

Abstract
We present a case of symptomatic perihepatic adhesions, which developed after a pregnancy complicated by hemolysis, elevated liver enzymes and low platelet (HELLP) syndrome, in which a subcapsular liver hematoma occurred. Our patient presented with complaints of persistent, severe right-sided upper abdominal pain. The complaints developed gradually, one year after a pregnancy that had been complicated by HELLP syndrome with a subcapsular liver hematoma. The hematoma had resolved spontaneously. An upper-abdominal magnetic resonance imaging revealed a density between liver and diaphragm at the site of the former subcapsular hematoma, suspect of perihepatic adhesions. The presence of perihepatic adhesions was confirmed during a laparoscopy and treated by adhesiolysis in the same session. The adhesions may have developed in response to the degradation process of the subcapsular liver hematoma during conservative treatment. This case of perihepatic adhesions may therefor be the first presentation of a long term sequel of subcapsular liver hematoma in HELLP syndrome.
Keywords: Hemolysis, elevated liver enzymes and low platelet syndrome; Liver; Haematoma; Long-term effects; Adhesions; Tissue
Core tip: This case of perihepatic adhesions may be the first presentation of a long term sequel of subcapsular liver hematoma in hemolysis, elevated liver enzymes and low platelet syndrome, which occured in pregnancy.
INTRODUCTION
Subcapsular liver hematoma is a rare but severe complication of the hemolysis, elevated liver enzymes and low platelet (HELLP) syndrome in pregnancy, with a reported incidence of 0.9% in a series of 442 pregnancies complicated by HELLP syndrome[1]. To the best of our knowledge, there are no reports on long-term sequels of subcapsular liver hematoma after HELLP syndrome[2].
CASE REPORT
A 29-year-old primipara presented with complaints of persistent, severe right -sided upper abdominal pain during deep inspiration, physical exercise and on local pressure. These complaints had developed gradually after giving birth one year earlier. This pregnancy had been complicated by HELLP syndrome with a subcapsular liver hematoma sized 20 cm × 5 cm, which had resolved spontaneously.
At current presentation, liver function tests were normal. She assured having never experienced signs suggestive of sexually transmitted diseases or pelvic inflammatory disease (PID). She had never undergone intra-abdominal interventions. An upper-abdominal magnetic resonance imaging revealed a density between liver and diaphragm at the site of the former subcapsular hematoma, suspect of perihepatic adhesions (Figure 1). She was referred to the hepatobiliary surgeon, who performed a laparoscopy and confirmed the presence of a thick adhesion between liver segment V/VIII and the diaphragm (Figure 2). Adhesiolysis was performed in the same session by monopolar diathermia and sharp dissection, followed by the instillation of 1.5 L Adept (4% icodextrin solution) into the peritoneal cavity to prevent the formation of new adhesions. On follow-up until three years post-surgery, she was free of symptoms.
Figure 1.

T2 weighted coronal magnetic resonance imaging image of subcapsular liver hematoma. The arrows indicate a hyperdense area suggestive of the subcapsular liver hematoma.
Figure 2.
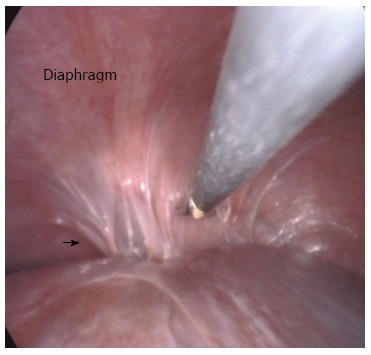
Laparoscopy image of perihepatic adhesions. The arrow indicates the location of the perihepatic adhesions to the diaphragm that were found during laparoscopy.
DISCUSSION
Clinical symptoms and imaging in our patient suggested the presence of perihepatic adhesions subsequently confirmed by laparoscopy. Adhesion formation is believed to be promoted by the inflammatory response to mesothelial injury, resulting from subcapsular liver parenchymal necrosis as part of the HELLP syndrome in our patient. Blood and other necrotic material are well-known triggers of inflammation[3]. Therefore, the formation of perihepatic adhesions in our patient may have been triggered by the degradation process of the resolving subcapsular liver hematoma. The aspect of the adhesion found in our patient differed clearly from that found in Fitz-Hugh-Curtis syndrome, occurring as a complication of PID.
This case may well be the first report of a long-term hepatic sequel of a subcapsular liver hematoma complicating HELLP syndrome. Perihepatic adhesions must be suspected in patients with complaints of persistent right-sided upper abdominal pain after conservative treatment of a liver hematoma. Biochemical markers such as liver function tests are expected to be normal in these patients and are therefore not of diagnostic value, however imaging studies can be suggestive of the presence of perihepatic adhesions. Key in confirming the diagnosis of perihepatic adhesions seems to be laparoscopy, which also enables immediate adhesiolysis as an effective therapeutic modality.
COMMENTS
Case characteristics
The authors present a case of symptomatic perihepatic adhesions, which developed after a pregnancy complicated by hemolysis, elevated liver enzymes and low platelet (HELLP) syndrome in which a subcapsular liver hematoma occurred.
Clinical diagnosis
The patient presented with complaints of persistent, severe right-sided upper abdominal pain.
Differential diagnosis
The complaints developed gradually, one year after a pregnancy that had been complicated by HELLP syndrome with a subcapsular liver hematoma.
Imaging diagnosis
An upper-abdominal magnetic resonance imaging revealed a density between liver and diaphragm at the site of the former subcapsular hematoma, suspect of perihepatic adhesions.
Treatment
Adhesiolysis was performed in the same session by monopolar diathermia and sharp dissection, followed by the instillation of 1.5 L Adept (4% icodextrin solution) into the peritoneal cavity to prevent the formation of new adhesions.
Experiences and lessons
Key in confirming the diagnosis of perihepatic adhesions seems to be laparoscopy, which also enables immediate adhesiolysis as an effective therapeutic modality.
Peer review
The authors describes for the first time a long-term hepatic sequel of a subcapsular liver hematoma complicating HELLP syndrome. It is suitable for publication as a case report observation.
Footnotes
P- Reviewers: Ni Y, Resende R S- Editor: Zhai HH L- Editor: A E- Editor: Wang CH
References
- 1.Sibai BM, Ramadan MK, Usta I, Salama M, Mercer BM, Friedman SA. Maternal morbidity and mortality in 442 pregnancies with hemolysis, elevated liver enzymes, and low platelets (HELLP syndrome) Am J Obstet Gynecol. 1993;169:1000–1006. doi: 10.1016/0002-9378(93)90043-I. [DOI] [PubMed] [Google Scholar]
- 2.van Pampus MG, Aarnoudse JG. Long-term outcomes after preeclampsia. Clin Obstet Gynecol. 2005;48:489–494. doi: 10.1097/01.grf.0000160316.67359.3d. [DOI] [PubMed] [Google Scholar]
- 3.Lauder CI, Garcea G, Strickland A, Maddern GJ. Abdominal adhesion prevention: still a sticky subject? Dig Surg. 2010;27:347–358. doi: 10.1159/000314805. [DOI] [PubMed] [Google Scholar]