
- 3.Cheong GH, Lee BC, Lee KS. Carcinoma of the axillary breast. Yonsei Med J 1999;40:290–3 [DOI] [PubMed] [Google Scholar]
- 4.Petrek J, Rosen PP, Robbins GF. Carcinoma of aberrant breast tissue. Clin Bull 1980;10:13–15 [PubMed] [Google Scholar]
- 5.Marshall MB, Moynihan JJ, Frost A, et al. Ectopic breast cancer: case report and literature review. Surg Oncol 1994;3:295–304 [DOI] [PubMed] [Google Scholar]
- 6.Loukas M, Clarke P, Tubbs RS. Accessory breasts: a historical and current perspective. Am Surg 2007;73:525–8 [PubMed] [Google Scholar]
- 7.Down S, Barr L, Baildam AD, et al. Management of accessory breast tissue in axilla. Br J Surg 2003;90:1213–14 [DOI] [PubMed] [Google Scholar]
- 8.Markopoulos C, Kouskos E, Kontzoglou K, et al. Breast cancer in ectopic breast tissue. Eur J Gynaecol Oncol 2001;22:157–9 [PubMed] [Google Scholar]
- 9.Kim HS, Cha ES, Kim HH, et al. Spectrum of sonographic findings in superficial breast masses. J Ultrasound Med 2005;24:663–80 [DOI] [PubMed] [Google Scholar]
- 10.Lesavoy MA, Gomez-Gracia A, Nejdl R, et al. Axillary breast tissue: clinical presentation and surgical treatment. Ann Plast Surg 1995; 35:356–60 [PubMed] [Google Scholar]