

Abstract
Background
The six-minute walk test has been widely used in people with chronic cardiopulmonary disorders as an outcome assessment with regards to therapeutic or prognostic determinants. This study was undertaken to determine the six-minute walk distance (6MWD) in a sample of healthy Koreans and to create a reference equation. We also compared the 6MWD of our cohort with previously published equations.
Methods
Two hundred fifty-nine healthy subjects (95 males) aged 22-59 years performed two walking tests using a standardized protocol. 6MWD was defined as the greatest distance achieved from the two tests. The effect of anthropometrics on the 6MWD was also investigated.
Results
The average 6MWD was 598.5±57.92 m, with significantly longer distances by males (628.9±59.51 m) than females (580.9±47.80 m) (p<0.001). Age, height, weight, and body mass index were significantly correlated with 6MWD in univariate analysis. Stepwise multiple regression showed height to be single independent predictor of 6MWD (r2=0.205, p<0.001). The reference equations derived in Caucasian and North African populations tend to overestimate the distance walked by Korean subjects, while Asian equations underestimate it.
Conclusion
The average 6MWD in these Korean populations was 600 m. The regression equation revealed that individual's height was the most significant predictor of distance, explaining 20.5% of the distance variance.
Keywords: Exercise Tolerance, Exercise Test, Physical Endurance, Reference Values, Healthy Volunteers
Introduction
The measurement of exercise capacity is frequently used to assist clinicians in evaluating functional capacity, assessing prognosis, and evaluating response to treatment in patients with various cardiopulmonary diseases1,2,3. Maximum oxygen consumption obtained via incremental laboratory tests performed in a cycle ergometer or treadmill is more useful in assessing exercise capacity4,5,6; however, it is not easily available because of the high cost of equipment and the complexity of test procedures.
The six-minute walk test (6MWT) is a simpler and less expensive tool, and patients are more willing to tolerate it as a method of assessing the cardiorespiratory fitness7. It provides a valid assessment of functional performance in persons with chronic cardiopulmonary disorders and has been broadly used in clinical settings. A variety of reference equations predicting six-minute walk distance (6MWD) in healthy subjects has been reported8,9,10,11,12, but most studies have been undertaken in white populations. These equations may not be suitable for predicting 6MWD in Asian populations, because the equations overestimate the distance13,14. Although some clinical studies using 6MWD as an outcome assessment have been reported in this country15,16,17,18, so far no study exists looking at 6MWD reference equations for healthy subjects.
The aims of present study were the following: 1) to determine 6MWD in a healthy sample of Koreans aged between 22 and 59 years, 2) to identify demographic and anthropometric factors contributing to 6MWD and establish a reference equation, and 3) to examine the differences between walking distances observed in our cohort and previously published equations.
Materials and Methods
1. Healthy subjects
Two hundred fifty-nine healthy Korean volunteers between the ages of 22 and 59 years were randomly recruited to participate in this descriptive, prospective, cross-sectional study. Subjects were medical students, hospital workers, visitors, and employees of a local private company. The study was conducted according to the Declaration of Helsinki and Good Clinical Practice guidelines. Written, informed consent was obtained from each healthy subject before participation in the study, and the study protocol was approved by local hospital institutional review board (approval number: DFH09OT057). Data from each subject included age, sex, height, weight, smoking history, medication use, medical history, physical examination, and spirometry. Any of the following is regarded as a criterion for exclusion from the study: medical histories that were indicative of metabolic, cardiovascular, or pulmonary disease, current or ex-smokers with a smoking history of at least 10 pack-years, upper respiratory tract infections within the last 4 weeks, conditions that could affect walking, resting blood pressures higher than 140/90 mm Hg, heart rates higher than 100 beats per minute, body mass index (BMI) greater than 35, or evidence of ventilatory impairment as measured by spirometry (i.e., forced expiratory volume in one second (FEV1)/forced vital capacity (FVC) values lower than 70%, of normal predicted value).
2. Six-minute walk tests
Two six-minute walks were performed for all healthy subjects on the same day, with 30-minute rests in between walks. The 6MWT protocol used was based on published guidelines7, and 30 m-long hospital corridor with marks at 3 m intervals was used. Each 6MWT was supervised by a medical doctor, who did not walk alongside the healthy subject. A standard explanation was provided just before the first 6MWT: "Walk as quickly as you can along the corridor for 6 minutes to cover as much ground as possible. You may stop if you have to, but continue again as soon as you are able. During the test, oxygen saturation and heart rate were measured by wearable transcutaneous pulse oximetry (Nonin WristOx 3100; Nonin, Plymouth, MN, USA). Subjects were allowed to stop if they developed symptoms of dyspnea, chest pain, leg cramps, or dizziness, but were encouraged to continue walking as soon as they could. At the ends of each minute subjects were given feedback on the elapsed time and standardized encouragement in the form of statements such as "you're doing well," and "do your best." Before and after each 6MWT, pulse rate, blood pressure, oxygen saturation, and Borg value were recorded. Subjects were asked to indicate their level of dyspnea perception using a modified 12-point Borg scale, wherein each score (i.e., ranging from 0 to 10) is illustrated by a printed figure. The maximum predicted heart rate (mHR) was calculated as 220 minus age.
3. Spirometry
Height and weight were measured using a calibrated scale, and BMI for each subject was calculated before spirometry. Subjects were asked to perform at least three measures, and the largest value was recorded for analysis as recommended by the American Thoracic Society guidelines19.
4. Statistical analysis
All statistical analyses were performed using the PASW version 18 (SPSS Inc., Chicago, IL, USA). The greatest distance covered in 6 minutes by each healthy subject was identified from among the two 6MWT trials performed and then used in the following analyses. A descriptive analysis was made to summarize the population's demographic and clinical parameters. Student's t-tests were used to compare female and male subjects. Pearson's univariate correlation coefficients (r) were computed to examine the association between subject characteristics and 6MWD. A stepwise linear regression model was used to determine if any of the above variables were independent predictors of 6MWD. The mean 6MWD measured of the subjects in our study was compared to the mean predicted 6MWD derived from the eight previously published equations8,9,10,11,12,13,14,20 according to each same age ranges. A p-value of <0.05 was considered significant for these analyses.
Results
1. Demographic, anthropometric, spirometric, and 6MWT data
Of the 278 subjects recruited for participation in this study, 19 were excluded because of smoking history of over 10 pack-years (n=13) and high blood pressure (n=6). Characteristics of the remaining 259 healthy subjects are summarized in Table 1. The study population was composed of 95 males and 164 females, with a mean age of 36.6±10.83 years, height 164.5±8.65 cm, weight 61.0±11.72 kg, BMI 22.4±2.85 kg/m2, and pre-bronchodilator FEV1 96.2±11.11% predicted. Significant difference was observed in age, height, weight, BMI, FVC (L), FEV1 (L), and FEV1 (% pred) between male and female subjects.
Table 1.
Characteristics of the study subjects
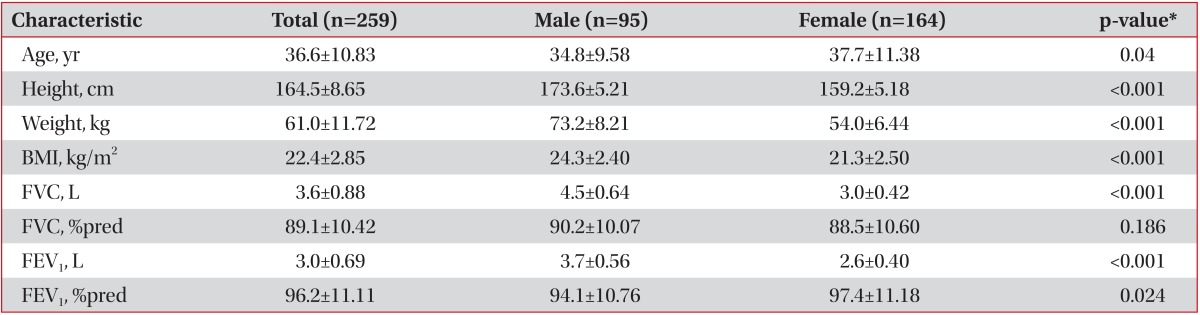
Values are expressed as mean±SD.
*p-value between male and female.
BMI: body mass index; FVC: forced vital capacity; FEV1: forced expiratory volume in one second.
The 6MWT data are shown in Table 2. The mean 6MWD was 598.5±57.92 m (range, 447-761 m) for the group total and was 628.9±59.51 m (range, 447-761 m) for male and 580.9±47.80 m (range, 454-720 m) for female, with significantly longer distances walked by males than females (p<0.001). Male and female subjects reached 60.7% and 64.4% of their maximum predicted heart rates, respectively, at the end of the test. The mean 6MWD of second walk was significantly longer than that of first walk (595.0±58.27 m vs. 578.3±55.03 m, p<0.001), suggesting a learning effect. We observed a small but significant difference between two groups with regards to resting heart rate, resting oxygen saturation, Borg values, and oxygen saturation measured at the end of the test. No clinically significant oxygen desaturation during 6MWT was observed.
Table 2.
6MWT measures of the study subjects
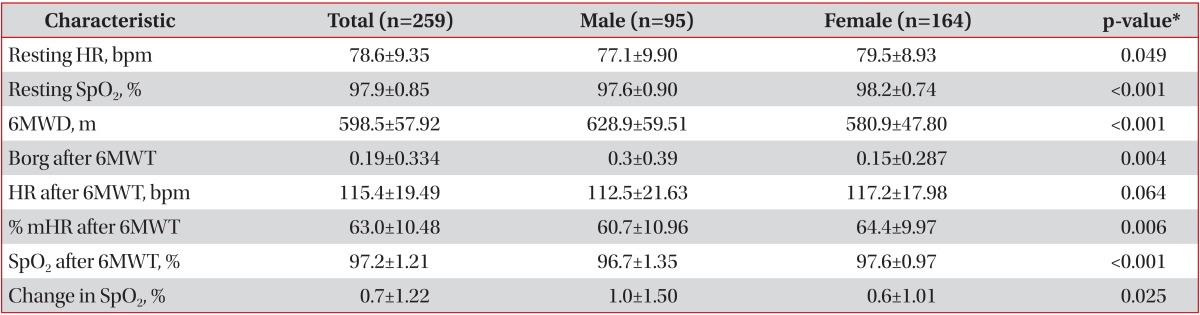
Values are expressed as mean±SD.
*p-value between male and female.
6MWT (D): 6 minute walking test (distance); HR: heart rate; SpO2: oxygen saturation; % mHR: percentage of the predicted maximum heart rate.
2. Univariate and multiple regression analysis
Univariate correlation coefficients between the 6MWD and subject variables are presented in Table 3. Significant correlations with age, height, weight, and BMI were observed in the group total (Figure 1). However, gender differences were observed. While age and height were significantly correlated with 6MWD in male subjects, there was no significantly correlated variable in female subjects. In the stepwise multiple regression analysis using age, height, weight, and sex in the group total, height was identified as a single independent contributing factor to 6MWD (p<0.001), and the model explained 20.5% of the variability in 6MWD. The regression equation for estimating 6MWD is as follows: 6MWD (m)=105.7+2.99×height (cm) (r2=0.205). In the group of 20-29 years, sex (p=0.005) and height (p=0.028) were significant independent predictors and together explained 42.4% of the variability in 6MWD. In the group of 30-39 years, height (p<0.001) was an independent predictor, and this model accounted for 23.9% of the total variance for the 6MWD. According to the gender, age (p<0.001) and height (p=0.014) were significant independent predictors in the group of male and together explained 30.5% of the variability in 6MWD. No significant independent demographic or anthropometric factors predicting the 6MWD in the group of female and of 40-59 years were observed (Table 4).
Table 3.
Univariate correlation coefficients for 6MWD

6MWD: six-minute walking distance; r-value: Pearson's correlation coefficient; BMI: body mass index.
Figure 1.

Relationships between six-minute walking distance (6MWD) and age (r=-0.219, p<0.001) (A), 6MWD and height (r=0.453, p<0.001) (B), and 6MWD and weight (r=0.355, p<0.001) (C). The linear regression line is superimposed, surrounded with the 95% confidence interval lines for the regression line.
Table 4.
Predicting model for 6MWD*
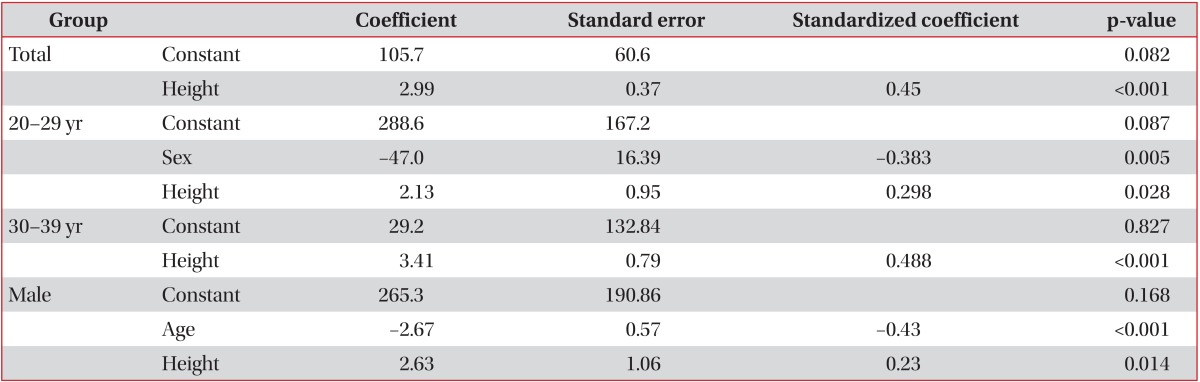
*Reference equations of six-minute walking distance (6MWD) are as follows.
Total: 6MWD (m)=105.7+2.99×height (cm); r2=0.205.
20-29 yr: 6MWD (m)=288.6-47.0×sex (male=0, female=1)+2.13×height (cm); r2=0.424.
30-39 yr: 6MWD (m)=29.2+3.41×height (cm); r2=0.239.
Male: 6MWD (m)=265.3-2.67×age (yr)+2.63×height (cm); r2=0.305.
There were no significant demographic or anthropometric variables predicting the 6MWD in the group of female and of 40-59 years.
3. Comparison with published regression equations
Comparisons between the 6MWD measured in our subjects and predicted 6MWD, with a match for the same age range, from the reference equations derived in Caucasian8,9,10,11,12, African20 and Asian13,14 populations are shown in Table 5. Walk distance for our cohort was overestimated by four out of six equations derived from Caucasian and African populations, including Troosters et al.9, who overestimated the distance walked by our subjects by 84.5±68.08 m (p<0.001), Camarri et al.10 by 101.2±54.41 m (p<0.001), Gibbons et al.11 by 113.4±58.60 m (p<0.001) and Ben Saad et al.20 by 70.4±92.63 m (p<0.001). However, walk distance was underestimated by two equations derived in Asian populations, Poh et al.14 by 24.0±51.96 m (p<0.001) and Alameri et al.13 by 140.6±52.40 m (p<0.001).
Table 5.
Measured and predicted 6MWD, for the same age range, from the equations derived in previous studies
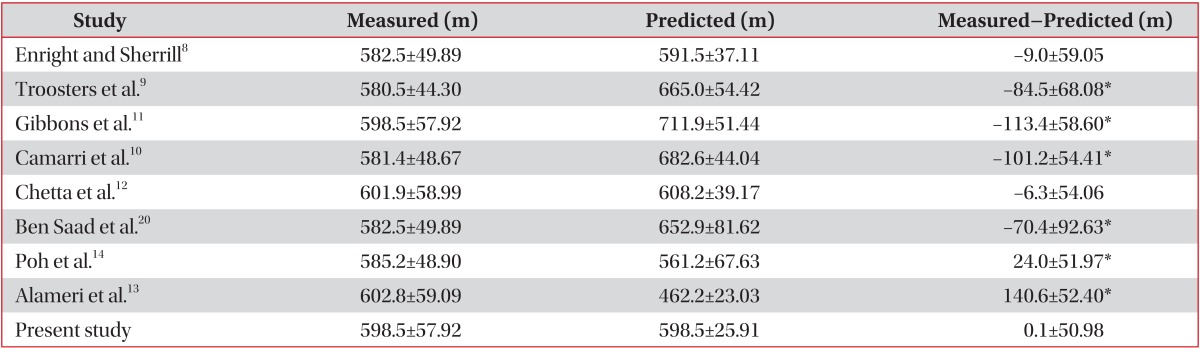
*p<0.05 by student t-test.
6MWD: six-minute walking distance.
Discussion
To our knowledge, this is the first study to predict 6MWD in healthy Korean populations. The average 6MWD in these Korean populations was 598.5±57.92 m. The regression equation revealed that height was the most significant predictor of distance, explaining 20.5% of the distance variance. The 6MWD in these populations showed a considerable variability, ranging 447-761 m, in line with previous studies9,10,12,14,20. However, the average 6MWD measured here was relatively shorter than those of Caucasian8,9,10,11 and North African studies20 and longer than those of Asian studies13,14. It is possible that this discrepancy reflects differences in how 6MWT protocol was conducted and differences in racial, demographic, and anthropometric factors of subjects recruited in each study. In addition, subjects' submaximal effort was also considered as a possibility. In this study, a 6MWT was performed twice and the better of the two tests was used for further analysis. In two studies9,20 consistent with our protocol, despite the fact that recruited subjects were relatively older than ours, their average 6MWD were longer than that of present study. Our subjects reached an average of 63±10% of their maximum predicted heart rates, while subjects in these studies reached an average of 77±15%, 79±13% of their mHRs, respectively. However, in the middle Asian study by Alameri et al.13, using single 6MWT protocol, the overall mean walking distance was 410±52 m, which was significantly shorter than those in our study. Despite possessing similar age ranges as those of our subjects, the male and female subjects in Alameri et al.'s study13 reached an average of 44% and 47% of their mHRs, respectively. This is natural in view of that there is a high prevalence of physical inactivity among Saudis21. In addition to a subject's level of daily physical activity, attitude or psychological factors may also influence the degree of submaximal effort22.
Several demographic and anthropometric factors can influence the 6MWT performance in healthy subjects, showing 34-78% of the variance in the 6MWD8,9,10,11,12,14,20. Among them, age, height, weight, and sex were the most common variables used to predict 6MWD. However, in our model, height was the only reliable predictor of distance, explaining 20.5% of the distance variance. This low variability is similar to that of recent study by Alameri et al.13; wherein twenty five percent of the variability of 6MWD was explained by age and height. Not surprisingly, a taller height is associated with a longer stride, which generates a longer distance8,9,14. In the univariate analysis of our series, age and height were significantly correlated with 6MWD in male subjects, but no significant variables were observed in female subjects. In the end, sex and age could not enter final model in the group total. However, sex was significant independent predictor in the younger age group. In the group of female and of 40-59 years, no significant independent demographic or anthropometric factors predicting the 6MWD were observed. As in the case of previous studies11,12, the different level of peripheral muscle conditioning or physical fitness of the participants in this study, particularly in female subjects, may be partly responsible for this, because most of the female subjects in their forties and fifties were hospital sanitation workers who were more physically active than younger subjects.
In present study, while the reference equations derived in Caucasian8,9,10,11,12 and North African20 populations tend to overestimate the distance walked by Korean subjects, two Asian equations13,14 underestimate it. The 6MWT has been widely used in clinical settings as an outcome assessment with regards to therapeutic or prognostic determinants. Clearly, these previously reported equations can provide misleading information when applied to Korean patients. It is therefore necessary to develop reference equations specific to Koreans.
This study was limited by several factors. First, our subjects consisted of middle-aged subjects. Therefore, the reference equation in the present study may predict 6MWD in Korean patients with cardio-respiratory dysfunction at a relatively young age. However, since most chronic obstructive pulmonary disease patients are older than the present cohort, there may be some controversy to apply this reference equation to wider populations. Second, the sample studied in present study included medical personnel, workers, medical students, and visitors at a local referral hospital and may not be representative of the entire Korean population. A well-organized nationwide study is needed to solve this problem. Third, the study did not attempt to evaluate the degree to which typical daily physical activity and psychological factors affected 6MWD.
In conclusion, the average 6MWD in these Korean populations was 600 m. The regression equation revealed that height was the most significant predictor of distance, explaining 20.5% of the distance variance.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Pauwels RA, Buist AS, Calverley PM, Jenkins CR, Hurd SS GOLD Scientific Committee. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop summary. Am J Respir Crit Care Med. 2001;163:1256–1276. doi: 10.1164/ajrccm.163.5.2101039. [DOI] [PubMed] [Google Scholar]
- 2.Ries AL, Bauldoff GS, Carlin BW, Casaburi R, Emery CF, Mahler DA, et al. Pulmonary rehabilitation: Joint ACCP/AACVPR evidence-based clinical practice guidelines. Chest. 2007;131(5 Suppl):4S–42S. doi: 10.1378/chest.06-2418. [DOI] [PubMed] [Google Scholar]
- 3.Nici L, Donner C, Wouters E, Zuwallack R, Ambrosino N, Bourbeau J, et al. American Thoracic Society/European Respiratory Society statement on pulmonary rehabilitation. Am J Respir Crit Care Med. 2006;173:1390–1413. doi: 10.1164/rccm.200508-1211ST. [DOI] [PubMed] [Google Scholar]
- 4.Bruce RA. Methods of exercise testing. Step test, bicycle, treadmill, isometrics. Am J Cardiol. 1974;33:715–720. doi: 10.1016/0002-9149(74)90211-2. [DOI] [PubMed] [Google Scholar]
- 5.Cox NJ, Hendriks JC, Binkhorst RA, Folgering HT, van Herwaarden CL. Reproducibility of incremental maximal cycle ergometer tests in patients with mild to moderate obstructive lung diseases. Lung. 1989;167:129–133. doi: 10.1007/BF02714939. [DOI] [PubMed] [Google Scholar]
- 6.ERS Task Force on Standardization of Clinical Exercise Testing; European Respiratory Society. Clinical exercise testing with reference to lung diseases: indications, standardization and interpretation strategies. Eur Respir J. 1997;10:2662–2689. doi: 10.1183/09031936.97.10112662. [DOI] [PubMed] [Google Scholar]
- 7.ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002;166:111–117. doi: 10.1164/ajrccm.166.1.at1102. [DOI] [PubMed] [Google Scholar]
- 8.Enright PL, Sherrill DL. Reference equations for the six-minute walk in healthy adults. Am J Respir Crit Care Med. 1998;158(5 Pt 1):1384–1387. doi: 10.1164/ajrccm.158.5.9710086. [DOI] [PubMed] [Google Scholar]
- 9.Troosters T, Gosselink R, Decramer M. Six minute walking distance in healthy elderly subjects. Eur Respir J. 1999;14:270–274. doi: 10.1034/j.1399-3003.1999.14b06.x. [DOI] [PubMed] [Google Scholar]
- 10.Camarri B, Eastwood PR, Cecins NM, Thompson PJ, Jenkins S. Six minute walk distance in healthy subjects aged 55-75 years. Respir Med. 2006;100:658–665. doi: 10.1016/j.rmed.2005.08.003. [DOI] [PubMed] [Google Scholar]
- 11.Gibbons WJ, Fruchter N, Sloan S, Levy RD. Reference values for a multiple repetition 6-minute walk test in healthy adults older than 20 years. J Cardiopulm Rehabil. 2001;21:87–93. doi: 10.1097/00008483-200103000-00005. [DOI] [PubMed] [Google Scholar]
- 12.Chetta A, Zanini A, Pisi G, Aiello M, Tzani P, Neri M, et al. Reference values for the 6-min walk test in healthy subjects 20-50 years old. Respir Med. 2006;100:1573–1578. doi: 10.1016/j.rmed.2006.01.001. [DOI] [PubMed] [Google Scholar]
- 13.Alameri H, Al-Majed S, Al-Howaikan A. Six-min walk test in a healthy adult Arab population. Respir Med. 2009;103:1041–1046. doi: 10.1016/j.rmed.2009.01.012. [DOI] [PubMed] [Google Scholar]
- 14.Poh H, Eastwood PR, Cecins NM, Ho KT, Jenkins SC. Six-minute walk distance in healthy Singaporean adults cannot be predicted using reference equations derived from Caucasian populations. Respirology. 2006;11:211–216. doi: 10.1111/j.1440-1843.2006.00820.x. [DOI] [PubMed] [Google Scholar]
- 15.Choe KH, Park YJ, Cho WK, Lim CM, Lee SD, Koh YS, et al. The effect of pulmonary rehabilitation in patients with chronic lung disease. Tuberc Respir Dis. 1996;43:736–745. [Google Scholar]
- 16.Kim C, Park YB, Mo EK, Choi EH, Nam HS, Lee SS, et al. Predicting oxygen uptake for men with moderate to severe chronic obstructive pulmonary disease. Tuberc Respir Dis. 2008;64:433–438. [Google Scholar]
- 17.Kim YS, Byun MK, Jung WY, Jeong JH, Choi SB, Kang SM, et al. Validation of the Korean version of the St. George's respiratory questionnaire for patients with chronic respiratory disease. Tuberc Respir Dis. 2006;61:121–128. [Google Scholar]
- 18.Lee JH, Shin HI, Jeong YS. Reliability of 6-minute walk test in stroke patients. J Korean Geriatr Soc. 2005;9:39–44. [Google Scholar]
- 19.American Thoracic Society. Standardization of spirometry, 1994 update. Am J Respir Crit Care Med. 1995;152:1107–1136. doi: 10.1164/ajrccm.152.3.7663792. [DOI] [PubMed] [Google Scholar]
- 20.Ben Saad H, Prefaut C, Tabka Z, Mtir AH, Chemit M, Hassaoune R, et al. 6-minute walk distance in healthy North Africans older than 40 years: influence of parity. Respir Med. 2009;103:74–84. doi: 10.1016/j.rmed.2008.07.023. [DOI] [PubMed] [Google Scholar]
- 21.Al-Hazzaa HM. Prevalence of physical inactivity in Saudi Arabia: a brief review. East Mediterr Health J. 2004;10:663–670. [PubMed] [Google Scholar]
- 22.King B, Cotes JE. Relation of lung function and exercise capacity to mood and attitudes to health. Thorax. 1989;44:402–409. doi: 10.1136/thx.44.5.402. [DOI] [PMC free article] [PubMed] [Google Scholar]